
Jahanbakhsh Pourahangarian1, Babak Masoumi2 , Amir Masoud Hashemian3, Farahnaz Bidari Zerepoosh4 and Hojjat Derakhshanfar4*
1Department of Educational Research, Tonekabon Branch, Islamic Azad University, Tonekabon, Iran.
2Department of Emergency Medicine, Isfahan University of Medical Sciences, Isfahan, Iran.
3Department of Emergency Medicine, Imam Reza Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
4Shahid Beheshti University of Medical Sciences , Tehran , Iran
DOI : https://dx.doi.org/10.13005/bpj/536
Abstract
Physicians’roleinreducinghealth care costsisobvious andundeniable. Therefore, the current studyseeks toSurvey management of residents’ awareness of the cost of hospital paraclinical measures. This studyused avalid and reliablequestionnaire to evaluate the residents’ awareness regarding thecost of tests,including CBC, ESR, U/A,troponin, chest radiography, ultrasound of abdomenand pelvis,CT scan of head.Any estimate in the range of25% ofactual pricewas considered as the correctestimate. Data was analyzed usingt-test,chi-square anddrawing Box Plot. Significancelevel was determined p< 0.05. 90residents(54.4% male) were studied. With the exception ofchest radiography(48/0 = p),averagecostsestimated byresidents in the diagnostic tests of CBC (p<0.0001), ESR (p<0.0001), UA (p<0.0001),troponin(p=0.004),ultrasound(p=0.01)and CTscan ofhead(p<0.0001) differed from theactual price. Also, theaverageerrorinestimating thecosts ofCBC, ESR, UA,troponin, chest radiography, ultrasoundand CTscan ofheadwas 243.6%, 798.2%, 229.8%, 22.3%, 5.7%, 35.1% and 56.1%,respectively.On average, only 24.3%of residentswere awareof thereal cost oflaboratoryfees. The resultsshowed that the management level information of assistantsof internalmedicine, surgery,pediatrics, obstetricsandemergency medicineaboutthe cost of paraclinicalmeasuresis low and the level of education regardingawarenessof these costsis inadequate.
Keywords
Medical Expenses; DiagnosticTests; Residents’ Estimates
Download this article as:| Copy the following to cite this article: Pourahangarian J, Masoumi B, Hashemian A. M, Zerepoosh F. B, Derakhshanfar H. Survey Management of Residents’ Awareness of the Cost of Hospital Paraclinical Measures. Biomed Pharmacol J 2014;7(2) |
| Copy the following to cite this URL: Pourahangarian J, Masoumi B, Hashemian A. M, Zerepoosh F. B, Derakhshanfar H. Survey Management of Residents’ Awareness of the Cost of Hospital Paraclinical Measures. Biomed Pharmacol J 2014;7(2). Available from: http://biomedpharmajournal.org/?p=3237 |
Introduction
Costsof healthsystemsaround the worldare increasinglyon the rise and have allocated a significant shareofcountries’Gross National Product to itself(1-3). Risingcostshas led to the increase infinancial burdenimposed onpeople, so thatfamilies, particularlyvulnerable groups, are forcedtocutother essentialexpenses in order tomeettheirmedical expenses(4).this matter hasled toa decline inthe terms ofhousehold welfareandquality of life(5).Health costs, due tothe reducedsavings and less allocation ofhousehold incometo otheruses, especiallyitems likeproperfoodoreducation, which is ashuman capital accumulation(6), reduces householdproductivitypower asthe keyfactor innationalproduction process.In the meantime, doctors whoareundoubtedly oneof theimportant elements ofthe health system play asignificant rolein cost control andlargelydetermine thepatient’s health carecosts(7-8).In developed countries, the importance of this matter was realized long agoandphysicianswereeducatedabout themedical expenses, to the extent thatthesetrainingshave beenmandatoryin some casesand apart of thecurriculum. However,studiesconductedinthesecountries indicatethat physicians have lowknowledgeaboutthe diagnostic and therapeuticcosts(1, 9-13) .Our countryisnot excluded from facing thehigh cost ofhealthcareand despitecertaineconomic and politicalconditionsandfinancial constraintsatpresent,optimizing theuse ofhealthbudgets is needed more than ever.So, thephysicians’ awareness regarding thecost ofdiagnosisand treatment measures appliedfortheir patientsisundoubtedlyan important step inachieving thisgoal. The aimof this studyis to assess thelevel of awarenessoflimitedcommunityofdoctors to thecost ofparaclinicalproceduresthatare commonlyperformed.Becauseresidentshavea prominent roleinthe treatment of patientsin university hospitals, and also are futurephysicians, the populationstudied in thisresearchwas considered residents ofinternal medicine, surgery, obstetrics,pediatrics andemergency medicine.
Methodology
This studyisacross-sectional one which aims to investigate the awarenessof allresidentsininternal medicine, surgery, obstetrics and gynecology,pediatrics andemergency medicine ofImamHussain(AS). In order toachieve theobjectives ofthisresearch,questionnaire usedbyJune A.Leeet al. (14)was translated under the supervisionoftwo specialistsin emergencymedicine and aepidemiologistandits validitywas verifiedby makingsome changesandits reliabilitywasproven by usingCronbach’s alpha coefficient(α=0.705). The questionnairewasdesigned inthree parts. The first partcontainsbasicdemographicdataof residents, such asage, sex,field of study,work experiencebefore starting theresidency, education level, history ofprior educationandsource of awarenessof test costs. The second partconsists ofquestionsabout thecost of4 casesoflaboratory tests(CBC, ESR, U/A,troponin) 3 cases ofimagingmeasures(chest radiography, ultrasound of abdomenand pelvis, CT scan ofhead). Residents recorded their estimated prices in each case quantitatively. The third part includes 4 Qualitative questions to assess the residents’ attitudes toward the need for awareness of expenses. In the present study, the awareness of residents in internal medicine, surgery, obstetrics and gynecology, and pediatrics were measured, because these specialties use routine paraclinical measures more than others. We went to residents’ classrooms in different days to access them and gavethem questionnaires in quiet and favorable conditions and 30 minutes to complete. List of priceswas also provided from laboratoryandradiology department. The prices are as follows: CBC: 12.000 Rials/ U/A: 8.500 Rials/ ESR: 4.000 Rials/ troponin: 17.8500 Rials/chest radiography: 87.800 Rials/ ultrasound of abdomenand pelvis: 168,600 Rials/ CT scan of head: 300.000 Rials.Datafrom thequestionnaireswereentered intoSPSS 21.0 andthen examined descriptively and analyticallyusingSTATA 11.0program. The possibledifferencesin averagecostsestimated byresidents with real costs were examined using thet-test. In present study, any estimate in the range of25% ofactual price was considered as the correctestimate.Upper and lowerestimates were defined as underestimate overestimate, respectively. Residents’attitudes were divided intoproper(correct answer to at least threequestions) and improper (correct answer at leasttwoquestions)groups. Then, therelationship betweenresidents’ attitudes anddemographic factorswere examined usingchi-square tests. Box Plot was drawn to portray the residents’ awareness aboutthecost of tests.P- Valueless than0.05 was set assignificance level.
Results
In this study, 90 residents (54.4% male) were studied including 50 (55.5%) emergency medicine residents, 12 (13.3%) internal medicine residents, 16 (17.8%), surgery residents, 6 (6.7%), 6 (6.7%) obstetricresidents and 6 (6.7%) pediatric residents. Their mean and standard deviation of age was estimated 32.7 ± 3.9. Of these individuals, only five residents (5.6%) have been trained in diagnostic and therapeutic costs and the mean and standard deviation of training timewas equal to 6.8 ± 3.8 h. It is worth noting that none of the participating residents was evaluated during the residency period about the rate of information on health care costs (Table 1).
Table1: Demographic characteristics ofparticipantsin current study
| Variable | Frequency | Percentage | |
| Age | 29-35 | 69 | 81.2% |
| 36-45 | 16 | 18.8% | |
| Sex | Male | 49 | 54.4% |
| Female | 41 | 45.7% | |
| Specialty | Emergency Medicine | 50 | 55.5% |
| Internal | 12 | 13.3% | |
| Surgery | 16 | 17.8.% | |
| Obstetrics | 6 | 6.7% | |
| Pediatrics | 6 | 6.7% | |
| Level of Education | Year 1 | 32 | 35.6% |
| Year 2 | 28 | 31.1% | |
| Year 3 | 27 | 30.0% | |
| Year 4 | 3 | 3.3% | |
| Work Experience | 2 years ≥ | 51 | 59.3% |
| 3-10 years | 27 | 31.4% | |
| < 10 years | 3 | 9.3% | |
| History ofeducationinthe field ofhealthcare costs | No | 585 | 94.4% |
| Yes | 5 | 5.6% |
46 (51.1%%) residents stated that no questions have been exchanged on health care costs in their previous 20 visits by Atend, patients, resident him/herself or other people (nurses, auxiliary nurses, etc.). Mean and standard deviation of the number of times thatAtend, patients, resident him/herself and others have spoken regarding their treatment costs was 5.4 ±6.4, 8.3 ± 5.8,6.8 ± 6.3 and 6.7 ± 5.3, respectively that had no significant difference with each other (p=0.18). The most important awareness sources of residentsabout health care costs are other physicians (30.3%), other people (15.6%), physicians and pharmacists (5.6%, Internet (4.4%), pharmacists (3.3%) and articles (1.1%), respectively (Figure 1).
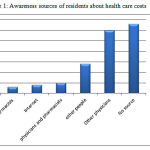 |
Figure 1: Awareness sources of residentsabout health care costs
|
The meanand standard deviation ofcostsestimated byresidentsindiagnostic CBC (p<0.0001), ESR (p<0.0001), UA (p<0.0001),troponin(p=0.004), chest radiography (p=0.48)ultrasound of abdomen and pelvis (p=0.01)and CTscan ofhead(p<0.0001) was 4136.1±3145.1, 3592.7±3600, 2803.4±1742.3, 14028.9±11718.1, 9280.7±6542.6, 22880.9±21872.8 and 47000.0±25822.4, respectively, that hada significant difference betweenthe actual price. AsFig2 shows, except residents’ estimates for chestradiography which were close to actual price and the price of troponinwhich was underestimated, the prices of remaining laboratorytestswere overestimated. Star symbolinfigure representsthe actualcost ofdiagnostictests.
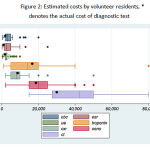 |
Figure 2: Estimatedcosts byvolunteerresidents, * denotes the actualcost ofdiagnostic test
|
According to thestudy, the estimatedcost ofdiagnostic testswithin 25percent ofactualcosts was considered as the correct estimate. Accordingly, the averageerrorsinestimating thepricesof CBC, ESR, UA,troponin, chest radiography, ultrasound of abdomen and pelvisand CTscan ofhead were observed 243.6%, 798.2%, 229.8%, 22.3%, 5.7%, 35.1% and 56.1%, respectively. Ascan be seen,the prices of ESR, CBCandUAestimated by residents arevery different from theactualprice. Table 2showsthe responseofphysicians. Mostresidentswere unawareof thetrue priceof CBC, so that80(88.8%) residentsoverestimated its price. Similarresultswere also obtainedin the prices of ESR andUA; meaning that 88 (98.8%) and 77 (85.6%) residents overestimated their prices. But itwas different abouttroponin. Mostresidents(46.7%) underestimated its price. While34(37.8%) residentsestimated the costof radiography equal and 62.2% overestimated thecost ofCT scan. Based on theanalyses, on average,only24.3%ofresidentswere awareof thereal cost oflaboratory fees.
Table 2: Distribution of physicians’ awareness of thecostoflaboratory testsandimagingtests
| Variable | Estimate | Frequency | Percentage |
| CBC | Underestimated | 2 | 2.2% |
| Equal to actual price | 8 | 8.9% | |
| Overestimated | 80 | 88.8% | |
| ESR | Underestimated | 1 | 1.1% |
| Equal to actual price | 1 | 1.1% | |
| Overestimated | 88 | 98.8% | |
| UA | Underestimated | 1 | 1.1% |
| Equal to actual price | 12 | 13.3% | |
| Overestimated | 77 | 85.6% | |
| Troponin | Underestimated | 42 | 46.7% |
| Equal to actual price | 32 | 35.6% | |
| Overestimated | 16 | 17.8% | |
| CXR | Underestimated | 29 | 32.2% |
| Equal to actual price | 34 | 37.8% | |
| Overestimated | 27 | 30.0% | |
| Ultrasoundof the abdomenand pelvis | Underestimated | 15 | 16.7% |
| Equal to actual price | 42 | 46.7% | |
| Overestimated | 33 | 36.6% | |
| Head CT | Underestimated | 11 | 12.2% |
| Equal to actual price | 23 | 25.6% | |
| Overestimated | 56 | 62.2% |
Investigating the responses of research unit indicated that more residents possessed a proper perspective on the necessity of promoting physicians’ awareness of healthcare costs and knowing the costs involved in their clinical decisions. Of 4 questions, 83 (92.2%) residents answeredat least three questions correctly (mean and standard deviation 3.5 ± 0.9), indicatingthat theattitude ofresidentsisdesirable. But their attitude didn’t affect their awareness of the price of any diagnostic tests of CBC (p=0.99), ESR (p=0.99), UA (p=0.62), troponin (p=0.89), chest radiograph (p=0.25), ultrasoundof abdomen and pelvic(p=0.22) and CT scan of head (p=0.6)(table 3).
Table 3: Estimatedcostsbased onresidents’ attitudes onhealth care costs
| Variable | Estimate | Improper attitude | Proper attitude | P |
| CBC | Overestimated | (0.0%) 0 | (100%) 2 | 99.0 |
| Equal to actual price | (0.0%) 0 | (100%) 8 | ||
| Underestimated | (8.8%) 7 | (2.91%) 73 | ||
| ESR | Overestimated | (0.0%) 0 | (100%) 1 | 99.0 |
| Equal to actual price | (0.0%) 0 | (100%) 1 | ||
| Underestimated | (0.8%) 7 | (0.92%) 81 | ||
| UA | Overestimated | (0.0%) 0 | (100%) 1 | 62.0 |
| Equal to actual price | (0.0%) 0 | (100%) 12 | ||
| Underestimated | (1.9%) 7 | (9.90%) 70 | ||
| Troponin | Overestimated | (5.9%) 4 | (5.90%) 38 | 88.0 |
| Equal to actual price | (2.6%) 2 | (8.93%) 30 | ||
| Underestimated | (2.6%) 1 | (8.93%) 15 | ||
| CXR | Overestimated | (9.6%) 2 | (1.93%) 27 | 25.0 |
| Equal to actual price | (9.2%) 1 | (1.97%) 33 | ||
| Underestimated | (8.14%) 4 | (2.85%) 23 | ||
| Ultrasoundof the abdomenand pelvis | Overestimated | (0.20%) 3 | (0.80%) 12 | 22.0 |
| Equal to actual price | (8.4%) 2 | (2.95%) 40 | ||
| Underestimated | (1.6%) 2 | (9.93%) 31 | ||
| Head CT | Overestimated | (0.0%) 0 | (100%) 11 | 6.0 |
| Equal to actual price | (4.4%) 1 | (6.95%) 22 | ||
| Underestimated | (7.10%) 6 | (3.89%) 50 |
Discussion
Survey ofresidents’ awareness of financial burdenimposedon the patient’s clinical by paraclinical measures had a big differencewith theactual rate. On average, pricesestimated bymedicalresidentswere 176% greater than the actual costs. On theother hand, only estimating 24.3%of research units incurrent studywerecloser tothe real prices. Althoughresidents in the study had a properattitudetoward the knowledgeof fees, this proper attitudehas not caused them to improvetheir knowledge. One ofthe maincauses oflack of awareness inresidents is their source ofinformation.The mainsource of data forresidentsparticipating in thestudy is their colleagues, namely, other physicians. Becausephysicians, likeresidents, have a lowawarenessin this field. So avicious cycle has been created that not only doesnotimproveresidents’ awareness, but alsoincreasesthe chanceto confusethem.
The comparison of presentpaperwith the findings ofotherstudiesreflects the highconsistencyofourfindingswith each other. This means thatmostresearchersbelieve thatphysicians’ awareness ofhealth care costsis low(13-19).For example,Allanand his colleaguesshowedin asystematic reviewthat on average;only 31% ofdoctorsare able to estimatethe pricesin the rangeof 25-20 percent ofreal rates(19). The same policyis trueInotherstudies, so that the frequencyof accurate estimateof health carecosts is assessedbetween24-33% (14, 20). These findingstogether with theresultsof this studyindicatethe poorawarenessof physiciansaround the world aboutdiagnosis and treatment costs.
In a systematic review of Allen et al.(19)it was found that nationality, country, level of education, expertise, and physicians’ other demographic and basic factors have a little impact on their knowledge and the only factor affecting accurateestimates ofthe prices ofdrugs and paraclinical testsis their real prices. This means that expensive drugs are underestimated and inexpensive ones are overestimated. This issue has been confirmed in other studies (16, 20-21). The prices of cheap laboratory tests, such as CBC, UA and ESR, have been also overestimatedin our study, but the status of expensive tests was variable. So that the cost of troponin was underestimated and the costs of ultrasound and CT scan were overestimated. The cause of this differencecan beattributed to the fact thatImamHussainhospital is a public one and itscosts are lower thanprivate andsemi-privatesectors.If the cost ofimagingmeasureswerecalculatedbased onnon-publictariffs, thedifferencebetweenthis study andprevious studieswasnot created. Ascan be seen, percentage ofphysicians’ errorsinestimating thecosts ofexpensivediagnostic tests is less than cheaper tests whichisconsistentwith the findings ofotherstudies(21).This issue should be attributed to themethod of calculating theexact price, not to the physicians’ awareness, becauseexpensivediagnostictests have a larger 25percent range thancheaper ones.
Physicians’attitude towards the need forawarenessof the costsand to applythemin clinical practicehas been studiedinpreviousstudies (1, 13, 22) .For example,in thestudyof TekSehgalet al.physicians have known their awareness ofhealth care costsless, butthey have shown a strong desireto gainthis knowledge(20).In thestudyofBovieret al, conductedin Switzerland, 90% of physicians believed thatawarenessof the costsistheirresponsibility(23) . In our study,theattitude towardsresidents’ awareness ofhealth care costswas positive.Butitis clearthat physicians, despite the interest inhaving more awareness of health care costs, have a limited access totheseresources(9, 24).In the present study, the majority ofresidents(30.3%) receivethe informationfromother doctors, indicating thelack ofofficialinforming. However,theprevious studies showed theeffectiveand useful role of teaching healthcare expenses in reducing health systemcosts andreducescosts30-10percent.
(25-26). Therefore, it seems essential to plan trainingprograms in order to improve physicians’ awarenessat alllevels inourcountry.
One limitationofthe present study is the lowfrequency ofobstetric andpediatricresidents. Due to the low frequency of them, it is impossible to make decisions regarding theimpactof major onresidents’ awareness ofhealth care costs. Therefore,it is recommendedthis point to be considered in subsequent research and acceptablevolumeofdifferent specialties to beevaluated. Anotherweaknessofthis study is the lack of examining the residents’ awareness of drugcosts. Since drug therapyisan important part ofhospital costs, the necessity to pay attention tothis issue is obvious. But since the purpose of the present study was to assess the residents’ awareness of diagnostic tests, their awareness of drug costs was not investigated. Also, due to the higher cost of laboratory measures in the private centers, if the awareness of physicians’ working in these centers could also be checked, more comprehensive and more accurate results would be obtained from the study. Unfortunately, it was not possible to study the awareness of physicians’ working in private centers.
Conclusion
The resultsshowed that themanagement level information of residentsof internalmedicine, surgery,pediatrics, obstetricsandemergency medicineaboutthe cost ofclinicalmeasuresis low andthe level of education regardingawarenessof these costsis inadequate.Accordingly, it can be said that educational systemhas poorlytrainedmedicalresidentsinthe field ofmedical expenses. Yet,residentsacknowledgedthe need tobe aware of thecostsandto applythisinformation whentreating patients andexpresseda strong desireto havemore informationon this subject.
References
- Korn LM, Reichert S, Simon T, Halm EA. Improving physicians’ knowledge of the costs of common medications and willingness to consider costs when prescribing. Journal of general internal medicine. 2003;18(1):31-7.
- Tierney WM, Miller ME, McDonald CJ. The effect on test ordering of informing physicians of the charges for outpatient diagnostic tests. New England Journal of Medicine. 2005;322(21):1499-504.
- Rao VM, Levin DC. The overuse of diagnostic imaging and the choosing wisely initiative. Annals of internal medicine. 2012;157(8):574-6.
- Chauvin P, Simonnot N. Access to health care for vulnerable groups in the European Union in 2012. 2012.
- Kini R, editor Challenges in Building a Community Health Information Exchange in a Complex Environment. 6th European Conference on Information Management and Evaluation; 2012: Academic Conferences Limited.
- Mannan H, MacLachlan M, McVeigh J. Core concepts of human rights and inclusion of vulnerable groups in the United Nations Convention on the rights of persons with disabilities. ALTER-European Journal of Disability Research/Revue Européenne de Recherche sur le Handicap. 2012;6(3):159-77.
- Fenton JJ, Jerant AF, Bertakis KD, Franks P. The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality. Archives of internal medicine. 2012:archinternmed. 2011.1662 v1.
- Emanuel EJ. Where are the health care cost savings? JAMA: the journal of the American Medical Association. 2012;307(1):39-40.
- Jansson S, Anell A. The impact of decentralised drug-budgets in Sweden–a survey of physicians’ attitudes towards costs and cost-effectiveness. Health policy. 2006;76(3):299-311.
- Barnett ML, Christakis NA, O’Malley J, Onnela J-P, Keating NL, Landon BE. Physician patient-sharing networks and the cost and intensity of care in US hospitals. Medical care. 2012;50(2):152-60.
- Ryan M, Yule B, Bond C, Taylor R. Scottish general practitioners’ attitudes and knowledge in respect of prescribing costs. BMJ: British Medical Journal. 1990;300(6735):1316.
- Ryan M, Yule B, Bond C, Taylor RJ. Do physicians’ perceptions of drug costs influence their prescribing? Pharmacoeconomics. 1996;9(4):321-31.
- Reichert S, Simon T, Halm EA. Physicians’ attitudes about prescribing and knowledge of the costs of common medications. Archives of Internal Medicine. 2000;160(18):2799.
- Lee JA, Chernick L, Sawaya R, Roskind CG, Pusic M. Evaluating Cost Awareness Education in US Pediatric Emergency Medicine Fellowships. Pediatric emergency care. 2012;28(7):655-75.
- Schilling UM. Cost awareness among Swedish physicians working at the emergency department. European Journal of Emergency Medicine. 2009;16(3):131-4.
- Allan GM, Innes GD. Do family physicians know the costs of medical care? Survey in British Columbia. Canadian family physician. 2004;50(2):263-70.
- Innes G, Grafstein E, McGrogan J. Do emergency physicians know the costs of medical care. CJEM. 2000;2(2):95-102.
- Graham JD, Potyk D, Raimi E. Hospitalists’ awareness of patient charges associated with inpatient care. Journal of Hospital Medicine. 2010;5(5):295-7.
- Allan GM, Lexchin J. Physician awareness of diagnostic and nondrug therapeutic costs: A systematic review. International journal of technology assessment in health care. 2008;24(2):158-65.
- Tek Sehgal R, Gorman P. Internal Medicine Physicians’ Knowledge of Health Care Charges. Journal of Graduate Medical Education. 2011;3(2):182-7.
- Allan GM, Lexchin J, Wiebe N. Physician awareness of drug cost: a systematic review. PLoS medicine. 2007;4(9):e283.
- McGuire C, King S, Roche-Nagle G, Barry M. Doctors’ attitudes about prescribing and knowledge of the costs of common medications. Irish journal of medical science. 2009;178(3):277-80.
- Bovier PA, Martin DP, Perneger TV. Cost-consciousness among Swiss doctors: a cross-sectional survey. BMC health services research. 2005;5(1):72.
- Anderson GM, Lexchin J. Strategies for improving prescribing practice. CMAJ: Canadian Medical Association Journal. 1996;154(7):1013.
- Snyder-Ramos S, Bauer M, Martin E, Motsch J, Böttiger B. Accessible price lists at the anaesthesiologist’s workplace enhance cost consciousness as a part of process and cost optimization]. Der Anaesthesist. 2003;52(2):154-9.
- Seguin P, Bleichner J, Grolier J, Guillou Y, Mallédant Y. Effects of price information on test ordering in an intensive care unit. Intensive care medicine. 2002;28(3):332-5.

