
Manuscript accepted on :07-12-2023
Published online on: 16-05-2024
Plagiarism Check: Yes
Reviewed by: Dr. Cherry Bansal
Second Review by: Dr. Mustafa TÜRKMEN
Final Approval by: Dr. Anton R Keslav
Premalatha Bidadi Rajashekaraiah1* , Sujeeth Kumar Shetty2, Usha Hegde1, Vidyadevi Chandavarkar3, Swetha P4 and Sunila Bukanakere Sangappa5
, Sujeeth Kumar Shetty2, Usha Hegde1, Vidyadevi Chandavarkar3, Swetha P4 and Sunila Bukanakere Sangappa5
1Department of Oral Pathology and Microbiology, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysuru, India.
2Department of Oral and Maxillofacial Surgery, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysuru, India.
3Department of Oral and Maxillofacial Pathology and Oral Microbiology, School of Dental Sciences, Sharda University, Greater Noida, Uttar Pradesh, India.
4Department of Oral and Maxillofacial Pathology, Vishnu Dental College, Bhimavaram, India.
5Department of Prosthodontics and Crown and Bridge, JSS Dental College and Hospital, JSS Academy of Higher Education and Research, Mysuru, India.
Corresponding Author E-mail: drpremalathabr_dch@jssuni.edu.in
DOI : https://dx.doi.org/10.13005/bpj/2892
Abstract
Arteriovenous malformations (AVMs) are uncommon vascular lesions. AVMs are the most serious type of vascular malformations, causing substantial deformity and functional disability. AVMs of the acquired type are rarely confronted in the head and neck region. They may present as a medical emergency while performing dental procedures due to their potential for uncontrollable haemorrhage. Dental professionals should be aware of their potentially fatal complications and management. Accurate diagnosis of AVMs is critical and their management remains challenging. Vascular anomalies involving the lips can negatively impact the functionality and facial appearance. In this article, we discuss a very rare case of acquired AVM of the lower lip triggered by hormonal variation occurring during menopause in a female patient, 58 years of age. There are no reported cases of acquired AVM of the lip with hormonal variation occurring during menopause as the trigger for proliferation of the lesion. An overview of the clinical, etiological, diagnostic and management aspects of head and neck region-acquired AVMs is also presented in this paper.
Keywords
Acquired arteriovenous malformation; Lower lip; Menopause; Sclerotherapy; Vascular malformation
Download this article as:| Copy the following to cite this article: Premalatha B. R, Shetty S. K, Hegde U, Chandavarkar V, Swetha P, Sangappa S. B. Acquired High Flow Arteriovenous Malformation of the Lower Lip Induced by Hormonal Variation- Report of a Rare Case and Review. Biomed Pharmacol J 2024;17(2). |
| Copy the following to cite this URL: Premalatha B. R, Shetty S. K, Hegde U, Chandavarkar V, Swetha P, Sangappa S. B. Acquired High Flow Arteriovenous Malformation of the Lower Lip Induced by Hormonal Variation- Report of a Rare Case and Review. Biomed Pharmacol J 2024;17(2). Available from: https://bit.ly/3UMckFs |
Introduction
Arteriovenous malformations (AVMs) are uncommon vascular lesions consisting of aberrant connections between arteries and veins without normal intervening capillaries.1 AVMs occurring in the head and neck region are rare lesions that affect only 0.1% of the general population, while extracranial AVMs make up only 8.1% of those cases.2,3,4 AVMs may be congenital or acquired.2Most of the oral AVMs are congenital and the acquired type is very rarely reported.5Congenital AVMs are vascular malformations caused by the differentiation failure of the embryonic vascular network.1The most common causes identified for acquired AVMs are trauma and hormonal changes. Oral-acquired AVM can be a fatal benign disease and is chronic and progressive.5
AVMs in the oral cavity can obstruct speech, mastication, and deglutition and frequently get traumatized resulting in ulceration and secondary infections.1Due to the possibility of uncontrolled bleeding during invasive oral operations or examinations, they are among the most infamous vascular lesions.4Spontaneous haemorrhage is also a possible hazard.1They might be asymptomatic or produce functional and cosmetic issues such as asymmetry of the face, discomfort, bone destruction and sudden haemorrhage.6 Accurate diagnosis of AVMs is critical and their management remains challenging.1The likelihood of progression and recurrence is also very high.7Recurrence of the lesion frequently larger than its original size is a common consequence of inadequate excision.5
The lips play an important role in mastication, speech and facial aesthetics. Lip vascular anomalies can adversely impact functionality and facial appearance.8 In this article, we discuss a very rare case of acquired AVM of the lower lip occurring due to hormonal variation in a female patient of 58 years age.
Case report
A female patient of 58‑years age reported to the dental hospital with swelling of the lower lip as the chief complaint. The swelling was painless and started as a peanut-sized lesion 6 years ago and slowly increased to the current size; it bled occasionally on mild manipulation. There was no history of trauma to the lips. The patient reported that the appearance of the swelling coincided with the onset of her menopause phase. Dental, medical and family history were not relevant. On general physical examination, all vital signs were normal.
Extra oral examination revealed a diffuse swelling on the left lateral side of the lower lip measuring approximately 2 ×2×1.5 cm in size. (Figure 1) The vermilion border of the lip appeared slightly erythematous in colour. Intraoral examination of swelling revealed erythematous but intact overlying mucosa. The swelling existed opposite the left mandibular lateral incisor-canine region. Hard tissue examination was not contributory. On palpation, the swelling was non-tender, had diffuse borders, soft consistency and was readily compressible with blanching and pulsations.
 |
Figure 1: Diffuse swelling on the lateral part of the lower lip. |
The lesion was diagnosed provisionally as Haemangioma based on clinical findings and history. Vascular malformations (VM), vascular tumours, pyogenic granuloma, mucocele, and cheilitis granulomatosum were considered differential diagnoses. On routine blood investigations, all values were within the normal range. To confirm diagnosis Colour Doppler Ultrasonography of the lower lip was suggested.
Ultrasonography investigation revealed submucosal soft tissue thickening with tufts of vascular channels showing both arterial and venous flow. The arterial feeder appeared to be a branch of the buccal and superior alveolar arteries. The findings suggested High-flow Arteriovenous malformation of the lower lip. (Figure 2)
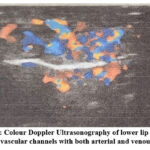 |
Figure 2: Colour Doppler Ultrasonography of lower lip showing tuft of vascular channels with both arterial and venous flow. |
Following the diagnosis of High flow AVM, sclerotherapy was opted as the treatment choice. 1% sodium tetradecyl sulphate was used as the sclerosing agent to induce vascular sclerosis. 1 ml of the sclerosant was directly injected into the centre of the lesion with slow infiltration using an insulin needle. The patient was given post-operative instructions and was prescribed antibiotics and analgesics. She was recalled after a week for a second dose of the sclerosant. The patient decided against further interventions and reported that the lesion had reduced in size and the result was aesthetically satisfactory to her. On examination of the lesion at 1-month follow-up, it had undergone fibrosis and a significant reduction in size. At 6 months follow-up, the lesion remained stable and the patient was comfortable with the result. Since then, the patient has been on regular follow-up with no subsequent consequences.
Discussion
AVMs are vascular malformations of fast-flow type, composed of an abnormal capillary network between the arterial and venous systems, resulting in the shunting of blood. AVMs are dangerous types of VMs, causing substantial deformity and functional disability.9They present in congenital (defective TGF‑β), acquired and familial forms (RASA1 gene mutation).4Terms such as arteriovenous shunt, arteriovenous aneurysm and arteriovenous fistula are also used synonymously to refer to AVMs.1
Clinical features: AVMs can be asymptomatic or can create functional impairments. They can present clinically as compressible pulsatile swellings1with some lesions exhibiting a palpable thrill and can occasionally be auscultated for a bruit.5An audible bruit is not produced by Intraosseous lesions.1The overlying skin may appear erythematous;10or have a true port-wine stain.11Neurosensory alterations can sometimes cause numbness in the affected area.1Local hyperthermia, bleeding, ulceration, impaired function due to arterial steal and ischaemia may also be noted.
In the oral cavity, the anterior portion of the tongue is the most frequent location of occurrence of AVMs followed by the palate, gingiva and buccal mucosa.11Intraoral lesions may be symptomless in many cases.1 Intraosseous VM involving alveolar bone can result in mobile teeth, widening of periodontal ligament spaces, pericoronal bleeding, facial asymmetry and occlusal anomalies.1,5 Acquired AVMs typically occur as asymptomatic, soft or firm pulsatile swellings.5 Our case presented with the typical features of acquired AVMs and was painless, slow growing, pulsatile, diffuse swelling on the lower lip with occasional history of bleeding.
AVMs can progress through four stages and can be graded by severity using the ISSVA (International Society for the Study of Vascular Anomalies) recognized clinical staging system introduced by Schobinger in 1990.5The clinical stages of AVM are presented in Table 1.
Table 1: Clinical stages of Arteriovenous malformations9
|
Stage |
Clinical features |
|
Stage 1- Quiescence |
Pink-bluish stain, local hyperthermia and arteriovenous shunting demonstrated by Doppler.9 (Progression to the next stage is usually induced by trauma, puberty, pregnancy or any interventions like ligation of feeder arteries, incomplete excision and laser treatment)5 |
|
Stage 2- Expansion |
Stage 1 lesion showing enlargement, pulsations, thrill, bruit and tense/tortuous veins. |
|
Stage 3- Destruction |
Stage 2 lesion showing dystrophic skin changes, ulceration, tissue necrosis, bleeding or persisting pain. |
|
Stage 4- Decompensation |
Extensive AVM causing increased cardiac output and heart failure. |
Classification
Vascular malformations are a diverse group of vessel disorders that can involve any part of the vascular system.2VMs can be classified depending on the vessel type involved as capillary, venous, lymphatic, and arteriovenous. Forbes et al. further differentiated VMs into high-flow (arteriovenous) and low-flow lesions (capillary, venous, lymphatic, or combinations thereof) based on the fluid velocity through their system.2,6,10 AVMs are the most aggressive of all VMs, that can cause severe morbidity and deformity.2 Our case was classified as High-flow arteriovenous malformation.
Etiopathogenesis
VMs are a type of vascular anomaly induced by the aberrant formation of vascular elements during embryogenesis.9Few prevailing theories of pathogenesis are TGF-beta signalling defects and a genetic two-hit hypothesis.11,12They are usually congenital but may not be evident clinically; later on, they show growth in proportion to the body volume and do not exhibit spontaneous involution.6The lesion enlarges due to variations in the blood flow and pressure, vascular channel dilatation, shunting and collateral proliferation. These do not exhibit endothelial cell turnover elevation as observed in vascular neoplasms.9 Occasionally, rapid growth can follow after trauma, hormonal changes such as puberty or pregnancy, infections6and iatrogenic injury (biopsy, proximal ligation, or subtotal excision).10VMs may sometimes be associated with underlying systemic conditions. Some AVMs associated syndromes are Parkes-Weber syndrome, Bonnet-Dechaume-Blanc syndrome or Wyburn-Mason syndrome, Capillary malformation-AVM syndrome and Cobb syndrome.11
In the case of acquired AVM, a history of trauma, hormonal imbalance or surgery usually precedes the proliferation of abnormal vasculature. They usually exhibit a single feeder vessel, unlike congenital forms which exhibit several feeder vessels.4 In our case, the patient gave a history of onset of the lip lesion coinciding with the onset of her menopause phase, thus hormonal variation is the most likely trigger for its proliferation. Though hormonal variations occurring during pregnancy and puberty have been implicated as the triggers for acquired AVM, on review of the literature, we did not find any other case with menopause as the cause for acquired AVM.
Histology
AVM is an unencapsulated aggregation of blood vessels within the submucosa.5 They consist of numerous abnormal arteriovenous shunts without normal intervening capillary plexus. These convoluted vessels consist of multiple compartments of arteries and veins devoid of muscle support, endothelial cell proliferation and giant cells.6The lining of the vessels consists of flattened endothelial cells. The arterial internal elastic lamina may be, interrupted, distorted or reduplicated. The thickness of the muscularis mucosa varies significantly. In close proximity, feeder arteries and veins may be observed.5Unlike proliferative phase haemangiomas, VMs do not exhibit high mitotic activity, or elevated concentrations of type IV collagenase and are negative for basic fibroblast growth factor (bFGF), vascular endothelial growth factor (VEGF) and urokinase markers.13,14,15 Inour case, a biopsy was not undertaken to avoid the risk of haemorrhage. Hence the lesion was not histopathologically evaluated.
Differential diagnosis
Vascular neoplasms, other VMs, and other forms of neoplasms are included in the differential diagnosis of AVM. Haemangiomas should not be confused with AVMs.5 They are the most frequent vascular tumours and must be distinguished from vascular malformations as they are managed differently.2Differential diagnoses can also include pyogenic granuloma and hematoma. These are non-pulsatile and do not reveal a combination of arterioles and venules.5Our case was provisionally diagnosed as Haemangioma. Vascular malformations, vascular tumours, pyogenic granuloma, mucocele and cheilitis granulomatosum were considered as differential diagnoses.
Diagnosis
Fine needle aspiration is a diagnostic aid for evaluating AVMs, albeit it may not differentiate between high and low-flow types. This method is safe, effective, and lowers the risk of fatal or extensive haemorrhage associated with biopsies. Recent advances in imaging modalities for evaluating AVMs have been made.5Doppler ultrasound is usually recommended for evaluation1 as it enables quick differentiation between low and high-flow lesions.5 It can be best supplemented with MRI and Computed tomography. Angiography is the gold standard diagnostic imaging modality used for the identification of entire VMs, their contributing vessels, flow characteristics1and dangerous anastomosis.4Colour Doppler Ultrasonography was employed in the diagnosis of our case and it revealed the vessel type, feeder vessel and flow characteristics of the lesion.
Management
Management of AVMs is quite difficult and requires a multidisciplinary strategy1,16which includes interventional radiologists, surgeons, plastic surgeons, anaesthetists and the blood bank. The appropriate management of vascular anomalies depends upon an accurate diagnosis. It is vital to differentiate between haemangiomas and AVMs, and further between high and low-flow types of AVMs.10It is also important to rule out a vascular anomaly when evaluating pulsatile swellings with a history of spontaneous bleeding, before proceeding with any intervention as it may result in uncontrolled and massive haemorrhage.5
When AVM is small and symptomless, close monitoring will suffice, but if it is accompanied by pain, ulceration, haemorrhage, deformity or cardiac issues, active treatment is necessary.5,6,11,17Treatment varies depending on the lesion’s location, extent and flow characteristics. Intraoral lesions can be managed by embolization, sclerotherapy, ligation of vessels, curettage, steroid injection, cryotherapy, laser therapy and surgical resection or a combination of the above modalities.1,6 Combination therapy is the most effective and is considered the gold standard of treatment.7 The most frequently used management technique for AVMs is preoperative sclerosing agents or embolization, followed by complete surgical removal.2
Surgical excision of lips vascular anomalies should be considered with care, since the lips have a distinctive anatomical structure that can be damaged during excision, causing aesthetic issues. Therefore, vascular anomalies should ideally be surgically excised only when they are minor, well-localized, or solitary lesions.8 Regular follow-up with Doppler sonography is suggested as the lesion has a high rate of recurrence.9,18,19
In our case, administration of a single dose of 1% sodium tetradecyl sulphate into the lesion was effective in reducing the lesion size. It provided a non-surgical method and aesthetic recovery of the patient. However, as the patient did not wish for any further interventions, complete involution of the lesion was not achieved. Since then, the patient has been on regular follow-up with no subsequent consequences.
Conclusion
Although acquired AVMs are rarely confronted in the head and neck region, dentists must be aware of them. It is crucial to accurately diagnose oral vascular anomalies with detailed patient history, thorough physical examination and diagnostic workup. Their correct diagnosis and appropriate management need utmost emphasis as they can pose unforeseen medical emergencies due to unmanageable bleeding while performing dental procedures. With the findings of the current case, we conclude that hormonal variations occurring during menopause can act as a trigger for the development of acquired AVM. We also recommend menstrual history be included as part of case history recording in female patients presenting with oral vascular lesions. Sclerotherapy is a feasible treatment method that can effectively resolve vascular malformations. We suggest that early detection, intervention and regular follow-up are required to rule out potential recurrence of vascular malformations.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Acknowledgements
None
Conflict of interest
None
Funding sources
None
References
- Modak R, Mhapuskar A, Hiremutt D, Hebbale M, Gaikwad S. Arteriovenous malformation of the oral cavity: a case report and review of literature. J Pharmaceut Biomed Sci. 2016;6(9):514–517
- Kolarkodi SH, Alnafisah AM. Arteriovenous Malformation of the Lip: A Rare Case Report. Cureus. 2020;12(7): e8979. doi:10.7759/cureus.8979
CrossRef - Javeed S, Khan FA, Awais M, Khan R, Ain RU, Waheed A. Arteriovenous Malformation of Upper Lip – a short cure for gross deformity. PJMHS. 2022;16(3):188-189. doi:10.53350/pjmhs22163188
CrossRef - Mohta A, Gupta D, Jain S. A case of acquired arteriovenous malformation of lip: Clinical and mucoscopic evaluation. Indian Dermatol Online J. 2021;12(1):198. doi:10.4103/idoj.IDOJ_542_19
CrossRef - Pandhare M, Jyoti DB, Mandale M, Suresh RB. Acquired arteriovenous malformation of lip occurring as an occupational hazard: A case report with review of literature. J Oral Maxillofac Pathol. 2018;22(2):287. doi:10.4103/jomfp.JOMFP_4_16
CrossRef - Jafarian M, Dehghani N, Shams S, Esmaeelinejad M, Aghdashi F. Comprehensive Treatment of Upper Lip Arteriovenous Malformation. J Maxillofac Oral Surg. 2016;15(3):394-399. doi:10.1007/s12663-015-0836-8
CrossRef - Shobeirian F, Sanei Taheri M, Yeganeh R, Haghighatkhah H. Huge Arteriovenous Malformation of Upper Lip- A Case Report. Iranian Journal of Otorhinolaryngology. 2020;32(1):49-52. doi:10.22038/ijorl.2019.36848.2207
- Ryu JY, Lee JS, Lee JW, et al. Clinical Approaches to Vascular Anomalies of the Lip. Arch Plast Surg. 2015;42(06):709-715. doi:10.5999/aps.2015.42.6.709
CrossRef - Bhat VS, Aroor R, Bhandary BSK, Shetty S. Traumatic Arteriovenous Malformation of Cheek: A Case Report and Review of Literature. An International Journal of Otorhinolaryngology Clinics. 2013;5(3):173-177. doi:10.5005/jp-journals-10003-1138
CrossRef - Pompa V, Valentini V, Pompa G, Di Carlo S, Bresadola L. Treatment of high-flow arteriovenous malformations (AVMs) of the head and neck with embolization and surgical resection. Ann Ital Chir. 2011;82(4):253-259.
- Manjunath SM, Shetty S, Moon NJ, Sharma B, Metta KK, Gupta N, et al. Arteriovenous Malformation of the Oral Cavity. Case Reports in Dentistry. 2014; Article ID 353580, 5 pages doi:10.1155/2014/353580
CrossRef - Tan S, Marsh P. Arteriovenous Malformation of the Oral Cavity: A Case Report. Oral Hyg Health. 2015;03(01). doi:10.4172/2332-0702.1000174
CrossRef - Van Doorne L, De Maeseneer M, Stricker C, Vanrensbergen R, Stricker M. Diagnosis and treatment of vascular lesions of the lip. British Journal of Oral and Maxillofacial Surgery. 2002;40(6):497-503. doi:10.1016/S0266-4356(02)00153-5
CrossRef - Takahashi K, Mulliken JB, Kozakewich HP, Rogers RA, Folkman J, Ezekowitz RA. Cellular markers that distinguish the phases of hemangioma during infancy and childhood. The Journal of clinical investigation. 1994;93(6):2357-2364.
CrossRef - Kräling BM, Razon MJ, Boon LM, et al. E-selectin is present in proliferating endothelial cells in human hemangiomas. The American journal of pathology. 1996;148(4):1181.
- Churojana A, Khumtong R, Songsaeng D, Chongkolwatana C, Suthipongchai S. Life-Threatening Arteriovenous Malformation of the Maxillomandibular Region and Treatment Outcomes. Interv Neuroradiol. 2012;18(1):49-59. doi:10.1177/159101991201800107
CrossRef - Siripurapu S, Pasupuleti S, Manyam R, Moturi K, Puvvada D N L. Arteriovenous Malformation of Upper Lip- A Case Report with Literature Review. J Adv Med Biomed Res. 2022;30(142):458-462. doi:10.30699/jambs.30.142.458
CrossRef - Richter GT, Friedman AB. Hemangiomas and vascular malformations: current theory and management. International journal of pediatrics. 2012.
CrossRef - Fearon JA. Discussion: extracranial arteriovenous malformations: natural progression and recurrence after treatment. Plastic and reconstructive surgery. 2010;125(4):1195-1196.
CrossRef

