
Manuscript accepted on :03-03-2025
Published online on: 28-04-2025
Plagiarism Check: Yes
Reviewed by: Dr. Ilya Nikolayevich Medvedev
Second Review by: Dr. Nicolas Padilla
Final Approval by: Dr. Patorn Piromchai
Mounika Yeladandi1 , Thirupambaram Nataraja Sundaram Uma Maheswari2*,Leela Rani Kandregula3, Malathi Manne4, Nallan Chakravartula Sri Krishna Chaitanya5, Tejaswi Kala6and Mohammed Abidullah7
, Thirupambaram Nataraja Sundaram Uma Maheswari2*,Leela Rani Kandregula3, Malathi Manne4, Nallan Chakravartula Sri Krishna Chaitanya5, Tejaswi Kala6and Mohammed Abidullah7
1 Department of Oral Medicine and Radiology, Panineeya Mahavidyalaya institute of dental sciences and research centre Hyderabad, Telangana, India.
2Department of Oral Medicine and Radiology, Saveetha Dental College and Hospitals, SIMATS, Saveetha University Chennai, Tamil Nadu, India.
3Department of Oral Medicine and Radiology, Sai Vennela Hospital, Tadepalligidem, Andhra Pradesh, India.
4Department of Oral Pathology, Malathi Dental Hub, Hyderabad, Telangana, India.
5Department of Oral Medicine, RAK College of Dental Sciences, Ras AL Khaimah, UAE
6Department of Public Health Dentistry, Tirumala Dental College, Nizamabad, Telangana, India.
7Department of Biomedical Dental Sciences, Faculty of Dentistry, Al Baha University, AL Baha, Saudi Arabia.
Corresponding Author E-mail:umamaheswaritn@saveetha.com
DOI : https://dx.doi.org/10.13005/bpj/3190
Abstract
Background: Early detection of oral cancer plays a pivotal role in improving patient outcomes, as identifying the disease at an early stage markedly increases survival rates. Given the rising incidence of oral cancer in India, there is a growing need to prioritise the implementation of regular screening programs and public awareness campaigns. Educating the community about the signs and symptoms can lead to earlier consultations with healthcare professionals. Additionally, promoting healthy lifestyle choices may help reduce the risk factors associated with oral cancer, ultimately contributing to better overall health outcomes. Non-invasive diagnostic tools are utilised for the screening and early diagnosis of dysplasia and malignancies within the oral cavity. The study aims to evaluate the diagnostic efficacy of a novel device, DrOroscope, in the early diagnosis of dysplasia. Methodology: A prospective cohort study was conducted among 200 participants with the presence of oral mucosal lesions in Hyderabad, India. We selected participants based on the clinical oral examination and documented data on behavioural risk factors such as smoking, tobacco, and alcohol use. We correlated DrOroscope analysis, which uses autofluorescence to detect dysplastic lesions, with DNA ploidy analysis using image cytometry. Statistical analysis was performed using SPSS version 26.0 to assess sensitivity, specificity, and overall diagnostic accuracy. The agreement between the two methods was analysed using Cohen’s Kappa, and the receiver operating characteristic (ROC) curve was used to evaluate the overall diagnostic performance of DrOroscope. Results: The sensitivity and specificity of the DrOroscope were 92.73% and 86.90%, respectively, with a positive predictive value (PPV) of 72.86% and a negative predictive value (NPV) of 96.92%. The overall diagnostic accuracy was 88.50%. Cohen’s Kappa value of 0.276 indicated a fair level of agreement between the two methods. The ROC curve revealed an AUC of 0.898 for the DrOroscope, demonstrating its excellent discriminatory ability. Conclusions: DrOroscope exhibited high diagnostic potential in the early diagnosis of dysplasia. The fact that DrOroscope and DNA ploidy agree on a lot of things suggests that using them together could make diagnoses more accurate. The DrOroscope’s non-invasive nature and real-time analysis make it a promising tool for widespread oral cancer screening.
Keywords
Autofluorescence; Diagnostic accuracy; DNA ploidy analysis; DrOroscope; Non-invasive diagnostics; Oral cancer; ROC curve; Sensitivity; Specificity
Download this article as:| Copy the following to cite this article: Yeladandi M, Maheswari T. N. S. U, Kandregula L. R, Manne M, Chaitanya N. C. S. K, Kala T, Abidullah M. Illuminating Dysplasia: A Novel Approach using DrOroscope for Early, Non-invasive Detection - A Prospective Cohort Study. Biomed Pharmacol J 2025;18(2). |
| Copy the following to cite this URL: Yeladandi M, Maheswari T. N. S. U, Kandregula L. R, Manne M, Chaitanya N. C. S. K, Kala T, Abidullah M. Illuminating Dysplasia: A Novel Approach using DrOroscope for Early, Non-invasive Detection - A Prospective Cohort Study. Biomed Pharmacol J 2025;18(2). Available from: https://bit.ly/42vAQ2Q |
Introduction
Oral cancer remains a significant global health issue, contributing to a substantial portion of cancer-related deaths worldwide. India, with its notably high prevalence of oral cancer, records over 100,000 new cases annually, with an incidence rate of 19 per 100,000 individuals—the highest globally. Oral cancer is the most common cancer among men and the third most common among women in the country, accounting for approximately 13%–16% of all cancers.1 Alarmingly, 95% of these cases are attributed to tobacco use, underscoring the critical need for timely intervention in populations at risk.
Early identification of oral cancer is pivotal in improving patient outcomes, as early-stage detection significantly enhances survival rates. However, conventional diagnostic methods, such as clinical examination and biopsy, are often invasive, time-consuming, and may result in delayed intervention. The rising incidence of oral cancer, particularly in India, presents a formidable challenge to public health systems, with a considerable financial burden on patients. Consequently, there is a growing demand for non-invasive, cost-effective diagnostic tools that can streamline the screening process and improve diagnostic accuracy.2
Preventing, diagnosing, and treating oral cancer in a timely manner is essential in reducing the overall burden of the disease. A big part of reducing the number of cases of oral cancer is teaching people about its causes and risk factors, especially how smoking and drinking can hurt you, as well as how important it is to keep your teeth clean. 2 Traditional clinical methods, such as physical examination, histopathology, biopsy, and imaging techniques, are still used to find oral cancer. However, their flaws, especially when it comes to finding early-stage cancers and how invasive they are, have led to interest in other screening methods. Early diagnosis is key not only to improving survival rates but also to alleviating the physical, psychological, and financial burdens on patients. In fact, prompt detection and treatment of early-stage oral cancer can increase survival probabilities by as much as 90%. As a result, there has been a surge in the development of advanced diagnostic tools designed to enhance early detection and provide non-invasive, efficient alternatives for screening.3
The DrOroscope is a new, non-invasive optical device that uses autofluorescence to find abnormal changes in oral tissues in real time. This lets doctors quickly and easily check out suspicious sores without having to take a tissue sample.The DrOroscope, a commercial fluorescence visualisation device, employs blue light (400-460 nm) to reveal abnormalities in oral tissues that may not be visible under standard white light. 4 Notably, the DrOroscope is a portable intraoral device equipped with three distinct light sources—red, blue, and green-amber. Recently developed in India, this cutting-edge technology provides a practical and accessible tool for clinicians, enhancing the potential for early detection of oral lesions and improving patient outcomes.5 DNA ploidy analysis checks for chromosomal problems inside cells and has shown promise as a way to tell the difference between benign and cancerous growths by measuring the amount of DNA in the nucleus.6 DNA ploidy is a very important biomarker that shows genomic instability, which is one of the main causes of abnormal tissue growth and cancer. We can find genomic instability and dysplasia early on in the development of cancer. This means that targeted therapies can be used sooner, which can improve prognoses and lower the chance of cancer coming back. 7 Techniques such as DNA image cytometry (DNA ICM), flow cytometry (FC), and fluorescent in situ hybridisation (FISH) are employed to assess ploidy and enable early identification of cellular abnormalities. 8
The goal of this study is to find out how well DrOroscope and DNA ploidy analysis work for finding dysplasia and oral cancer early. By looking at these technologies, the study hopes to help improve ways to find oral cancer and make it possible to make diagnoses earlier and with less damage.
Materials and Methods
We conducted a prospective cohort study to assess the diagnostic efficacy of the DrOroscope device in detecting oral dysplasia early. In Hyderabad, India, 200 people from the general population who had oral mucosal lesions and were examined clinically during oral health screening camps were included in the study. Prior to the study, ethical permission was obtained from the Institutional Human Ethical Committee (IHEC) of Saveetha Dental College and Hospital, bearing the ethical number SDC/Ph.D-01/19/05, and all subjects provided informed consent before being included in the study.
Sample size calculation
Sample size was calculated with an expected sensitivity and specificity of 0.9 each and a disease prevalence of 0.2; a precision of ±0.1 is targeted with a 95% confidence level. To account for potential variability and ensure robust results, the expected dropout rate is set at 10%. These parameters lead to a calculated sample size of 193, which we round off to 200 participants to ensure adequate statistical power for the study. 9
Study Design and Participant Selection
All the subjects who participated in the oral health screening camps underwent a thorough clinical examination with a specific focus on those with a high susceptibility to oral cancer, as determined by their demographic and behavioural characteristics. Comprehensive patient histories, which included detailed information about risk variables such as tobacco use and alcohol usage, were documented. A proficient team of dental professionals conducted a thorough clinical oral examination at the screening camps. Afterwards, the team categorised all the participants who had oral mucosal lesions into a cohort.
The criteria for inclusion and exclusion were
Individuals aged 18 years or older, the existence of visibly identifiable oral abnormalities, such as red, white, or combination oral lesions, and willingness to participate were included in the study. The study excluded patients who were not willing and had previously received treatment for oral cancer or had other oral diseases that could interfere with the results.
Diagnostic procedures
Every patient underwent two diagnostic procedures that did not require any intrusive methods.
DrOroscope Examination: We used the DrOroscope equipment to assess lesions for dysplastic alterations. The gadget employs blue light with a wavelength range of 400–460 nm to stimulate autofluorescence in oral tissues. Healthy tissues release a vivid green fluorescence, while dysplastic or malignant tissues exhibit a decrease in fluorescence that appears dark. The inspection was conducted in a dimly lit room to ensure the best possible visualisation of the autofluorescence patterns. This non-invasive technique allowed for a quick evaluation of oral abnormalities in real-time.
DNA Ploidy Analysis: Due to the non-invasive nature of DrOroscope as a diagnostic tool, DNA ploidy analysis has been deemed the preferred method over histopathological biopsy. It has been proven that DNA ploidy is a beneficial way to find dysplastic and cancerous changes in oral lesions because it gives an objective picture of problems with cells. Samples of exfoliative cells were obtained from oral lesions using a cytobrush. We stored the samples in a solution and transported them to a laboratory for DNA ploidy analysis using image cytometry (DNA ICM). The ploidy status (either diploid or aneuploid) was assessed, revealing the existence of dysplasia in the case of aneuploidy.
Statistical analysis
The study used SPSS version 26.0 to analyse data on DrOroscope diagnostic performance and correlations between risk habits and ploidy status. Descriptive and inferential statistics were used to summarise the data, with age as a continuous variable and categorical variables like lesion type and ploidy status represented as frequencies. The Chi-Square test was used for categorical comparison, while Fisher’s exact test was employed for accuracy in small sample sizes. We analysed the efficacy of the DrOroscope using its sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall diagnostic accuracy. The Provider Operating Characteristic (ROC) curve showed how well the diagnostic worked, and the Area Under the Curve (AUC) showed how accurate it was overall. To assess agreement between DrOroscope findings and DNA ploidy status, Cohen’s kappa statistic was calculated. Interpretation of Cohen’s kappa followed Landis and Koch’s criteria. Hypothesis testing was conducted, with a p-value less than 0.05 deemed statistically significant for all tests, and 95% confidence intervals computed when applicable.
Results
The study included a cohort of 200 participants, with 105 males (52.5%) and 95 females (47.5%). The average age of the participants was 54.7 years, with males having a mean age of 54.2 years and females slightly older at 55.3 years. The overall age distribution showed a standard deviation of 13.2 years, with the first quartile at 45.0 years and the third quartile at 65.0 years, reflecting the middle 50% of the sample. The median age for both genders was 55 years, with ages ranging from 20 to 85 years for males and 27 to 80 years for females. This demographic profile provides a balanced representation across gender and age for the study cohort.
The study evaluated the diagnostic performance of the DrOroscope and found its sensitivity to be 92.73% (95% CI: 82.74, 97.14). The specificity was 86.90% (95% CI: 80.44, 91.45).The positive predictive value (PPV) and negative predictive value (NPV) were 72.86% (95% CI: 61.46, 81.88) and 96.92% (95% CI: 92.36, 98.80), respectively. Overall, the diagnostic accuracy of the procedures was 88.50% (95% CI: 83.34, 92.21).
Table 1 presents the agreement between the DrOroscope device and ploidy analysis. It shows that out of 200 cases, the DrOroscope was positive in 70 cases and negative in 130 cases. Among the DrOroscope positives, 51 cases were also positive for ploidy, while 19 were negative. For the DrOroscope negatives, 4 cases were positive for ploidy and 126 were negative. The Cohen’s Kappa value of 0.276 shows that the two methods agree on most things, and the p-value of <0.001 shows that this agreement is statistically significant. This means that the observed agreement is not likely to be due to chance.
Table 1: Agreement of DrOroscope with DNA Ploidy Analysis
| Ploidy | Cohen’s Kappa value | p-value | ||||
| Positive | Negative | Total | ||||
| Dr Oroscope | Positive | 51 | 19 | 70 | 0.276 | <0.001 |
| Negative | 4 | 126 | 130 | |||
| Total | 55 | 145 | 200 | |||
Graph 1 and Table 2 depict the Receiver Operating Characteristic (ROC) curve analysis comparing the DrOroscope to DNA Image Cytometry (ICM) revealed an Area Under the Curve (AUC) of 0.898 with a p-value < 0.001 (95% CI: 0.847, 0.949). Graph 2 illustrates the prevalence of risk behaviours among the study population, highlighting key habits that are linked to oral cancer. Alcohol consumption was the most prevalent risk behaviour, reported by 70.5% of participants. This was followed by pan chewing at 35.0%, tobacco use at 27.5%, and smoking at 26.0%. The least common risk behaviour identified was the use of gutka, with a prevalence of 15.0%. These findings underscore the high rates of substance use, particularly alcohol, in the population, which may significantly contribute to oral cancer risk.
 |
Graph 1: ROC Curve Analysis (Dr Oroscope vs DNA ICM)Click here to view Graph |
Table 2: Area Under the Curve
| Test Result Variables | Area | p-value | 95% CI | ||
| LB | UB | ||||
| Dr Oroscope | 0.898 | <0.001 | 0.847 | 0.949 | |
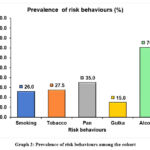 |
Graph 2: Prevalence of risk behaviours among the cohort Click here to view Graph |
Table 3 summarises the comparison of various risk behaviours (smoking, pan, tobacco, gutka, and alcohol use) across different oral disease diagnoses using the chi-square test and Fisher’s exact test, where applicable. Some of the medical terms used to describe the condition were oral submucous fibrosis (OSMF), non-homogenous leukoplakia (NHL), homogenous leukoplakia, pigmentation, keratosis, and oral lichen planus. For smoking, the majority of NHL cases showed higher proportions of non-smokers (38.5%) compared to smokers (32.7%), though the result was not statistically significant (p = 0.18). However, statistically significant differences were found for tobacco (p < 0.001), pan (p < 0.001), gutka (p = 0.004), and alcohol (p = 0.029). In the case of gutka use, OSMF was notably associated with higher consumption (56.7%) compared to non-users (21.2%). Similarly, alcohol consumption showed a significant difference, with NHL and OSMF showing high proportions of users compared to other diagnoses.
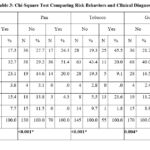 |
Table 3: Chi-Square Test Comparing Risk Behaviors and Clinical DiagnosisClick here to view Table |
* p-value by Fisher’s Exact Test
Table 4 presents the comparison of DNA ploidy results (positive and negative) across different demographic and behavioural factors (gender, smoking, tobacco, pan, gutka, and alcohol use) using the Chi-Square test. Out of 200 participants, 27.5% tested positive for abnormal ploidy, while 72.5% tested negative. No significant association was found between ploidy status and gender (p = 0.362), smoking (p = 0.330), gutka use (p = 0.149), or alcohol use (p = 0.190). However, there was a statistically significant difference in ploidy status with respect to tobacco use (p < 0.001), where 52.7% of tobacco users showed abnormal ploidy compared to only 17.9% of non-users. Additionally, a significant association was observed for pan consumption (p = 0.020), with 33.1% of non-users showing abnormal ploidy compared to 17.1% of users.
Table 4: Correlation of Demographic and Behavioral risk Factors with DNA Ploidy
| Ploidy | p-value | |||||||
| Positive | Negative | Total | ||||||
| N | % | N | % | N | % | |||
| Gender | Male | 26 | 24.8 | 79 | 75.2 | 105 | 100.0 | 0.362 |
| Female | 29 | 30.5 | 66 | 69.5 | 95 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
| Smoking | No | 38 | 25.7 | 110 | 74.3 | 148 | 100.0 | 0.330 |
| Yes | 17 | 32.7 | 35 | 67.3 | 52 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
| Tobacco | No | 26 | 17.9 | 119 | 82.1 | 145 | 100.0 | <0.001 |
| Yes | 29 | 52.7 | 26 | 47.3 | 55 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
| Pan | No | 43 | 33.1 | 87 | 66.9 | 130 | 100.0 | 0.020 |
| Yes | 12 | 17.1 | 58 | 82.9 | 70 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
| Gutka | No | 50 | 29.4 | 120 | 70.6 | 170 | 100.0 | 0.149 |
| Yes | 5 | 16.7 | 25 | 83.3 | 30 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
| Alcohol | No | 20 | 33.9 | 39 | 66.1 | 59 | 100.0 | 0.190 |
| Yes | 35 | 24.8 | 106 | 75.2 | 141 | 100.0 | ||
| Total | 55 | 27.5 | 145 | 72.5 | 200 | 100.0 | ||
Discussion
The surge of oral cancer cases leads to the necessity of early detection of oral cancer, which in turn alleviates the suffering of the patients and improves the prognosis of the disease. The DrOroscope is a non-invasive tool that uses the autofluorescence principle to detect dysplastic changes in oral tissues. By emitting blue light, it highlights abnormal tissues in real-time, offering a rapid and efficient method for screening oral lesions without the need for invasive biopsies.Analysis of DNA ploidy gives us useful information about genomic instability, which is a key part of how cancer grows and can be stopped early. Both technologies aim to enhance the accuracy and timeliness of oral cancer diagnoses, promoting earlier and less invasive interventions.
The present study involved 200 participants with a nearly equal gender distribution, allowing for the generalisation of findings across both genders. The average age of the participants was 54.7 years. The study primarily focused on middle-aged and older adults, who are typically at higher risk for potentially malignant oral disorders and oral cancer. The age range of participants was 20 to 85 years for males and 27 to 80 years for females, enhancing the study’s ability to examine the performance of the device across different life stages.However, the study may not be completely representative because the age range does not include people under 20. People under 20 may still be at risk of oral dysplasia because of habits like smoking cigarettes as a child or genetics. Additionally, the results may not be fully generalisable to populations in other regions or countries with different genetic, environmental, and lifestyle factors.
DrOroscope has demonstrated superior diagnostic performance in the early detection of oral dysplasia among the cohort selected. The device worked much better than autofluorescence-based devices like Velscope, which only worked 75% of the time and only 61.39% of the time. It had a sensitivity of 92.73% and a specificity of 86.90%. A high rate of false positives limited the diagnostic accuracy.10 Overall, the diagnostic accuracy of 88.50% shows that the DrOroscope is a good tool for finding oral cancer and dysplastic changes. In contrast, a handheld fluorescence device had an even lower sensitivity of 43.24%, which means it wasn’t very good at finding oral lesions. 11 These results suggest that the DrOroscope is a more reliable way to find oral dysplastic lesions early on. However, using a combination of different diagnostic methods could make it even more accurate in real life.
We can see from the Receiver Operating Characteristic (ROC) curve analysis that the DrOroscope is effective at finding oral dysplasia and cancer. This is because the AUC value is 0.898 and the p-value is less than 0.001. The high AUC value implies that it can tell the difference between true positive and true negative cases, which makes it easier to find oral dysplasia early. 12 Despite not being associated with disease prevalence, the AUC holds clinical significance. This makes it a reliable way to evaluate diagnostic tools. The high AUC value in this study shows that the DrOroscope is excellent at telling the difference between individuals who actually have oral dysplasia and those who do not.
The findings from the present study suggest a clear association between certain risk behaviours and the prevalence of oral conditions. The prevalence of risky behaviours associated with oral cancer, such as alcohol consumption, tobacco use, pan chewing, and gutta use, remains alarmingly high in certain populations. According to Zhe’s recent study, 70.5% of the people who took part said they drank alcohol, 35.0% said they chewed Pan, 27.5% said they used tobacco, 26.0% said they smoked, and 15.0% said they used Gutka. This is in line with other research that has linked these habits to oral cancer. It has been shown that drinking alcohol, which is already known to raise the risk of oral squamous cell carcinoma (OSCC), raises the risk even more. For drinkers, the risk rises by 1.6 times, and when combined with other factors like HPV, it rises even more.13 At the same time, Laosuwan and Alpana say that smoking is strongly linked to oral cancer, with studies showing a strong link between smoking and changes in the tissues of the mouth. 14, 15 Less extensive studies have linked pan chewing and gutka to elevated cancer risk, particularly in regions where these habits are more prevalent. 16, 17 The high prevalence of these risk behaviours, coupled with inadequate awareness and education, continues to undermine prevention efforts for affected populations. The current study’s analysis of the results of DNA ploidy in relation to different demographic and behavioural factors gives us useful information about the risk of oral cancer. The study revealed that 27.5% of the participants tested positive for abnormal ploidy, indicating a potential connection to lifestyle factors like smoking and alcohol consumption.
Navya and others reported in their research that males are more likely to exhibit DNA aneuploidy, potentially due to higher smoking rates.18 Some studies show a direct link between smoking and DNA damage, while others show no significant link between smoking and aneuploidy in normal mucosa. This shows that smoking has a complex effect on DNA ploidy.19, 20 Das also said that using smokeless tobacco products like tobacco and gutka is linked to a higher rate of oral potentially malignant disorders (OPMD) and aneuploidy.21 According to the study done by Bechstedt et al., alcohol consumption has been shown to enhance the carcinogenic effects of tobacco, though studies specifically examining its direct influence on DNA ploidy remain limited. 22 Some intriguing evidence suggests that quitting smoking may help fix DNA damage. This shows that ploidy status can change, and more research is needed to find out how these factors affect the development of oral cancer.19
The study’s strengths include the use of non-invasive diagnostic methods, the high accuracy and precision of the diagnostic tools, the use of complementary diagnostic methods, the ability to screen people in real time with the DrOroscope, and the focus on people who are at high risk. The study’s strengths make it highly beneficial for early identification and screening, particularly in countries like India where oral cancer is prevalent.
Nevertheless, it is important to take into account specific limitations. The study’s findings may lack full generalisability to broader groups due to the restricted sample size and geographical location of the study. While the relatively high PPV of the DrOroscope suggests that more tests are needed to confirm the results, it also causes the diagnosis and treatment process to be held up. Additionally, there isn’t agreement on the diagnostic methods, which creates uncertainty or calls for more investigations. Future recommendations involve incorporating diverse diagnostic methods; carrying out extensive studies on a larger population; assessing the long-term predictive usefulness of the diagnostic tools; creating cost-efficient DNA ploidy platforms; offering standardised training for the DrOroscope; and conducting comparative analyses with alternative diagnostic technologies. The purpose of these recommendations is to enhance the overall precision, availability, and practicality of the diagnostic techniques used in screening and diagnosing oral cancer.
Conclusion
In conclusion, the integration of advanced diagnostic technology, such as DrOroscope, has ushered in a new era of precision in the early detection and screening of oral cancer. The DrOroscope, on the other hand, has non-invasive autofluorescence-based technology that makes it a useful real-time screening tool for finding abnormal changes in oral tissues. This makes it a promising way to find oral lesions without having to take invasive biopsies. The study showed that the DrOroscope has a lot of potential to make early diagnosis of oral dysplasia more accurate and quicker. The DrOroscope showed a high sensitivity and specificity, thus supporting its role as a viable screening tool for oral cancer. In the end, using advanced diagnostic tools like the DrOroscope along with DNA ploidy analysis could change the way oral cancer is screened by making diagnoses earlier, more accurate, and with less pain. By addressing the current limitations and improving accessibility and training, these technologies can significantly reduce the global burden of oral cancer, particularly in high-risk populations.
Acknowledgement
We are thankful to Dr Ramaraju Devaraju, CEO of Raamah Biocare for his valuable support in providing the device DrOroscope for the research.
Funding Sources
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Author contributions
- Mounika Yeladandi – Conceptualization, Review and editing.
- Thirupambaram Natarja Sundaram Uma Maheswari- Supervision and research methodology.
- Leela Rani and Malathi Manne – Data collection and analysis
- Nallan CSK Chaitanya- Research Methodology, Review and editing the draft.
- Tejaswi Kala- Original draft preparation.
References
- Oral Cancer Information | Oral Cancer Signs & Symptoms. www.indiancancersociety.org. https://www.indiancancersociety.org/oral-cancer/
- Sathishkumar K, Chaturvedi M, Das P, Stephen S, Mathur P. Cancer incidence estimates for 2022 & projection for 2025: Result from National Cancer Registry Programme, India. The Indian Journal of Medical Research. 2022;156(4-5).
CrossRef
- Oral cancer diagnosis and perspectives in India. Sensors International. 2020;1:100046.
CrossRef - Devaraju RR, Muppirala S, GotoorSG, Katne T, Harsha N, Gantala R. IJSR – International Journal of Scientific Research. IJSR – International Journal of Scientific Research. 2019;8(3).
- Efficacy of utility of droroscope for detection of potentially malignant disorders malignant disorders| International Journal of Innovative Science and Research Technology. Ijisrt.com. Published 2023.
- Khanna R, Agarwal A, Khanna S, Basu S, Khanna AK. S-phase fraction and DNA ploidy in oral leukoplakia. ANZ Journal of Surgery. 2010;80(7-8):548-551.
CrossRef - Helena S, Lima R, Weege F. Detection of deletions in 1q25, 1p36 and 1pTEL and chromosome 17 aneuploidy in oral epithelial dysplasia and oral squamous cell carcinoma by fluorescence in situ hybridization (FISH). Oral Oncology. 2021;116:105221-105221.
CrossRef - Annapoorani S, Gururaj N, Balambigai A, Prakash N, Hasinidevi P, Janani V. Assessment of Ploidy Status in Oral Potentially Malignant Disorders – A Systematic Review. Journal of Pharmacy And Bioallied Sciences. 2023;15(1):S86-S92.
CrossRef - Buderer NMF. Statistical Methodology: I. Incorporating the Prevalence of Disease into the Sample Size Calculation for Sensitivity and Specificity. Academic Emergency Medicine. 1996;3(9):895-900.
CrossRef - Sharma A, Sharma A, Avi Kumar Bansal, To Evaluate the Efficacy of Tissue Autofluorescence (Velscope) in the Visualization of Oral Premalignant and Malignant Lesions among High-Risk Population Aged 18 Years and Above in Haroli Block of Una, Himachal Pradesh. Journal of International Society of Preventive and Community Dentistry. 2022;12(3):365-375.
CrossRef
- Abhay K. Kattepur, Deepika Kenkere, C. Deepa, K.S. GopinathA, prospective study to evaluate the efficacy of a fluorescence based hand-held device in the detection of malignant andpotentially malignant disorders of the oral cavity.J.OralMaxillofac.Surg.Med.Pathol.2024.
CrossRef - Al-Labadi L, Evans M, Liang Q. ROC Analyses Based on Measuring Evidence Using the Relative Belief Ratio. Entropy (Basel, Switzerland). 2022;24(12):1710.
CrossRef
- Yang Z, Sun P, Dahlstrom KR, Gross N, Li G. Joint effect of human papillomavirus exposure, smoking and alcohol on risk of oral squamous cell carcinoma.BMC Cancer .2023;23(1).
CrossRef - Laosuwan K, Somngam C, Ngamsanong P, Techachan S, Sangtongthong S, Chamusi N, A Study of Clinical Appearances, Histopathological Features, and Demographic Data in Patients with Oral Potentially Malignant Disorders | OSR : Oral Sciences Reports. Cmu.ac.th. Published 2023.
- Talukdar A, Barman I, Roy D, Das A, Putul Mahanta. Oral Cancer Hazards Related to Tobacco Use and a Transtheoretical Model Assessment of Preparedness of Individuals With Oral Potentially Malignant Disorders to Quit Tobacco Use. Curēus.2023.
CrossRef - Li Y, Wang K, Li X, Zhang L. Association of exposure factors and their causal relationship with oral cancer: A Mendelian randomization study. Clinical oral investigations. 2024;28(4).
CrossRef
- Henrique P, Carolina J, Rezende N, Andreia Borges Scriboni. Development of mouth cancer associated with deleterious habits such as etilism and tabagism: a review. MedNEXT Journal of Medical and Health Sciences. 2023;4(S4).
CrossRef - Navya BN, Najem H, Alva SR. Comparison of cytogenetic abnormality of exfoliative buccal cells among Smokers and Non-smokers. IP Archives of Cytology and Histopathology Research. 2016;2(1):1-4.
- Cruz BS, Schwarzmeier L, Carvalho B. Association between DNA ploidy and micronucleus frequency in chronic smokers and impact of smoking cessation. Human & Experimental Toxicology. 2021;40(8):1374-1382.
CrossRef - Lima CF, Alves MGO, Carvalho BF do C. Is DNA ploidy related to smoking? Journal of oral pathology & medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology. 2017;46(10):961-966.
CrossRef - Das P, Deshukh RS. Assessment of DNA Ploidy in Oral Potentially Malignant Disorders using a VELscope. Jcdr.net. Published 2018.
- Bechstedt N, Pomjanski N, Schramm M, Remmerbach TW. Evaluation of Static DNA Ploidy Analysis Using Conventional Brush Biopsy-Based Cytology Samples as an Adjuvant Diagnostic Tool for the Detection of a Malignant Transformation in Potentially Oral Malignant Diseases: A Prospective Study. Cancers. 2022;14(23): 5828.
CrossRef

