
Manuscript accepted on :18-09-2025
Published online on: 26-09-2025
Plagiarism Check: Yes
Reviewed by: Dr. Putu Indah
Second Review by: Dr. Ana Golez
Final Approval by: Dr. Prabhishek Singh
Hala Tabie El-Bassyouni1 , Dina Abdallah Nagi1, Eman Refaat Youness2*, Hisham Abdel Aziz Orban2, Hend Mostafa Ahmed2, Kamal Abdel Rahman El- Atrebi 3, Hanaa Reyad Abdallah4and Moushira Zaki4
, Dina Abdallah Nagi1, Eman Refaat Youness2*, Hisham Abdel Aziz Orban2, Hend Mostafa Ahmed2, Kamal Abdel Rahman El- Atrebi 3, Hanaa Reyad Abdallah4and Moushira Zaki4
1Clinical Genetics Department, Human Genetics and Genome Research Institute, National Research Centre, Cairo, Egypt.
2Medical Biochemistry Department, Medical Research Institute, National Research Centre, Cairo, Egypt.
3 General Medicine and Hepatology Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt.
4Biological Anthropology Department, Medical Research and Clinical Studies Institute, National Research Centre, Cairo, Egypt.
Corresponding Author E-mail: hoctober2000@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/3227
Abstract
Inflammatory bowel disease (IBD) is a chronic, relapsing-remitting condition of the gastrointestinal tract with an unclear etiology. It is characterized by alternating periods of active inflammation and clinical remission. Among the biomarkers used to assess disease activity, serum C-reactive protein (CRP) and fecal calprotectin (FCP) have emerged as noninvasive, reliable indicators of intestinal inflammation, offering valuable insights into disease monitoring and management. A total of 150 patients with IBD, and 150 control subjects with no history of intestinal resections were included and were prospectively recruited from the IBD Clinic of the National Institute of Hepatology and Tropical Medicine (NHTMRI) and the Clinical Genetics Department of the National Research Centre. (FCP) and (CRP) markers were measured. Receiver operating characteristic (ROC) curves were used to evaluate the accuracy of FCP and CRP for diagnosing inflammatory activity. The median values of these markers were significantly higher in IBD than in controls. FC was associated with higher sensitivity than CRP for the diagnosis of IBD. ROC curve analysis revealed FCP had higher sensitivity for diagnosing with a higher area under the curve than CRP. We concluded that both (CRP) and (FCP) demonstrated a strong association with colorectal inflammation. These biomarkers can serve as valuable tools for monitoring treatment response, screening asymptomatic individuals, and predicting disease relapse in patients with inflammatory bowel disease (IBD).
Keywords
Crohn’s Disease; CRP; Fecal calprotectin; IBD; Ulcerative Colitis
Download this article as:| Copy the following to cite this article: El-Bassyouni H. A, Nagi D. A, Youness E. R, Orban H. A. A, Ahmed H. M, El-Atrebi K. A, R, Abdallah H. R. Zaki M. Fecal Calprotectin and CRP: Noninvasive Biomarkers in IBD. Biomed Pharmacol J 2025;18(3). |
| Copy the following to cite this URL: El-Bassyouni H. A, Nagi D. A, Youness E. R, Orban H. A. A, Ahmed H. M, El-Atrebi K. A, R, Abdallah H. R. Zaki M. Fecal Calprotectin and CRP: Noninvasive Biomarkers in IBD. Biomed Pharmacol J 2025;18(3). Available from: https://bit.ly/3VEL9gK |
Introduction
Inflammatory bowel diseases (IBDs) are chronic disorders of the gastrointestinal tract with an unclear etiology, characterized by alternating periods of remission and exacerbation.1,2 One manifestation, colitis, often presents with chronic diarrhea as a primary symptom. Notably, colitis may display no visible abnormalities during colonoscopy; however, histological analysis of biopsy samples typically reveals enlarged intraepithelial lymphocytes within the colonic mucosa. Patients commonly experience lower gastrointestinal symptoms, including persistent abdominal pain accompanied by diarrhea or constipation.1 To assess disease activity, both invasive and noninvasive diagnostic methods are utilized. Among these, fecal calprotectin (FCP) testing has gained prominence due to its high sensitivity and noninvasive nature, making it a preferred tool for detecting gastrointestinal inflammation. 3
C-reactive protein (CRP) levels and fecal calprotectin (FCP) testing are currently among the most widely recommended diagnostic tools for assessing gastrointestinal inflammation.4,5 FCP is favored for its high sensitivity and non-invasive nature, making it especially suitable for routine clinical evaluation. We aimed to assess the utility of fecal calprotectin in monitoring inflammatory bowel disease (IBD) activity and to explore its correlation with serum CRP levels.
Materials and Methods
This prospective study was carried out at the National Institute of Hepatology and Tropical Medicine’s (NHTMRI) IBD Clinic and the National Research Center’s Clinical Genetics Department 150 patients affected with IBD, 120 with Ulcerative Colitis (UC), and 30 with Crohn’s Disease (CD), aged 25 to 65 years, and 150 healthy controls. Of all participants, 35 had positive consanguinity, whereas only 12 had similarly affected family members.
Informed consent was obtained from all participants before conducting this observational cross-sectional study. The National Hepatology and Tropical Medicine Research Institute’s (NHTMRI) Research Ethics Committee provided ethical approval, under approval number 11-2022. The study was conducted in accordance with national regulations, institutional guidelines, and the principles outlined in the Declaration of Helsinki.
Expert gastroenterologists confirmed the diagnosis of ulcerative colitis and Crohn’s disease at the specialized clinic of the National Hepatology and Tropical Medicine Research Institute (NHTMRI). Diagnostic confirmation was based on colonoscopic findings, histopathological evaluation of colonic biopsy specimens, relevant laboratory parameters, and clinical presentation. The control group consisted of healthy individuals matched by age and gender, randomly selected from among the patients’ companions.
Each patient was carefully evaluated through detailed clinical examination and complete medical history documentation, encompassing age, consanguinity, familial occurrence of similar conditions, as well as anthropometric measurements such as weight and height.
Assessment of Fecal Calprotectin (FCP)
Dry stool sample was collected and mixed with a phosphate-buffered saline (PBS) in a 1:9 ratio (e.g., 9 mL of buffer for 1g of stool). The mixture is then typically shaken or vortexed to homogenize it, followed by centrifugation to separate the solid components from the liquid supernatant. This supernatant was collected and the ELISA kit (My Biosource Co., Ltd.), catalog number MBS7606803, was used to measure FCP according to the manufacturer’s instructions.
Assessment of C-reactive protein (CRP)
The nephelometric technique (C-Reactive Protein Reagent, IMMAGE Immunochemistry Systems catalog number k981638) was used to assay CRP.
Statistical analysis
The statistical software SPSS version 20 was used for all analyses. The median and interquartile range (IQR) were used to describe the results for nonparametric data. The Mann–Whitney U test was used to compare two independent samples in groups. The best cut-off values for fecal calprotectin (FCP) and C-reactive protein (CRP) in the diagnostic evaluation were found using Receiver Operating Characteristic (ROC) curve analysis.
Results
Table 1: CRP and FC median levels and interquartile range in IBD patients. The FCP and CRP levels in the IBD group were significantly higher than those in the control group.
| Median | IBD | Control | p |
| FCP (mg/kg) | 255(202-407) | 94(79-113) | 0.01 |
| CRP (mg/l) | 41(28.6-55.6) | 3.15(2.8-4.05) | 0.01 |
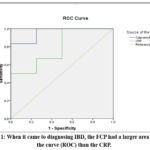 |
Figure 1: When it came to diagnosing IBD, the FCP had a larger area under the curve (ROC) than the CRP. |
Discussion
IBD encompasses ulcerative colitis (UC) and Crohn’s disease (CD), both of which are characterized by persistent gastrointestinal inflammation. 6,7 The pathogenesis includes Genetic susceptibility, environmental triggers, unbalanced microbiota, and immune dysregulation.8 This results in mucosal damage, ulceration, and infiltration of immune cells, especially neutrophils, which play a key role in calprotectin release.9 Calprotectin is a calcium-binding immune cell-derived protein found in neutrophils. It makes up approximately 60% of their cytosolic protein. When neutrophils migrate to the intestinal mucosa during inflammation, they release calprotectin into the gut lumen. It is then excreted in stool, making it a specific marker of intestinal inflammation.10 Calprotectin has inherent antimicrobial and anti-inflammatory properties and plays a pivotal role in immune regulation and intestinal homeostasis.11
Fecal calprotectin (FCP) has recently been recognized as a simple, noninvasive biomarker for assessing disease activity in patients with ulcerative colitis (UC). 12 Recent therapeutic strategies for IBD focus on suppressing pro-inflammatory cytokines and preventing leukocyte migration to inflamed intestinal tissue by targeting sphingosine-1-phosphate receptors and integrins. 13,14 Despite its clinical importance, studies evaluating the usefulness of fecal calprotectin (FCP) in IBD management are limited in this region. In our cohort, FCP demonstrated strong diagnostic performance, with a cut-off value of 200 mg/kg, providing a sensitivity of 95%, a specificity of 85%, and an area under the curve (AUC) of 0.95. (Figure 1).
Calprotectin’s clinical value includes monitoring disease activity and response to treatment, as well as helping to distinguish IBD from functional diseases like irritable bowel syndrome (IBS), predicting illness recurrence, and reducing the need for endoscopies.15
The liver produces CRP in response to systemic inflammation. CRP is triggered by signals comprising IL-6, TNF-α, and IL-1β released during immunological activation in IBD. 16 CRP correlates with disease activity, tracks the effectiveness of treatment, predicts flare-ups, and guides therapeutic decisions. 17,18 However, CRP levels may not always accurately reflect mucosal inflammation, particularly in UC.19
When measured in tandem, calprotectin and CRP provide a more comprehensive view of disease activity, aid in precise diagnosis, help customize treatment regimens, and avoid unnecessary procedures. 20 FCP and CPR levels have been used in several studies to diagnose inflammatory activity in IBD.21-24 The cut-off values were chosen to determine the variety of sensitivity and specificity values.25
Compared to treatments based solely on symptoms, it was shown that treating CD patients based on clinical evaluation and biomarkers (FCP and CRP) produced better results.26 However, the use of biomarkers alone versus in combination was not compared in that study. Furthermore, CD patients were not categorized based on the disease’s clinical activity.27,28 Moreover, the efficacy of these tests was established in three clinical settings. FCP was more sensitive than CRP in both diseases and showed greater sensitivity in ulcerative colitis than in Crohn’s disease. 29,30 The area under the ROC curve analysis showed that FCP and CRP levels were highly accurate in identifying inflammatory activity in CD.31 Studies from different parts of the world revealed wide variability in the FCP cut-off levels used to predict disease activity and distinguish from IBS patients.32,33 The Mayo Score and MES in this investigation indicated a significant relationship between FCP concentration and disease activity. According to research on the best FCP cut-off levels for identifying disease activity and distinguishing this group from IBS patients, endoscopic inflammation in this group was associated with FCP, C-reactive protein, and erythrocyte sedimentation rate. Nevertheless, in patients with endoscopically active illness, FCP was higher more often than erythrocyte sedimentation rate and C-reactive protein. Our results confirm earlier findings that FCP predicts endoscopic inflammation better than other biomarkers.34,35
Conclusion
In conclusion, this study demonstrated that fecal calprotectin (FCP) and C-reactive protein (CRP) are effective non-invasive diagnostic tools for inflammatory bowel disease (IBD), exhibiting high diagnostic accuracy with a sensitivity of 95%, specificity of 85%, and an area under the ROC curve (AUC) of 0.95. However, considerable variability in FCP cut-off values was observed, particularly during the initial diagnosis of ulcerative colitis (UC) and in post-treatment follow-up. These findings underscore the need for standardized validation of available test kits and the establishment of population-specific cut-off thresholds to enhance diagnostic precision and clinical utility.
Acknowledgement
We thank all the participants and the National Research Centre
Funding Sources – The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Author contributions
Hala Tabie El-Bassyouni, Moushira Zaki, and Hanaa Reyad Abdalla: Conceptualization, writing the original draft, and approved final draft.
Dina Abdallah Nagi: Collect the data.
- Eman Refaat Youness, Hisham Abdel Aziz Orban, and Hend Mostafa Ahmed: laboratory procedures, data analysis, and approved final draft.
- Kamal Abdel Rahman El-Atrebi: Clinical investigations
Reference
- Walsham NE., Sherwood RA. Fecal calprotectin in inflammatory bowel disease. Exp. Gastroenterol. 2016; 28;9:21–29.
CrossRef - Wan J, Zhou J, Wang Z, Liu D, Zhang H, Xie S, Wu K. Epidemiology, pathogenesis, diagnosis, and treatment of inflammatory bowel disease: Insights from the past two years. Chin Med J (Engl). 2025 ; 5;138(7):763-776.
CrossRef - Dhaliwal A, Zeino Z, Tomkins C, Cheung M, Nwokolo C, Smith S, Harmsto C, Arasaradnam RP. Utility of faecal calprotectin in inflammatory bowel disease (IBD): what cut-offs should we apply? Frontline Gastroenterol. 2015; 6, 14–19.
CrossRef - Vermeire S, Van Assche G, Rutgeerts P, C-reactive protein as a marker for inflammatory bowel disease. Bowel Dis. 2004; 10, 661–665.
CrossRef - Schoepfer AM, Beglinger C, Straumann A, et al. Fecal calprotectin correlates more closely with the Simple Endoscopic Score for Crohn’s disease (SES-CD) than CRP, blood leukocytes, and the CDAI. Off. Am. Coll. Gastroenterol. ACG. 2010; 105, 162–169.
CrossRef - El-Atrebi KA, Taher E, El Aguizy FH, Ali RM, Hegazy A, El-Sayed MM, Eysa B, El-Atreby AA, Mohammed AA, El-Bassyouni HT. A descriptive study of inflammatory bowel disease at an Egyptian tertiary care center. Rev Gastroenterol Mex (Engl Ed). 2023;88(1):12-18.
CrossRef - Zaki, M., Orban, H.A., Mahmoud, M. et al. Evaluation of adropin, fibroblast growth factor-1 (FGF-1), and Toll-like receptor-1 (TLR1) biomarkers in patients with inflammatory bowel disease: gene expression of TNF-α as a marker of disease severity. Egypt J Med Hum Genet. 2024;25, 63.
CrossRef - Guo X, Li J, Xu J, Zhang L, Huang C, Nie Y, Zhou Y. Gut microbiota and epigenetic inheritance: implications for the development of IBD. Gut Microbes. 2025;17(1):2490207.
CrossRef - Li T, Jing H, Gao X, Zhang T, Yao H, Zhang X, Zhang M. Identification of key genes as diagnostic biomarkers for IBD using bioinformatics and machine learning. J Transl Med. 2025;23(1):738.
CrossRef - Janssen L, van Linschoten RCA, West RL, Gilissen LPL, Romberg-Camps M, Brandts L, Mujagic Z, Römkens TE, Pierik M. Predicting mucosal inflammation in IBD patients using patient-reported symptom scores and a faecal calprotectin home test: protocol for a multicentre prospective validation study. BMJ Open. 2024;14(10):e076290.
CrossRef - Wang W, Cao W, Zhang S, Chen D, Liu L. The Role of Calprotectin in the Diagnosis and Treatment of Inflammatory Bowel Disease. Int J Mol Sci. 2025;26(5):1996.
CrossRef - Clough J, Colwill M, Poullis A, Pollok R, Patel K, Honap S. Biomarkers in inflammatory bowel disease: a practical guide. Adv. Gastroenterol. 2024; 17, doi: 10.1177/17562848241251600.
CrossRef - Liu J, Di B, Xu L. Recent advances in the treatment of IBD: Targets, mechanisms, and related therapies. Cytokine Growth Factor Rev. 2023; 71-72:1-12.
CrossRef - Cai Z, Wang S, Li J. Treatment of inflammatory bowel disease: a comprehensive review. Med. 2021; 8, 765474.
CrossRef - Lichtenstein GR, Loftus EV, Afzali A, Long MD, Barnes EL, Isaacs KL, Ha CY. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2025;120(6):1225-1264.
CrossRef - Toskas A, Manti M, Kamperidis N, Arebi N. Infliximab Precision Dosing in Inflammatory Bowel Disease (IBD) Patients: A Review of Current Literature. Cureus. 2024;16(12): e76424.
CrossRef - Omer N, Ibrahim S, Ramadhan AA. Diagnostic Value of Inflammatory Markers in Inflammatory Bowel Disease: Clinical and Endoscopic Correlations. Cureus. 2025;17(5):e84073.
CrossRef - Takagi Y, Sato T, Nishiguchi T, Nogami A, Igeta M, Yagi S, Ikenouchi M, Kawai M, Kamikozuru K, Yokoyama Y, Tomita T, Fukui H, Fukata M, Kobayashi T, Shinzaki S. Real-World Effectiveness and Safety of Mirikizumab Induction Therapy in Patients with Ulcerative Colitis: A Multicenter Retrospective Observational Study. Aliment Pharmacol Ther. 2025;61(12):1923-1934.
CrossRef - Sezer S, Demirci S, Kara MI, Korkmaz M. The Serum Biomarkers in Ulcerative Colitis. Medeni Med J. 2024;39(4):261-267.
CrossRef - González-Moret R, Cebolla-Martí A, Almodóvar-Fernández I, Navarrete J, García-Esparza Á, Soria JM, Lisón JF. Inflammatory biomarkers and psychological variables to assess quality of life in patients with inflammatory bowel disease: a cross-sectional study. Ann Med. 2024 Dec;56(1):2357738.
CrossRef - Kyle BD, Agbor TA, Sharif S, Chauhan U, Marshall J, Halder SLS, Ip S, Khan WI. Fecal Calprotectin, CRP, and Leucocytes in IBD Patients: Comparison of Biomarkers With Biopsy Results. J Can Assoc Gastroenterol. 2020;4(2):84-90.
CrossRef - Magro F, Domingues B, Estevinho MM, Patita M, Arroja B, Lago P, Rosa I, Tavares de Sousa H, Ministro P, Mocanu I, Vieira A, Castela J, Moleiro J, Roseira J, Cancela E, Sousa P, Portela F, Correia L, Fernandes S, Dias CC, Dias S, Peyrin-Biroulet L, Danese S, Santiago M. Longitudinal profiles of fecal calprotectin and C-reactive protein in relation to outcomes in Crohn’s disease patients on infliximab. J Crohns Colitis. 2025;19(8):jjaf120.
CrossRef - Shahub S, Kumar RM, Lin KC, Banga I, Choi NK, Garcia NM, Muthukumar S, Rubin DT, Prasad S. Continuous Monitoring of CRP, IL-6, and Calprotectin in Inflammatory Bowel Disease Using a Perspiration-Based Wearable Device. Inflamm Bowel Dis. 2025;31(3):647-654.
CrossRef - Hou D, Swaminathan A, Borichevsky GM, Frampton CM, Kettle AJ, Gearry RB. Plasma Calprotectin and Myeloperoxidase as Biomarkers in Inflammatory Bowel Disease. Inflamm Bowel Dis. 2025:izaf110.
CrossRef - Lobatón T, López-García A, Rodríguez-Moranta F, Ruiz A, Rodríguez L, Guardiola J. A new rapid test for fecal calprotectin predicts endoscopic remission and postoperative recurrence in Crohn’s disease. Crohn’s Colitis. 2013; 7, e641–e651.
CrossRef - Colombel J.-F, Panaccione R, Bossuyt P et al. Effect of tight control management on Crohn’s disease (CALM): a multicentre, randomised, controlled phase 3 trial. Lancet. 2017; 390, 2779–2789.
CrossRef - Penna FGC, Rosa RM, Pereira FH et al.Combined evaluation of fecal calprotectin and C-reactive protein as a therapeutic target in the management of patients with Crohn’s disease. Hepatol. 2021; 44, 87–95.
CrossRef - Mosli MH, Zou G, Garg SK et al. C-Reactive Protein, Fecal Calprotectin, and Stool Lactoferrin for Detection of Endoscopic Activity in Symptomatic Inflammatory Bowel Disease Patients: A Systematic Review and Meta-Analysis. Off. Am. Coll. Gastroenterol. 2015; 110(6) doi:10.1038/ajg.2015.120.
CrossRef - Menees SB, Powell C, Kurlander J, Goel A, Chey WD. A Meta-Analysis of the Utility of C-Reactive Protein, Erythrocyte Sedimentation Rate, Fecal Calprotectin, and Fecal Lactoferrin to Exclude Inflammatory Bowel Disease in Adults With IBS. Off. Am. Coll. Gastroenterol. 2015; 110(3):444-54.
CrossRef - Temido MJ, Peixinho M, Cunha R, Silva A, Lopes S, Mendes S, Ferreira AM, Ferreira M, Figueiredo P, Portela F. Plasma calprotectin as a biomarker of inflammatory activity in ulcerative colitis. Med Clin (Barc). 2025;164(4):168-172. English, Spanish.
CrossRef - Pepys MB, Druguet M, Klass HJ, Dash A., Mirjah DD, Petrie, A. Immunological studies in inflammatory bowel disease, in: Ciba Foundation Symposium. 1977; 46(46):283-304 .
CrossRef - Olsen BC, Opheim R, Kristensen VA, Høivik ML, Lund C, Aabrekk TB, Johansen I, Aass Holten KI, Strande V, Glad IF, Bengtson MB, Ricanek P, Detlie TE, Medhus AW, Boyar R, Torp R, Vatn S, Frigstad SO, Valeur J, Bernklev T, Jelsness-Jørgensen LP, Huppertz-Hauss G. Prevalence of Irritable Bowel Syndrome Based on Rome IV Criteria in Patients in Biochemical and Endoscopic Remission From Newly Diagnosed Inflammatory Bowel Disease: One- and Three-Year Results (the IBSEN III Cohort). Inflamm Bowel Dis. 2025:izaf047.
CrossRef - Dajti E, Frazzoni L, Iascone V, Secco M, Vestito A, Fuccio L, Eusebi LH, Fusaroli P, Rizzello F, Calabrese C, Gionchetti P, Bazzoli F, Zagari RM. Systematic review with meta-analysis: Diagnostic performance of faecal calprotectin in distinguishing inflammatory bowel disease from irritable bowel syndrome in adults. Aliment Pharmacol Ther. 2023;58(11-12):1120-1131.
CrossRef - Ukashi O, Kopylov U, Ungar B, Talan Asher A, Shachar E, Engel T, Albshesh A, Yablecovitch D, Lahat A, Eliakim R, Ben-Horin S; Israeli IBD Research Nucleus (IIRN). Fecal Calprotectin Diagnostic Level Gradient Along the Small Bowel in Patients With Crohn’s Disease. J Crohns Colitis. 2025;19(1):jjae123.
CrossRef - Costa MHM, Sassaki LY, Chebli JMF. Fecal calprotectin and endoscopic scores: The cornerstones in clinical practice for evaluating mucosal healing in inflammatory bowel disease. World J Gastroenterol. 2024;30(24):3022-3035.
CrossRef
Abbreviations List
IBD Inflammatory bowel disease
CRP C-reactive protein
FCP fecal calprotectin
ROC Receiver operating characteristic
Crohn’s Disease (CD)
Ulcerative Colitis (UC)

