
Manuscript accepted on :
Published online on: 23-12-2015
Plagiarism Check: Yes
N. P. Prabhu, Vijay Ebenezer* and R. Balakrishnan
Department of Oral and Maxillofacial Surgery, Sree Balaji Dental College and Hospital, Bharath University, Chennai, 600100, India.
DOI : https://dx.doi.org/10.13005/bpj/477
Download this article as:| Copy the following to cite this article: Prabhu N. P, Ebenezer V, Balakrishnan R. Ameloblastoma: Report of two Cases and A Brief Literature Review. Biomed Pharmacol J 2014;7(1) |
| Copy the following to cite this URL: Prabhu N. P, Ebenezer V, Balakrishnan R. Ameloblastoma: Report of two Cases and A Brief Literature Review. Biomed Pharmacol J 2014;7(1). Available from: http://biomedpharmajournal.org/?p=2923 |
Introduction
Ameloblastoma is reported to constitute about 1-3% of tumours and cysts of the jaws.(1-3) The tumour is by far more common in the mandible than in the maxilla and shows predilection for various parts of the mandible in different racial groups.(4) The relative frequency of the mandible to maxilla is reported as varying from 80–20% . It often presents as a slow growing, painless swelling, causing expansion of the cortical bone, perforation of the lingual and or buccal plates and infiltration of soft tissue. There is often delay in the diagnosis because of its slow-growing nature.(5) Ameloblastoma of the jaws is the most commonly encountered odontogenic tumour in Africa(6-9) and Asia,(10,11) but the second most common odontogenic tumour in North and South America.(12–14) The aim of the present study was to critically review the pertinent literature and determine the most appropriate method of treatment for ameloblastomas.
Case Report
Case 1
A 66-years-old female patient sought treatment at the Oral and maxillofacial department due to a localized swelling and asymptomatic intraoral lesion on the posterior region of the left inferior alveolar ridge. The lesion exhibited no bleeding and a slow and progressive evolution of approximately six months; however, the time since the lesion was noticed was undetermined. No signs of facial asymmetry were noted on an extra-oral physical examination. Patient was edentulous and used upper and lower dentures. A localized intraosseous cavitary lesion was observed on the left inferior alveolar ridge that was approximately 30 mm in diameter and below the mucosa and that had an oval shape, a wrinkled and ulcerated surface and a soft and firm consistency. The edges of the lesion were irregular and undefined. No palpable lymph nodes were noticed on palpation of the submaxillary and cervical chains. Following clinical examination, the patient was subjected to radiographic examination and computed tomography , which revealed the location of the tumor. Incisional biopsy was performed, and histopathology confirmed the final diagnosis of multicystic intraosseous ameloblastoma with a plexiform pattern. The patient underwent a surgical procedure for ressection of the lesion with complete removal of the tumor and safety margins of approximately 15 mm, which were tumor-free. To date, this patient remains free of any signs of recurrence following clinical and imaging examinations periodically and she has received prosthetic rehabilitation with functional and aesthetic satisfaction.
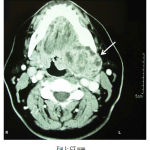 |
Figure 1: CT scan |
Case 2
A 40-years-old male patient sought treatment at Oral and maxillofacial department, complaining of a localized and asymptomatic swelling in the region of the right posterior mandibular body. The patient was unable to report the time evolution of the lesion, and the extra-oral physical examination was normal. However, during an intra-oral examination, a discrete nodular mass of approximately 5 mm in diameter was noticed on the right inferior vestibular alveolar mucosa (apical region of the first premolar), with a smooth surface, normal color, irregular margins and a fibrous consistency on palpation. Radiographic examination revealed a radiolucent lesion with irregular margins in the right inferior premolar region that was associated with an area of bone destruction, with invasion of the mandibular canal and preservation of the basal cortex. After incisional biopsy was confirmed the diagnosis of multicystic ameloblastoma with a plexiform pattern, and the patient was subjected to a surgical procedure for the segmental resection of the lesion, with safety margins of approximately 15 mm. The surgical specimen was again submitted to histopathological analysis, which verified that the margins were tumor-free. Surgical resection of the right mandible was then performed, preserving only the condyle and the coronoid process on the right side, with reconstruction plate fixation . After 24 months of follow-up, the patient currently undergoes 6-month follow-ups and shows no signs of tumor recurrence.
 |
Figure A: Affected site
|
 |
Figure B: Ressected mandible |
 |
Figure C: Reconstruction plate
|
Discussion
Ameloblastoma originate from epithelial remnants of dental embryogenesis, without the participation of the odontogenic ectomesenchyme(15). This tumor was initially considered to be a type of odontogenic cyst and was first described by cusak(16) in a case report of mandibulectomy, and later reported by Broca (1866) and Falksson (1879). The classic study by Malassez (1885) ultimately differentiated the tumor from other types of cyst and gave it the name adamantinoma. The term ameloblastoma was later suggested by Ivy & Churchill (1960), based on an analysis of the odontogenic epithelium involvement in the tumor origin. According to the literature, potential sources of this specialized epithelium may also include embryonic odontogenic rests (rests of Malassez and rests of Serres), the epithelial lining of odontogenic cysts (especially the dentigerous cyst) and basal cells from the oral mucosa(17). However, the trigger for neoplastic transformation of these epithelial structures remains unknown (18). Although a wide variation in the range of ages can be observed, ameloblastoma primarily affects young adults between the fourth and fifth decades of life. Unlike the observation in the first case report (Case 1), the mean age is most commonly between 35 and 45 years. Ameloblastoma is usually included in the differential diagnosis according to the presentation of the patients history and clinical characteristics. The diagnosis of ameloblastoma is suggested by nonspecific radiographic findings and a thorough locoregional physical examination. Nevertheless, a definitive diagnosis is only obtained through a histopathological exam . The persistent growth pattern (localized and infiltrative to the maxillofacial region) and the ability to produce pronounced deformities are clinical characteristics that contribute to the possible identification of ameloblastomas. The typical ameloblastoma begins as a slowly destructive asymptomatic and intraosseous expansion, being a lesion that tends to expand and infiltrate, rather than perforate the bone. However, the diagnosis can also be suggested through a routine radiographic examination (19). As observed in the above mentioned cases, unless the tumor becomes infected, it is rarely painful. When these tumors become symptomatic, the patient may experience pain or numbness, swelling, malocclusion, tooth mobility or secondary infection. Ameloblastomas can occur at any location in the mandible or maxilla, but the regions of the inferior molars and mandibular ramus are the most prevalent anatomical locations (80%)(20). Larger tumors may rupture the bone cortex and infiltrate adjacent soft tissues on the lingual surface of the mandible. When the tumor occurs in the maxilla, the posterior region is the most affected, and the evolution and invasion of the tumor may compromise the maxillary sinus and the orbit.
Ameloblastoma occur in distinct clinical and radiographic situations, which need to be considered separately due to therapeutic and prognostic differences. These tumors are classified as solid or multicystic (86% of cases), unicystic (13% of cases) or peripheral or extraosseous (approximately 1% of cases). In addition, rare malignant subtypes with metastasis can occur (malignant ameloblastoma and ameloblastic carcinoma). This distinction is important because the treatment for a unicystic lesion can be more conservative due to its less aggressive behavior and usually smaller size than the solid or multicystic variation(21). The most common radiographic findings are unilocular and multilocular masses, septation, association with unerupted teeth, loss of lamina dura and root resorption. The uni- and multilocular radiographic patterns result in the traditional division of ameloblastomas into the solid and cystic types. In solid or multicystic ameloblastoma, a multilocular radiolucent lesion with undefined borders is the most characteristic radiographic aspect (soap bubble or honeycomb appearance). In the unicystic type, the lesions usually appear as radiolucent areas with relatively well-defined borders that surround the crown of an impacted inferior third molar, resembling a dentigerous cyst. The peripheral extraosseous ameloblastoma are rare, and usually the peripheral ameloblastoma present themselves as painless, usually non-ulcerated lesions on the alveolar or gingival mucosa, which can be sessile or pedunculated and demonstrate a non-aggressive benign course. In general, unicystic and peripheral lesions do not invade the bone tissue, respond better to treatment and have low recurrence rates. Unlike most cases, neither of the cases reported in this article showed the characteristic radiolucent multilocular images on initial clinical examination. However, even when an ameloblastoma shows the typical expansive multilocular aspect, the differential diagnosis can include a variety of odontogenic and nonodontogenic lesions with similar radiographic characteristics (aneurysmal bone cyst, odontogenic keratocyst, ameloblastic fibroma, odontogenic myxoma, giant cell lesions and brown tumor of hyperparathyroidism). When the lesion presents with a cystic, unilocular and well-defined aspect, the differential diagnosis is typically of odontogenic keratocyst, dentigerous cyst, residual and radicular cysts or even a traumatic bone cyst. Additionally, peripheral ameloblastoma may resemble lesions such as fistulas (parulis), pyogenic granulomas, peripheral giant cell lesions and peripheral odontogenic fibromas(22). On rare occasions, ameloblastoma may exhibit malignant behavior and metastasize. However, the nomenclature for these tumors (malignant ameloblastoma and ameloblastic carcinoma) is still controversial. Both the nomenclature and the issue of malignancy in these neoplasms are problems that require lengthy discussions. Therefore, because these issues deserve special discussion, they will not be addressed in the present study. The histopathology of ameloblastomas basically consists of the proliferation of epithelial cells arranged in variable patterns, which may occasionally coexist in the same tumor. The most frequent histopathological patterns are the follicular and plexiform subtypes. Although rare, other histopathological patterns can also be observed, such as acanthomatous, granular cell, basal cell and desmoplastic. In the plexiform pattern, interdigitating cords and irregular masses of epithelial cells surrounding small amounts of stroma of the stellate reticulum can be observed. The granular cell pattern is an aggressive lesion with a significant tendency to recur, and the neoplastic epithelial component exhibits cells with a finely granular cytoplasm, resembling the cells of the granular cell tumor. The basal cell ameloblastoma is the least common type and is composed of nests of uniform basaloid cells. In contrast, the desmoplastic pattern exhibits the formation of a densely collagenized stroma with several fibrous septa. Clinical, imaging and histopathological examinations of the reported cases confirmed the diagnosis of a solid or multicystic ameloblastoma that contained histological features consistent with the plexiform pattern. Because infiltration between the trabeculae of spongeous bone can occur, the recommended treatment for solid or multicystic ameloblastoma consists of wide resection to prevent recurrences and the possible progression to malignancy. A high recurrence rate, particularly after conservative treatments, is not uncommon for this type of odontogenic tumor(23). Given these high recurrence rates, which vary between 50 and 90% after conservative treatment, several authors have supported surgical resection with safety margins for the treatment of solid or multicystic ameloblastomas and have advocated bone resection in the affected area with at least 15 mm of healthy adjacent tissue beyond the radiographic borders of the lesion , as performed in both of the above mentioned cases. The second patient is currently free of recurrences and was rehabilitated with reconstruction plate fixation , as well as reported in other cases . In addition to the low radiosensitivity of this neoplasm, the intraosseous location of the ameloblastoma prevents the use of radiotherapy as an effective therapeutic option because radiation increases the potential development of secondary tumors(24). To try to prevent disfigurement of the patient, smaller unicystic lesions can be treated solely with enucleation and curettage, but recurrence occurs in an average of 10 to 20% of cases. Similarly, peripheral ameloblastomas exhibit innocuous clinical behavior and can be treated more conservatively because the local recurrence rate is 10%. However, in all types of ameloblastomas, a thorough long-term clinical and radiographic follow-up is always recommended, and these follow-ups were performed in both of the above mentioned cases. Although clinical and imaging findings aid in the differential diagnosis, histopathological evaluation is essential for the definitive diagnosis of ameloblastomas. For successful treatment, early diagnosis and detection of the precise boundaries of the tumor are essential. However, due to the slow growth rate of these tumors and the ability to develop late recurrences, the recurrence events may occur several years after the initial primary tumor resection(25), and a long follow-up is recommended for patients diagnosed with this type of tumor, as performed in both reported cases in this study. Summarizing, ameloblastomas are uncommon benign odontogenic neoplasms that rarely become malignant. In most cases, radical surgery is the treatment of choice for solid or multicystic ameloblastoma. Although several articles have been published on the subject, little is known regarding the biological behavior of this tumor, and a careful clinical examination combined with a thorough imaging investigation to evaluate the general aspects of the lesions and its margins, as well as its internal architecture and its relationship to adjacent anatomical structures, can assist in treatment planning. These informations coupled with the histopathological confirmation of the diagnosis will allow for the selection of the best individual therapeutic approaches, increasing the treatment efficacy in patients diagnosed with this tumor.
References
- Jackson IT, Callan PP, Robert A. An anatomic classification of maxillary ameloblastoma as an aid to surgical treatment. J Craniomaxillofac Surg 1996; 24:230–6.
- Small LA, Waldron CA. Ameloblastoma of the jaws. Oral Surg Oral Med Oral Pathol 1955;8:281–97.
- Ajagbe HA, Daramola JO. Ameloblastoma: A survey of 199 cases in the University College Hospital, Ibadan, Nigeria. J Nat Med Assoc 1987;79:324–7.
- Adekeye EO. Ameloblastoma of the jaws: a survey of 109 Nigerian patients. J Oral Surg 1980;38:36–41.
- Gandhi D, You AF, Anthony M, MacDonald G, Brocklebank LM, Moos KF. Ameloblastoma: a surgeon’s dilemma. J Oral 140 Vohra F A, Hussain M, Mudassir M S Journal of Surgery Pakistan (International) 14 (3) July – September 2009 Maxillofac Surg 2006;64:10104.
- Odukoya O. Odontogenic tumours: analysis of 289 Nigerian cases. J Oral Pathol Med 1995;25:454–7.
- Arotiba JT, Ogunbiyi JO, Obiechina AE. Odontogenic tumours: a 15-year review from Ibadan, Nigeria. Br J Oral Maxillofac Surg 1997;35:363–7.
- ChidzongaMM, Lopez VM, Alverez AP. Odontogenic tumours; analysis if 148 cases in Zimbabwe. Cent Afr J Med 1996;42:158–61.
- Ladeinde AL, Ajayi OF, Ogunlewe MO, Adeyemo WL, Arotiba GT, Bamgbose BO, Akinwande JA. Odontogenic tumors: a retrospective analysis of 319 cases in a Nigerian teaching hospital. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:191–5.
- Wu PC, Chan KW.A survey of tumours of the jaw bone in Hong Kong Chinese. 1963–1982. Br J Oral Maxillofac Surg 1985;23:92–102.
- Lu Y, Xuan M, Takata T et al. Odontogenic tumors. A demographic study of 759 cases in a Chinese population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:707–14.
- Regezi JA, Kerr DA, Courtney RM. Odontogenic tumours: analysis of 706 cases. J Oral Surg1978;3 6:771–8.
- Daley TM, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumours and oral jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol 1994;77:276–80.
- Ochsenius G, Ortega A, Godoy L, Penafiel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases. J Oral Pathol Med 2002;31:415–20.
- Martinez, C. R.; Barros, R. M. G.; Oru., N. R.; Oliveira, J. G. P. & Monteiro, J. C. C. Ameloblastoma: estudo cl.nicohistopatol.gico. Rev. Cir. Traumatol. Buco-Maxilo-Fac., 8:55-60, 2008.
- Cusak, J. W. Report of the amputation of the portions of the lower jaw. Dubin Hosp. Rep., 4:1-38, 1827.
- Adekeye, E. O. & Lavery, K. M. Recurrent ameloblastoma of the maxillo-facial region. Clinical features and treatment. J. Maxillofac. Surg., 14:153-7, 1986.
- Olaitan, A. A.; Arole, G. & Adekeye, E. O. Recurrent ameloblastoma of the jaws. A follow-up study. Int. J. Oral Maxillofac. Surg., 27:456-60, 1998.
- Medeiros, M.; Porto, G. G.; Laureano Filho, J. R.; Portela, L. & Vasconcellos, R. H. Ameloblastoma em mand.bula. Rev. Bras. Otorrinolaringol., 74:478, 2008.
- Reichart, P. A.; Philipsen, H. P. & Sonner, S. Ameloblastoma: biological profile of 3677 cases. Eur. J. Cancer B Oral Oncol., 31B:86-99, 1995.
- Ord, R. A.; Blanchaert, R. H. Jr.; Nikitakis, N. G. & Sauk, J. J. Ameloblastoma in Children. J. Oral Maxillofac. Surg., 60:762-71, 2002.
- Martins, R.; Sobrinho, J.; Rapoport, A. & Rosa, M. Histopathologic features and management of ameloblastoma: study of 20 cases. Rev. Paul. Med.,117(4):171-4, 1999.
- Medeiros, M.; Porto, G. G.; Laureano Filho, J. R.; Portela, L. & Vasconcellos, R. H. Ameloblastoma em mand.bula. Rev. Bras. Otorrinolaringol., 74:478, 2008.
- Reichart, P. A.; Philipsen, H. P. & Sonner, S. Ameloblastoma: biological profile of 3677 cases. Eur. J. Cancer B Oral Oncol., 31B:86-99, 1995.
- Ferretti, C.; Polakow, R. & Coleman, H. Recurrent ameloblastoma: report of 2 cases. J. Oral Maxillofac. Surg., 58:800-4, 2000.

