
Ahmad Hematfar* and Mandana Shekarchian
Physical Education Department, Islamic Azad University, Borujerd, Iran.
DOI : https://dx.doi.org/10.13005/bpj/398
Abstract
The superiority of continuous active recovery on passive recovery has been completely specified. However, the time needed for such recovery is (20-60 minutes) and its intensity is not well controlled. One the other hand, after the majority of short-term exercises, a short-term recovery is need to return the athlete promptly to normal condition to have better performance. But, this type of recovery is not completely known in terms of duration, intensity and type of activity. The objective of the present study is to investigate the effect of short-term recovery (3 min) in replicated rock-climbing activities on blood lactate, LDH and CPK concentration of elite male rock-climbers. For this purpose, 10 elite male rock-climbers (age: 24±2.92 years, weight: 60±6.19 kg, height: 173±5.73 cm and BMI: 19±2.98) voluntarily participated in this study. Rock-climbers participated in a cross over study with an interval of 5 days in two trials, including four 2 min climbing activities with 3 min of passive recovery after each activity in the first experiment and 3 min of active recovery after each activity in the second experiment.In the case of active recovery, the subject ran on a treadmill with an intensity of 45% VO2Max. Before each climb, two additional minutes were considered for blood sampling. The blood samples were taken from auricle vessels for measuring lactate level. Forearm venous blood samples were taken in each period for measuring LDH and CPK levels. Blood samples were taken before the first climb and immediately after each recovery period. The results showed a significant difference between active and passive recovery in terms of lactate and LDH (P <0.005) and CPK levels (P <0.039). Regarding this investigation, after each period of active recovery, the rock-climbers began the next climb with lower levels of lactate, LDH and CPK compared with passive recovery.
Keywords
Recovery (active and passive); Lactate; CPK; LDH; Rock-climbing
Download this article as:| Copy the following to cite this article: Hematfar A, Shekarchian M. The Effect of Short-Term and Interval Periods of Active and Passive Recovery on Blood Lactate, Lactate Dehydrogenase (LDH) and Creatine Phosphokinase (CPK) Levels in Male Rock-Climbers in Borujerd. Biomed Pharmacol J 2013;6(2) |
| Copy the following to cite this URL: Hematfar A, Shekarchian M. The Effect of Short-Term and Interval Periods of Active and Passive Recovery on Blood Lactate, Lactate Dehydrogenase (LDH) and Creatine Phosphokinase (CPK) Levels in Male Rock-Climbers in Borujerd. Biomed Pharmacol J 2013;6(2). Available from: http://biomedpharmajournal.org/?p=2662 |
Introduction
Athletes are always attempting to show their best performance at tournaments. However, several factors may prevent their optimal performance. One of the most effective factors which reduces athletic performance and prevents the activity continuity is fatigue. Fatigue is the most important factor in the inability of a person to perform better. Especially in short periods of high intensity exercises, fatigue usually limits the athletic performance and delays the desired result [1]. One reason for local fatigues is accumulation of lactic acid in active muscles and increase of hydrogen ion concentration in the blood circulation [2]. The amount and type of muscle fatigue depends on the type, duration and intensity of active muscle fibers and environmental factors as well as the intensity of these factors [3]. Increased lactate level in anaerobic exercise is due to reduction of blood flow, because of isometric contraction of active muscles following intense exercises [4]. Intracellular acidosis caused by increased lactic acid is an important factor in development of skeletal muscle fatigue.
Many studies showed that the pH reduction has a little effect on the intensity of muscle contraction [4]. Lactate is the major metabolite in ATP recovery period; although the substance itself is effective in restoring energy resources [5]. Basically, when performing the athletic exercises, muscle cells are stimulated and then stressed. However, the main adjustment in the cell is developed during recovery. This process may be justified as follows: When a cell is involved with muscle tensions, it consumes metabolic energy to sustain tension; this energy is used for setting consistency during recovery period [6]. During recovery, some methods should be used in quickly removal of formed lactate [7]. Lactate removal after exercise is performed as both active and passive recovery; off course, active recovery is much more effective in lactate removal [8].
Among sports, rock-climbing has special features; climb intensity is strongly influenced by rock-climbers exercises and their ability to overcome fatigue in exercises [9, 10]. To maintain the athletic performance at desired level, some physiological factors in athlete’s body must remain in the normal range [10]. The so-called fatigue in rock-climbing is often localized and limited to the muscles in the fingers, elbow flexion and arm [11, 12]. In the case of rock-climbers where the fatigue limits their performance, recovery within climb paths is of vital importance [13]. The strategy of recovery after exercise, starting the next exercise and its effect on skeletal muscles, nervous, immune and metabolic systems in rock-climbers have been discussed [14]because some studies emphasized on force and energy reduction following fatigue immediately after exercise [11, 4].
However, some believes that rest periods between exercise bouts vary from 30 seconds to 3 minutes [15]. Once the recovery is completed, the power returns to its amount before the practice and exercise are followed with a better performance [11] ; rest periods between exercises may be short or long, of course, interval shorter rest times result in higher rate of athletic performance [17, 16]. Rock-climbers forearm and finger strength and endurance decreases by increased lactate levels, following recovery and faster disposal of lactate, the athlete returns to the situation prior the athletic activity, more rapidly [18]. When the goal of exercise is strengthening, short rest periods of 2-5 min are recommended to prepare an individual to maintain and continue exercise [19, 20, and 21].
When interval rests are replicated between periods, the ability increases as well [19]. Evans et al. studied the effect of active and passive recovery on lactate excretion. They found a significant increase in lactate disposal by active recovery [22]. Recovery increases blood flow and the mean heart rate [13]. Watts et al. [10] proved that lactate level increases in both active and passive recovery in rock-climbers. In the case of passive recovery, it took 30 min to reach the initial level while in active recovery the lactate level decreases after 20 min.
Draper et al. [17] studied the effect of short periods of active and passive recovery on lactate levels in rock-climbers. Their results showed that active recovery is very more effective in reducing lactate level. Nicros [23] studied the effect of four types of recovery on rock-climbers and concluded that active recovery along with massage result in maximum lactate excretion. Thereafter, active recovery is more effective than passive recovery. Few studies examined rock-climbing and its physiological effects [9, 10, and 20]. Available data suggest long recovery periods or only refer lactate. While few studies have been carried out on LDH, CPK that need several blood sampling from a forearm vein along with a sampling of the auricle.
On the other hand, incomplete or ambiguous information about the intensity of active recovery -a very important factor to influence the above enzymes and lactate- reveals the need for further research in this area. Therefore, the primary objective of the study is to investigate the effect of 4 periods of 3 min active recovery with a rate of 45% VO2 Max on lactate, lactate dehydrogenase and creatine phosphokinase levels in male rock climbers. Accordingly, research hypotheses are constructed based on 3 min recovery. Unlike previous studies, the activity intensity is quietly controlled in the present study. It can be said that the unique feature of the present study is controlling the intensity of climb as well as controlling activities during recovery. The most important point is that due to the use of hands during the climb and the lack of the impact of pain caused by Lancet on the performance of rock-climbers during the climb, blood samples were taken from the auricle vessels for lactate measurement. Furthermore, several blood samplings from a forearm vein are rarely seen in previous studies.
Another point is that running was used for recovery; due to more volume of the leg muscles than hands (which have a major role in the climb), this recovery method is more effective than other methods for rock-climbers. Researchers agree on the production of lactate and blood enzymes after an intense anaerobic activity. But few studies have been done on the effect of time and intensity of recovery on the reduction rate of these factors, especially in rock-climbers. Thus, the present study aims to examine Iranian rock-climbers by controlling the intensity of recovery activities. This study has investigated the changes in blood lactate, lactate dehydrogenase and creatine phosphokinase levels in rock-climbers.
Research Methodology
This is a quasi-experimental study. The subjects were 10 male rock-climbers in Borujerd (age: 24±2.92 years, weight: 60±6.19 kg, height: 173±5.73 cm and BMI: 19±2.98). The subjects had at least 2 years’ experience of climbing indoor walls and participated in regular exercise programs. They voluntarily participated in this study. Before conducting the study, the subjects signed a medical questionnaire and a consent form for participating in the study. In a briefing meeting, the details of tests were introduced. All subjects were tested using cross-over method in both active and passive recovery plans.
Methods
One week before starting the study protocol, VO2Max was calculated using Bruce test to evaluate the amount and intensity of active recovery. The protocol consisted of two test sessions with an interval of 5 days. In the first experiment, the passive recovery was performed while in second experiment, active recovery was done. In the first experiment, participants warmed up for 10 minutes, and then blood samples were taken from the subjects. In each period, blood samples were taken from the forearm vein using IV for measuring CPK and LDH enzymes. Blood samples were taken from auricle vessels for lactate measurement using a Lactometer device. In the first trial, after warm up and blood sampling, four 2-min climb were performed. A 3-min recovery was carried out within the interval of 2 climbs (in the seats). Blood sampling was performed before the first climb, after each recovery period. Blood sampling were similarly performed in the second experiment, but in this case, active recovery (running on a treadmill with an intensity of 45% VO2Max) was done. In both active and passive recovery, two additional minutes were considered for blood sampling in addition to the time for recovery.
Measurements
Blood lactate level
A Lactometer device (Boehringer Mannheim, Germany) was used to measure blood lactate levels. Blood samples were taken from auricle vessels using an automatic lancet to minimize pain and its impact on assessment by sampling from the fingertip.
Lactate dehydrogenase (LDH) and creatine phosphokinase (CPK)
LDH and CPK enzymes were measured using a special kit E, Vitalab Selectra 2 (Auto Analyzer, the Netherlands).
Treadmill
A J-STAR equipment (Taiwan) was used to measure the speed of running in active recovery.
Climb Wall
An indoor wall with a height of 6 m and an average slope of 28º was used for climbing. The points indicate the climb path and the start and end of the route.
Statistical Methods
The descriptive statistics of mean and standard deviation as well as figures and tables were used to describe results. Inferential statistics of analysis of variance with repeated measurements (MANOVA) was used for data analysis. Independent t-test was used to compare the mean difference (P<0.005). All statistical analyses were carried out using SPSS 15.
Results
Smirnov test was used to examine the normality of data distribution. The data distribution was normal. Tables 1-3 show the descriptive results of 4 recovery periods of lactate, LDH and CPK, respectively.
Table 1: Mean and standard deviation of 4 active and passive recovery periods on lactate
| Lactate (mmol/l) | After 1st recovery | After 2nd recovery | After 3rd recovery | After 4th recovery |
| Passive recovery | 40/1 ± 74/6 * | 84/2 ± 03/11 | 07/2 ± 81/12 | 34/2 ± 01/14 |
| 6.74±1.40 | 11.03±2.84 | 12.81±2.07 | 14.01±2.34 | |
| Active recovery | 71/1 ± 6/5 | 60/1 ± 40/8 | 12/2 ± 37/9 | 88/1 ± 17/11 |
| 5.6±1.71 | 8.40±1.60 | 9.37±2.12 | 11.17±1.88 | |
| Difference | 14/1 | 63/2 | 44/3 | 84/2 |
| 1.14 | 2.63 | 3.44 | 2.84 |
Table 2: Mean and standard deviation of 4 active and passive recovery periods on CPK (U/L)
| CPK U/L | After 1st recovery | After 2nd recovery | After 3rd recovery | After 4th recovery |
| Passive recovery | 53/66 ± 90/223 | 29/71 ± 40/237 | 94/72 ± 00/246 | 27/74 ± 40/250 |
| 223.90±66.53 | 237.40±71.29 | 246.00±72.94 | 250.40±74.27 | |
| Active recovery | 26/49 ± 00/172 | 39/53 ± 50/188 | 25/55 ± 30/200 | 78/54 ± 80/213 |
| 172.00±49.26 | 188.50±53.39 | 200.30±55.25 | 213.80±54.74 | |
| Difference | Sep-51 | 80/48 | 70/45 | 60/36 |
| 51.9 | 48.8 | 45.7 | 36.6 |
Table 3: Mean and standard deviation of 4 active and passive recovery periods on CPK (U/L)
| LDH IU/L | After 1st recovery | After 2nd recovery | After 3rd recovery | After 4th recovery |
| Passive recovery | 75/68 ± 70/322 | 08/92 ± 00/343 | 70/83 ± 00/298 | 15/76 ± 88/268 |
| 322.70±68.75 | 343.00±92.08 | 298.00±83.70 | 268.88 | |
| Active recovery | 73/55 ± 60/279 | 18/72 ± 70/296 | 22/71 ± 70/256 | 55/66 ± 40/240 |
| 279.60±55.73 | 296.70±72.18 | 256.70±71.22 | 240.40±66.55 | |
| Difference | Oct-43 | 30/46 | 30/41 | 48/28 |
| 43.1 | 46.3 | 41.3 | 28.48 |
The results show that the lactate, CPK and LDH levels in active recovery are lower compared to their levels in passive recovery. Figures 1-3 show the variations of lactate, CPK and LDH levels in both active and passive recovery, respectively.
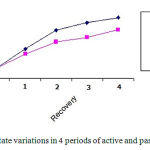 |
Figure 1: Lactate variations in 4 periods of active and passive recovery
|
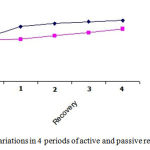 |
Figure 2: CPK variations in 4 periods of active and passive recovery
|
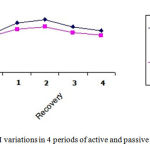 |
Figure 3: LDH variations in 4 periods of active and passive recovery
|
Table 4 represents the analytical results of mean concentrations of lactate, CPK and LDH in active and passive periods of recovery using independent t-test.
Table 4: The t-test analytical results of lactate, CPK and LDH levels in 4 periods of active and passive recovery
| Variables | t | Mean and standard deviation | Significance level | |
| passive | Lactate (mmol/l) | 8-Nov | 82/1 ± 14/11 | 005/0* |
| 8.11 | 11.14±1.82 | 0.005 | ||
| active | 57/1 ± 65/8 | |||
| 8.65±1.57 | ||||
| passive | LDH(UI/L) | 75/5- | 25/76 ± 12/308 | 005/0 |
| -5.75 | 308.12±76.25 | 0.005 | ||
| active | 89/63 ± 35/268 | |||
| 268.35±63.89 | ||||
| passive | CPK (U/L) | 40/2- | 16/71 ± 42/239 | 039/0 |
| -2.4 | 239.42±71.16 | 0.039 | ||
| active | 11/52 ± 65/193 | |||
| 193.65±52.11 | ||||
As it can be seen, there is a significant difference between the two types of recovery. The lactate and LDH and CPK levels are far less in active recovery compared with passive recovery.
Discussion and Conclusion
Increased lactic acid following intense activities and impairment in optimal energy production and muscle contractions [24] have prompted researchers to find more rapid ways to excrete it from the blood and muscles. The objective of the present study is to investigate two types of recovery on blood lactate, LDH and CPK levels. One of the factors affecting the rapid recovery of athletes is the type of activity during recovery. The results show that there is a significant difference between the blood lactate variations in active and passive recovery.
Furthermore, CPK and LDH levels in active recovery were significantly lower than the passive recovery. Cook et al. [25] studied the effect of alternating 3-min rest against 1-min rest on 3 replications of leg press. Their results showed that 2 min of rest had a significant effect on replications. Kashef [26] studied the effects of active and passive recovery on enzymes and blood gases of male athletes. The results showed that active recovery is more effective in rapid elimination of fatigue and lactate reduction.
Nemati et al. [27] examined the effect of three selected cooling down plans on blood lactate excretion following an intense exercise. They concluded that the enough time to cool down should be more than 5 min and cooling down as slow running is more effective in rapid excretion of lactate. Ramazani [6] compared the effect of age on blood lactate excretion in the two types of active and passive recovery. The results showed that blood lactate reduction in active recovery is significant in all age groups compared to passive recovery. Ramazani, et al. [28] studied the effect of active and passive recovery on the levels of blood lactate and heart rate in swimmers. They found a significant difference between levels of blood lactate in the active and passive recovery.
Gaeini [29] studied the effect of three different intermittent periods of recovery on bench press. The results showed that recovery period and rest time between periods have a significant effect on power and force in specific groups of muscles. Von et al. [12] investigated the effect of active recovery between rapid periods in peak performance of swimmers. They concluded that passive recovery leads to better performance of swimmers in an 825 m test. Rahimi [29] studied the effect of rest intervals between exercises on the squat and leg press in 1, 2 and 5 minutes of the rest. It was found that a 5-min rest is more effective than other rest times. These findings are consistent with the results of Kashef [26]. Kashef also indicated the significant effect of active recovery on CPK and LDH levels in male athletes.
Moreover, the effect of active recovery on lactate, CPK and LDH levels in this study and their reductions compared to passive recovery are consistent with the results of Evantes et al. (1983), Ramazani, et al. [6], Ramazani [28], Gaeini [29] and Nemati et al. But Ramezani [6, 27] examined swimmers of various age groups and Gaeini [29] studied bench press. The results for effect of active recovery on above factors in rock-climbers are consistent with the results of Watts et al. [25] and Nicros [23]. They found that active recovery is more effective in rapid excretion of lactate.
Draper and colleagues [17] also demonstrated that besides more influence of active recovery on lactate excretion, alternating short-term periods are highly effective. The results of the present study are consistent with the findings of Draper et al. [17], Willardson et al. [19], Cook et al. [25] and Rahimi [29]. Rahimi found that a 5-min alternating rest period the best time for leg press while Cook et al. [25] reported a 2-min rest period for 3 leg press replications. All of them used short and intermittent recovery between exercises. However, Von et al. [12] showed that passive recovery is more effective in improving the performance of swimmers. This is not consistent with the results of the present study. This may be due to differences in various sports or different intensity of active recovery (60% VO2 Max).
The results of Castro et al. [30] showed that long-term recovery is more effective in minimizing the amount of lactate. Most researchers do not agree on this result. This result is also inconsistent with the results of present study. This discrepancy is possibly due to the time of Castro’s study. At that time (1975), few studies had been done on short-term recovery. This can also be attributed to the implementation method of active recovery. Anyway, low levels of blood lactate are indicative of increased lactate disposal during recovery. The results of this study show a direct relationship between climb replications and increased lactate levels, because anaerobic glycolysis has a major role in energy production. During recovery period, due to the exercise stoppage, the amount of required energy significantly reduces [28]. For faster recovery, it is better to use active rest including light and long running. The best rate is between 30-45% of maximal aerobic capacity. These values vary for trained and untrained people [24].
Given that rock-climbers do not have a high aerobic capacity, this aerobic capacity was selected. In most sports, interval training constitutes the main part of the training sessions (e.g., football or basketball). In rock-climbing, different interval climb results in producing excessive amounts of lactic acid in muscles and blood. So practical and scientific methods are needed to recover the body status and start the next climb. The use of a method which results in required readiness in minimum time is of utmost importance. In the case rock-climbers, a method that results in sooner lactate excretion and partial elimination of fatigue in very important. Coaches can prevent exerting excessive pressure to rock-climbers using this strategy. On the other hand, given the short time period for recovery between training and matches, short time intervals are necessary. In rock-climbing, muscles of upper extremities are the major lactate producers. While in this study, the recovery is primarily performed by lower extremities. The intensity of recovery was consistent with the aerobic capacity of subjects. The subjects ran along with hand motions which aid rapid excretion of lactate. More blood flow in the active muscles results in increased excretion of lactic acid and its movement towards the liver, heart and passive muscles [17].
Since the lactate producer muscles (upper extremities) include a smaller volume of muscle responsible for its excretion (lower extremities), running in active recovery results in further increase in heart rate and increased blood flow and thereby lactate is rapidly excreted. This is a suitable method to resolve of fatigue in rock-climbers relatively. One striking point in this study is repeated blood samplings (10 times) which required collaboration of rock-climbers. Moreover, due to the impact of pain caused by Lactometer lancet on the intensity and frequency of climbs, samples were taken from the auricle vessels. Therefore, considering all findings it can be concluded that to reach relax condition after intense activities, active recovery has significant positive effects, compared with passive recovery. This result can be employed in all sports in which athletes is placed at race or practice condition more than once a day. Rock-climbers can also raise their efficiency using this technique to prevent early fatigue during the successive climbs. Further studies on different recovery times and intensities are needed. Research on rock-climbing on outdoor walls may provide different results.
References
- Hetzler, R.K., knowlton, R.G., Brown, D.D. etal. (1989). The effect of voluntary ventilation on acid- base responses to a Moo Duk Tkow form. Research Quality for Exercise and sports. 60: 77-80.
- Fitts,R.H.(1993) Mechanisms of muscular fatigue In: Resource manual for exercise testing and prescription.American College of Sports Medicine. Lea & Febiger, Philadelphia. exercise.
- Sahlin, K. (1986) Muscle fatigue and lactic acid accumulation. Acta physiologic Scandinavia 1128, 83-91.
- Powers, S.K. and Howley, E.T. (2004). Exercise physiology: Theory and application to fitness and performance. Mc Graw- Hill Boston.
- Robergs, R.A ., Farzaneh, G. and Dary l,P (2004). Biochemistry of exercise-induced metabolic acidosis.American Journal of Physiology-Regulatory Integrative and Comparative Physiology 287,R 502-R516
- Ramazani, A., 2002, The effect of age on the production and disposal of blood lactate in different recovery types after one hundred meters swimming, Olympic 21, published by National Olympic Committee of the Islamic Republic of Iran
- Maughan,R ,Gleeson,M .& Greenhaff, P.L (1977). Biochemistry of Exercise and Training., New York : Oxford University Press.
- Baldari,C.,Videria, M., Madeira, F., Sergio, J. and Guidetti, L. (2005) Bloodlactat removal during recovery at various intensities below the individual anaerobic thereshold in triathletes.Journal of Sports Medicine and Physical Fitness 45,460-466.
- Gaeini, A., (2004), The effect of three various recovery (intermittent rest) on the trained students bench press, Olympic consecutive19, published by the National Olympic Committee of the Islamic Republic of Iran.
- Phillip B. Watts (2004). Physiology of difficult rock climbing Eur Journal Appl physiol 91: 361-372.
- Dotan R.,Falk, B. Raz A. (2000). Intensity effect of recovery from glycolytic exercise on decreasing blood lactate concentration in prepubertal children. Med. sci sports exerc, volume 32, issue. 3.
- Von/ By Felix K.G. Munder. (2005). Influence of differents rest intervals during active or passive recovery on repeated sprint swimming performance. Schwimm Verein Limmate Zurich.
- Luke Roberts (2005). Effectiveness of “Dangling Arm” and “G- Tox” Recovery Techniques. Training for climbing.
- Kir Kandall, D.T. (1990) Mechanism of peripheral fatigue. Medicine and science in sports and Exercise. 22/444- 449.
- Parcell ,A.C.,Sawyer,R.D., Tricoli, V.A and Chinevere, T.D (2002). Minimum rest period for strength recovery during a common isokinetic testing protocol.Medicine and Science in Sports and Exercises 34,1018-1022.
- Zuhal Gultekin, Ayse kin – Isler, Ozgur Surenkok (2006). Hemodynamic and Lactic acid responses to proprioceptive neuromuscular facilitation exercise. Journal of sports science & Medicine vol. 5 issue 3, 375-380.
- Nick Draper, Ellis L. Bird, Ian Colemon and Chris Hodgson (2006). Effects of active recovery on lactate concentration, Heart rate and RPE climbing. Journal of sports science and Medicine. 5, 97-105.
- Nick Nilsson. (2006). The insider secrets of interval training learn How Now!.
- Willardson, J.M. and Burkett, L.N. (2005). A comparison of 3 different rest intervals on the exercise volume completed during a workout. The journal of strength and conditioning research 19, 23-26.
- Watts PB. Daggett M. Gallapher P. Wilkins B. (2002). Metabolic response during sport rock climbing and the effects of active versus passive recovery. Training for climbing (International Journal of sports Medicine). 21 (3) : 185-90.
- Ekblom, Bjorn; Reilly, Thomas (2005). The use of recovery methods post- exercise. Journal of sports science.
- Bul Evans and KJ Cureton (1983). Effects of physiological conditioning on blood lactate disappearance after supramaximal exercise. British Journal of sports Medicine, vol. 17, issue 1, 40-45.
- Nicros, Training center, climb, Research : The benefits of Active recovery (2007).
- Mathews, D.K., and Fox, E.L (1976).The Physiological Basis of Physical Education and Athletics. W.B. Saunders company Philadelphia-London. Toronto.
- Cooke, S.P., Patersen, S.R., & Quinney, H.A. (1997). The influence of maximal aerobic power on recovery of skeletal muscle following aerobic exercise. European Journal of physiology, 75, 512-519.
- Kashef, M., (1996), Effects of two types of active and passive recovery on enzymes and blood gases in men athletes, Ph.D. Thesis, Tehran University.
- Nemati, J., The effect of three selected cooling program on the excretion of blood lactate and heart rate following an exercise in athletes, International Conference of Physical Education and Sport Sciences, Tehran.
- Ramazani, A., (2003), Effects of active and passive recovery on blood lactate levels and heart rate after an intense anaerobic exercise in elite swimmers, Olympic 23, published by National Olympic Committee of the Islamic Republic of Iran.
- Rahimi Rahman, (2005). Effect of different rest intervals on the exercise volume completed during SQUAT BOUTS. Journal of sports science and Medicine 4, 361-366.
- Belcastro, A.N. and Bonen, A. (1975) Lactic acid removal rates during controlled and uncontrolled recovery exercise. Journal of Applied Physiology 39, 932-936.

