
Manuscript accepted on :April 19, 2011
Published online on: 27-11-2015
Plagiarism Check: Yes
Ranjana Tiwary1*, J. N. Tripathi¹ and K. N. Dwivedi²
¹Department of Chemistry, Kuteer P G. College Jaunpur (India). ²Department of Dravyaguna, I.M.S. B.H.U. (India).
Abstract
Diabetes now a days is a global problem. Diabetes mellitus is one of the most prevalant diseases of adults. It will affect a person regardless of weight, age, or race, ,especially if diabetes runs in the family. Medicinal plants used to treat hypoglycemic and hyperglycemic conditions are of considerable interest to ethno-botanical community as they are recognized to contain valuable medicinal properties in different parts of the plant. The active principles of many plant species with desired properties are isolated to cure ailments such as diabetes type-1 and type-2, respectively
Keywords
Wound healing; Diabetic foot ulcer; medicinal plant therapy
Download this article as:| Copy the following to cite this article: Tiwary R, Tripathi J. N, Dwivedi K. N. Effect of Medicinal Plant on Wound Healing in Diabetics. Biomed Pharmacol J 2011;4(1) |
| Copy the following to cite this URL: Tiwary R, Tripathi J. N, Dwivedi K. N. Effect of Medicinal Plant on Wound Healing in Diabetics. Biomed Pharmacol J 2011;4(1). Available from: http://biomedpharmajournal.org/?p=1879 |
Introduction
Diabetes mellitus is associated with micro vascular changes, deranged immunity neurologic and macro vascular complications. These factors play a vital role to delay the wound healing process in diabetics. Sushruta-one of the ancient scholar of Ayurveda (the Indian system of Medicine) a great surgeon and the author of Sushruta Samhita (1000 B.C.) has very scientifically pointed out that the vessels of a diabetic become weak to perform normal functions which ultimately lead to cause non-healing/delayed healing nature of wounds in a diabetic.
In the context of present era we can say that micro vascular changes and deranged immunity are two major factors related to delayed wound healing in diabetics even after a good control over blood sugar levels. Infection is another important factor to make the situation worse and all these factors often lead to development of gangrene. Finally this situation ends either in the form of amputation of the part or death of the patient due to toxemia, gas gangrene/pulmonary embolism. Today the problem of diabetic wound is a challenge to clinicians because amputation is not a desirable answer and the healing is not in its normal process in diabetics. Amputation causes irreparable physical mental and social damage and death causes in compensable loss of life. It is the need of era to provide a safe treatment to diabetic wounds for proper healing to save the body part and to restore normal functions.
The paucity of literature and the beneficial effect of this medicinal plant therapy prompted us to conduct this study on this dreaded complication of diabetes. Available data has shown that present therapy by medicinal plants has great potential for accelerated healing, reduction in number of amputation, reduction in duration of hospital stay and control of infection of the wounds in the diabetics.
Material and Methods
This study was conducted in age-matched groups during a period of 2 years. A total of 100 patients of non-healing diabetic foot ulcer having 6-12 months duration were selected. The study was done among 100 patients consisting of 70 males and 30 females. The patients were divided into two groups A and B consisting of 50 cases in each group. Both the groups were age-matched and divided in a randomised fashion. All the patients were thoroughly examined as per our research protocol which included detailed clinical examination, roentgenogram of the affected part, blood glucose profile, lipid profile, blood urea, serum creatinine, wound swab culture, antibiotic sensitivity testing of the micro-organism, ultrasound Doppler recording of arterial circulation of affected part and Ankle-Brachial blood pressure ratio (AB Index).
Methods
The patients of group “A” received regular treatment consisting of suitable systemic antibiotics according to the antibiotic sensitivity pattern along with metronidazole, local antiseptics, and peripheral vascular dialator (Pentoxifylline). The patients of group “B” were treated with water-soluble solid extract of manjishtha (Rubia cordifolia) 500 mg orally thrice daily. The patients were also required to keep the affected part dipped in luke warm decoction of roots of the plant for 30 minutes daily. Then their wounds were dressed without using any conventional local antiseptic.
The patients of both the groups received regular surgical treatment consisting of incision, drainage of abscesses and wound debridement (as and when required).
Diabetic control in both the groups was achieved by suitable oral hypoglycemic agents or insulin, all the patients were kept on diet yielding 1500-2000 calories per day.
On the basis of description available in ancient Ayurvedic texts. We select Majishtha (Rubia Cordifolia Linn.) our test drug. For the purpose of oral administration water soluble solid extracts of the plant was prepared by classical Ayurveic method by using the roots. The roots of the crude drug were taken in a sterilized container and water amounting four times than that of crude drug was addedd to it. Then it was heated until 3/4th of the water was evaporised. Then it was filtered. This filtrate is called as Kvatha (Decoction). Thus obtained decoction was further gently heated until in became semisolid. Then it was cooled at room temperature. We obtained water soluble solid extracts of the plant by this method of oral use.
For external use (dipping purpose) the Kvatha (decoction) was prepared as described above. The standardising parameters of decoction of the plant was as follows:
Decoction of Rubia cordifolia
pH = 6.2
Specific gravity = 1.013 to 1.015
Solid contents = 27.20 mg%
Temperature = 37-40°C
Parameters of Assessment
The patients of both the groups were assessed periodically at the interval of one month. The subjective parameters included improvement in general condition and sense of well being, body temperature and body weight.
The objective parameters of assessment included naked eye examination (measurement of ulcer margins by centimetre tape by Smelo’s device, presence of healthy granulation tissue, absence of purulent discharge), tissue biopsies for histological changes, roetgenogram of affected part, improvement in arterial circulation (by ultrasound Dopper recording and AB index). Immunological changes (in the levels of lgG, 1gA and 1gM) and estimation of total proteins.
Criteria for grading of results
Only objective parameters were taken for grading the results. These parameters included –
(i) Improvement in arterial circulation (by ultrasound Dopper recording and AB index).
(ii) Favourable histological changes.
(iii) Naked eye examination of the wound (measurement) of ulcer margins by centimetre tape by Smelo’s device, presence of healthy granulation tissue and absence of purulent discharge).
(iv) Improvement in immunological status.
We categorised the results as
(a) Mild recovery-If any two of the above parameters were found improved.
(b) Moderate recovery – if any three of the above parameters were found improved.
(c) Good recovery- if all the four parameters were found improved.
Results
There were a total of 100 patients equally divided in both the groups- A & B. The age and sex group distribution has been shown in Table 1 and 2. Sixty patients belonged to rural area and fourty to urban area (Table 3). 40% patients had diabetes for 5 to 10 years and the same percentages of patients were recorded having diabetes for more than 10 years (table 4).
Table: 1 Pattern of Age-group in present study.
| Age Group (Yrs) | No. of Cases | Percentage |
| 31-40 | 10 | 10% |
| 41-50 | 20 | 20% |
| 51-60 | 30 | 30% |
| 61-70 | 30 | 30% |
| >70 | 10 | 10% |
Table 2: Pattern of Sex in present study
| Sex | No. of Cases | Percentage |
| Male | 70 | 70% |
| Female | 30 | 30% |
Table 3: Social Status of the patients
| Sex | No. of Cases | Percentage |
| Rural | 60 | 60% |
| Urban | 40 | 40% |
Table 4 : Duration of diabetes in patients studied.
| Duration of | No. of | Percentage |
| Diabetes (yrs.) | Cases | |
| 0-5 | 30 | 30% |
| 10-Jun | 40 | 40% |
| > 10 | 40 | 40% |
Table 5: Quantitative estimation of immunoglobulin and total protein in patients of group “A” and its statistical analysis is shown in Table 5 and 6.
| Immunoglobulin/ | Lab. Control | Group B | |
| Total Proten | Values for age- | (B1) | (B2) |
| matched non- | Before treatment | After treatment | |
| Diabetics (mg%) | (mg%)Mean/ ±SD | (mg%) Mean±SD | |
| Mean/± SD | |||
| lgG | 1145±208.20 | 1680±111.64 | 1768±190.26 |
| lgA | 295.50±40.90 | 282±46.51 | 320±44.42 |
| lgM | 148.70±40.90 | 94±19.916 | 122±49.923 |
| Total Protein | 7.54±0.66 | 6.1±0.31 | 7.02±2.811 |
Table 6: Statistical analysis of group “A” findings
| Groups | IgG | IgA | lgM | Total Protein |
| Compared | T-Value | T Value | T Value | T Value |
| P Value | P Value | P Value | P Value | |
| Control Vs. A | 7.1056 | 0.5842 | 3.137 | 3.817 |
| <0.001 | >0.05 | >0.01 | >0.01 | |
| Control Vs. A2 | 7.32 | 1.2076 | 0.5386 | 0.4185 |
| <0.001 | >0.05 | >0.05 | >0.05 | |
| A1 Vs. A2 | 0.16 | 1.804 | 1.374 | 0.675 |
| <0.05 | >0.05 | >0.05 | >0.05 |
Table 7: Quantitative estimation of immunoglobulin and total protein in patients of group “A”
| Immunoglobulin/ | Lab. Control | Group B | |
| Total Proten | Values for age- | (B1) | (B2) |
| matched non- | Before treatment | After treatment | |
| Diabetics (mg%) | (mg%)Mean/ ±SD | (mg%) Mean±SD | |
| Mean/± SD | |||
| lgG | 1145±208.20 | 1720±143.44 | 1828±201.26 |
| lgA | 295.50±40.90 | 291±47.53 | 349±47.72 |
| lgM | 148.70±40.90 | 104±20.659 | 152±82.603 |
| Total Protein | 7.54±0.66 | 6.3±0.39 | 8.07±2.811 |
Table 8: Statistical analysis of group “B” findings.
| Groups | IgG | IgA | lgM | Total Protein |
| Compared | T-Value | T Value | T Value | T Value |
| P Value | P Value | P Value | P Value | |
| Control Vs. A | 7.1856 | 0.5855 | 1.5386 | 3.877 |
| <0.001 | >0.05 | >0.01 | >0.01 | |
| Control Vs. A2 | 7.44 | 1.4988 | 0.5386 | 0.8785 |
| <0.001 | >0.05 | >0.05 | >0.05 | |
| A1 Vs. A2 | 0.163 | 1.985 | 1.734 | 0.979 |
| <0.05 | >0.05 | >0.01 | >0.01 |
Above observation prove that only lgG level has been elevated upto statistically significant extent in the patients of group ‘A” being treated with convential antibiotic, antiseptics etc. lgA. lgM and total proteins did not show any significant change in their status in these patients.
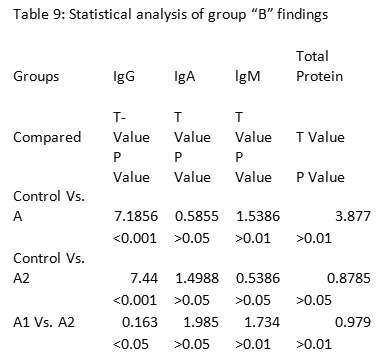 |
Table 6 : Statistical data showing change in AB index (for arterial circulation) in patients studie.
|
Apart from this the patients of group “A” Showed mild to moderate recovery and 30% cases underwent either total or partial amputations.
Table 7 and 8 show the quantitative estimation of immunoglobulins and total protein and their statistical analysis in the patients of group “B” treated by medicinal plant therapy-
In patients of group “B” being treated with medicinal plants it is evident from table 7 and 8 that statistically significant changes have been noticed in lgG. lgM and total protein levels when compared before and after treatment but when we compared the findings of after treatment with that of control values, it was observed that only lgG, lgA and total protein levels showed significant improvement and lgM level did not show any significant change.
After three months therapy statistically significant changes in the ratio of Brachial and Ankle Blood pressure (AB index) was noticed in the patients of both the groups.
Apart from these changes patients of group “B” showed moderate to good recovery and domonstrable histological changes in terms of reduced subepithelial oedema reduced exudates vascular change proliferation and appearance of health granulation tissue. A very good improvement in arterial circulation was also recorded by ultrasound doppler in the arteries and capilliaries supplying to the affected part.
Most significant fact noticed was that only 16% cases underwent partial amputation in the patients of group “B” receiving medicinal plant therapy.
Discussion
The overall outcome was significantly better in the patients of group “B” receiving medicinal plant therapy 84% cases of group “B” showed moderate to good recovery i.e. three or all four paramenters of assessment were found improved in three months. These patients presented appreciable growth of healthy granulation tissue, marked improvement in the arterial circulation of the affected part (as recored by doppler and AB index) as well as improved immunological status. It is to be noticed that only 16% cases of this group underwent partial amputation.
The patients of group “A” who received conventional treatment of antibiotics showed mild to moderate recovery i.e. only two or three, out of tour parameters were found improved in these patients after three months therapy. The patients of this group showed a lesser improvement in the arterial circulation when compared to group “B” Only lgG level was found statistically improved in this group. Overall, more number of patients (30%) required total or partial amputation.
The most striking effect of the medicinal plant therapy was seen in control of purulent discharge and if present, the maggots came out spontaneously only after 4-6 dippings.
The plant Majishtha (Rubia cordifolia) in Ayurvedic texts has been claimed for its wonderful VISHAGHNA (Detoxicating/Antimicrobia) and SROTOSHO DHAKA (Channel Clearing) actions. Most probably it showed it effect by removing the microangiopathic and atherosclerotic changes inside the arteries and capillaries supplying the area of non healing wound and thus facilitated proper blood supply and nutrition to the area. Owing to its VISHAGHNA prabhava (DETOXICATING/ANTIMICROBIAL ACTION) it has proved itself efficient enough to remove the microbes causing infection.
Present study has proved that the medicinal plant is of potential value to treat non healing diabetic wounds. This plant deserves be further explored for its possible beneficial role in other diabetic complications.
References
- Bailey CJ, Day C. Traditional plant medicines as treatment for diabetes. Diabetes Care. 12: 553–564 (1989).
- Keen RW, Deacon AC, Delves HT, Moreton JA, Frost PG. Indian herbal remedies for diabetes as a cause of lead poisoning. Postgrad Med J; 70: 113–114 ( 1994).
- Morgan M, Watkins CJ. Managing hypertension: beliefs and responses to medication among cultural groups. Sociol Health Illn; 10: 561–578 (1988).
- J. P. Burke, et al., Diabetes Care, 26: 7 (2003).
- B. Thylefors, The WHO program for the prevention of blindness. Int. J. of Ophthal., 14: 211 (1990).
- Gulliford MC. Health and health care in the English-speaking Caribbean. J Public Health Med., 16: 263–269 (1994).
- Morgan M. The significance of ethnicity for health promotion: patients’ use of antihypertensive drugs in inner London. Int J Epidemiol., 24: S79–S84 (1995).
- J. K. Grover, et al., J Ethnopharmacol., 81: 81 (2002).

