
Manuscript accepted on :27-04-2023
Published online on: 16-06-2023
Plagiarism Check: Yes
Reviewed by: Dr. Tamer Addissouky
Second Review by: Dr. Ahmed Salah
Final Approval by: Dr. Patorn Promchai
Hendry Irawan1* and Putu Anda Tusta Adiputra2
and Putu Anda Tusta Adiputra2
1Surgical Oncology Division, Department of Surgery, Medical Faculty Universitas Udayana, Bali, Indonesia.
2Surgical Oncology Division, Department of Surgery, Medical Faculty Universitas Udayana, Prof. Dr. I.G.N.G. Ngoerah General Hospital, Bali, Indonesia.
Corresponding Author E-mail:hendry.irawan@unud.ac.id
DOI : https://dx.doi.org/10.13005/bpj/2665
Abstract
Background: Malignancy of the thyroid in children was a rare finding and the most pathological finding was papillary thyroid carcinoma. Thyroid carcinoma in children can present with neck lumps or enlarged neck lymph nodes. However, enlarged neck lymph nodes can be a mark of disruption immune system or lymph nodes’ malignancy or metastases from another organ. Case: An eight-year-old girl came to surgical oncology policlinic Prof. Dr. I.G.N.G. Ngoerah general hospital with a tumor on her right neck below the ear lobe and a scar from surgery on her right neck. Previously, she was done surgery on the right neck lump without cytomorphological examination at a regional hospital and it was a papillary thyroid carcinoma. She was referred to Prof. Dr. I.G.N.G. Ngoerah general hospital. She had done total thyroidectomy and right radical neck dissection with sternocleidomastoid muscle removal. The pathological examination was papillary thyroid carcinoma with four metastasis lymph nodes from nine lymph nodes. She had done radioactive iodine and take levothyroxine daily for hormonal suppression. After radioactive iodine therapy, she did not have any malignancy in the surgical field. Conclusion: In children, enlarged neck lymph nodes must be considered as a metastasis lesion of the thyroid. Although thyroid carcinoma is rare in children, we can do fine needle aspiration biopsy to evaluate the origin of enlargement. It can reduce the increase in cancer staging and the risk of metastasis.
Keywords
Children; Metastasis Lymph Node; Neck Lump; Papillary Thyroid Carcinoma
Download this article as:| Copy the following to cite this article: Irawan H, Adiputra P. A. T. Inaccurate Examination of Neck Lump as Regional Metastasis of Papillary Thyroid Carcinoma in Children: A Case Report. Biomed Pharmacol J 2023;16(2). |
| Copy the following to cite this URL: Irawan H, Adiputra P. A. T. Inaccurate Examination of Neck Lump as Regional Metastasis of Papillary Thyroid Carcinoma in Children: A Case Report. Biomed Pharmacol J 2023;16(2). Available from: https://bit.ly/3NfpuH8 |
Introduction
A neck lump or enlarged neck lymph nodes were common in children because the lymph nodes were an immune system. Involvement of neck lymph nodes can be caused by infection, autoimmune, metabolic disease, and malignancy.1 However, enlarged neck lymph nodes can be a mark of metastases from another organ. Thyroid carcinoma is uncommon in children and it can present with or without palpable thyroid enlargement1–5.
Thyroid carcinoma of childhood and adolescence is a rare case finding 1,2, approximately 1.5-3% of all carcinoma in that group in the United States and Europe.2 Incidence of thyroid carcinoma is very rare in early childhood and the case can increase with age.2 Based on an epidemiological survey in the United States, the new case of thyroid carcinoma is 1.8% in people <20 years old.4 Thyroid carcinoma can occur in children who receive external radiation therapy for the treatment of other carcinomas in the neck, autoimmune thyroid disorders, and genetic syndromes.3
Presentation of differentiated thyroid carcinoma (DTC) was thyroid nodule in children and the incidence of clinically palpable thyroid was 1-1.5%.2,4 In the young age population, thyroid nodule was four times the risk of malignancy and DTC was 0.5-3% of all malignancies.2
The most common thyroid cancer in children was papillary thyroid carcinoma3,5 and it usually presents as neck lymph node enlargement, with or without palpable thyroid.4 Thyroid in children usually manifests with advanced disease when diagnosed, compared to adults. Approximately 60-80% of children with DTC had regional lymphadenopathy. The prognosis the DTC in children was good with 10-year mortality <10% and overall survival of 98%, but 20-year overall survival was 95%.6
The diagnosis of thyroid in children is the same as in adults. It is based on history taking, physical examination, laboratory analysis, imaging, cytology with fine needle aspiration biopsy, and histopathology from thyroid after surgery. We will report a pitfall of misdiagnosing management of the thyroid carcinoma in children.
Case Report
An eight-year-old girl came to surgical oncology policlinic Prof. Dr. I.G.N.G. Ngoerah general hospital with a tumor on her right neck below the ear lobe and a scar of biopsy on her right neck (Figure 1). Previously, she went to the regional hospital because there were multiple lumps on right neck below the ear lobe in the last 1.5 years ago. Physical examination on thyroid was on her normal limits. She had neck ultrasonography (Figure 2) and the result was a suspicious malignancy mass of the right thyroid with size 2.71 x 2.19 x 3.1 cm, and right neck lymph nodes enlargement with size 5.31 x 2.87 cm. And then, she underwent a computerized tomography (CT) scan of the neck (Figure 3) to confirm a lesion at the right thyroid and the result was multiple conglomerated lymph node enlargements of the right neck, enhanced with contrast, and suspicious of the malignant lesion. Both thyroid and nasopharynx were within normal limit s. She had done the surgery on the right neck lump without fine needle aspiration biopsy and it was a papillary thyroid carcinoma.
 |
Figure 1: Clinical picture at surgical oncology policlinic Prof. Dr. I.G.N.G. Ngoerah general hospital and scar of biopsy on right neck.
|
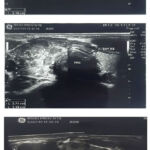 |
Figure 2: Neck ultrasonography.
|
 |
Figure 3: Computerized tomography scan of neck.
|
She was referred to Prof. Dr. I.G.N.G. Ngoerah general hospital and we found a scar from surgery on her right neck (Figure 1). We examined the neck region and thyroid function. The neck examination found painless with multiple lymph nodes and solid consistency in the right neck with the greatest diameter of 5 cm, a scar of biopsy, small enlargement of right thyroid of 1 cm. The thyroid function was within normal limits with free thyroxine (FT4) 1.21 ng/dl and thyroid stimulating hormone (TSH) 2.63 µIU/ml. She had done total thyroidectomy and right radical neck dissection (Figure 4).
 |
Figure 4: Total thyroidectomy and right Radical Neck Dissection. Surgical incision plan (A), right radical neck dissection with sternocleidomastoid muscle removal (B and C), wound closure after surgery (D).
|
The surgical pathology examination was papillary thyroid carcinoma with four metastasis lymph nodes from nine lymph nodes at levels II, III, and IV. She did not consume levothyroxine after surgery because she will undergo radioactive iodine (RAI). The laboratory results before RAI were TSH 192.40 µIU/ml, thyroglobulin 200 ng/ml, and antithyroglobulin antibody 12 IU/ml. One month after the surgery, she underwent RAI using NaI-131 33 mCi. The results were no signs of residual malignancy in the area of surgery, residual functional left thyroid tissue at the level of the thyroid cartilage, and multiple subcentimeter nodules of bilateral lung that are currently not capturing radioactivity should be considered as metastases due to competitive residual functional thyroid tissue. She consumed levothyroxine for hormonal suppression starting from 50 µg per day with target of TSH <0.1 µIU/ml. After thyroid ablation, she was no any local recurrent in surgical field and had no complains. Her schedule of second RAI was next 9 months.
Discussion
Neck lymph nodes are an important part of immune system and it can enlarge because of infection, autoimmune, metabolic disease, and malignancy. Lymph nodes involvement in a variety of conditions is accompanied by a large number of available diagnostic procedures. This can be a challenge for clinicians to establish a proper diagnosis and therapy in pediatric patients through history taking, physical examination, and adjunct examination.1
Adjunct examination can help clinician to confirm the enlargement of neck lymph nodes. It includes laboratory or microbiology test, radiological examination (sonography, CT scan, or magnetic resonance imaging), cytology test, and histopathology test.
Thyroid carcinoma in children has a unique characteristic, in which 36% the size of the tumor at first diagnosis is more than 4 cm and only 9% less than 1 cm. Papillary thyroid carcinoma in children with less than 1 cm size of tumor at diagnosis is only 1.5-3% and it is usually multicentric.2 In addition, it is necessary to evaluate for risk factors that can cause thyroid carcinoma in children, such as a family history of thyroid carcinoma or radiation exposure.
The histological subtypes of thyroid carcinoma in children is similar to adult, there are 90-95% papillary and 5% follicular. Poorly differentiated thyroid carcinoma in children is very rare case, the incidence is about 2-5%. 2,7 Papillary thyroid carcinoma had good prognostic, but with proper treatment, it had risk of recurrence with estimation 14-25% in five years and 34-40% in 10 years.8 Sporadic papillary thyroid carcinoma occurred 1.4% of pediatric carcinoma in United States of America.9
Based on gender, the incidence of carcinoma changes according to age group. The incidence in the 5-14 age group, boys have a 6:1 risk of developing thyroid carcinoma, whereas in the age group more than 14 years, girls are more at risk with 5:2.9 Other characteristic is higher probability of neck lymph nodes metastasis and distant metastasis. In the previous report, 90% of children with papillary thyroid carcinoma had involvement of neck lymph nodes enlargement and 7% of children had distant metastasis (most common site is the lung).2
The most patient of DTC needs total thyroidectomy for the initial surgical approach.2,4,8 American Thyroid Association recommend central neck dissection for patients had central neck lymph nodes metastasis and lateral neck dissection for patients had metastasis lymph nodes on lateral neck.4
Suspicious lymph nodes on lateral neck can be investigated prior surgery by neck ultrasonography and confirmation of metastasis by fine needle aspiration biopsy.4 Preoperative diagnosis of a lump in the neck is necessary to differentiate the presence of lymph node metastases or not. The accurate prediction can help surgeon to select the surgical technique and reduce reoperation.10
The incidence of central cervical metastasis in children was 60-90% macro or microscopic metastasis, so the prophylactic central neck dissection should be performed during total thyroidectomy.8 Other report showed metastatic papillary thyroid carcinoma of lymph nodes without primary carcinoma in thyroid gland. It can be categorized as an occult thyroid carcinoma.11
Other investigation used lymph node ratio (LNR), that is an index by dividing the number of positive lymph nodes by the total of lymph nodes resected. The cut-off value point of 0.45 was useful to predict recurrence in pediatric patients.8 In that research, there were a significant result of recurrence with p = 0.02 on pediatric patient who performed total thyroidectomy and modified radical neck dissection. There were 3 recurrences in 12 patients (25%) with LNR ≤0.45 and 4 recurrences in 4 patients (100%) with LNR >0.45.8
Most cases are recommended RAI after total thyroidectomy, but RAI can not replace the surgery. RAI can be repeated 6-12 months after first treatment. Other modality to treatment is hormonal replacement. The suppressive therapy of thyroid hormone can reduce risk of tumor growth proliferation by TSH. In children, there is still a growth process, so there are side effects of suppression treatment. The side effect of Iodine 131 is temporary loss of salivary flow, change of taste, sialadenitis, and infertility. The accumulative doses of iodine up to 300 mCi does not cause infertility in girl but can cause infertility in < 10% boy. The accumulative doses of more than 800 mCi can cause infertility in 60% girl and > 90% boy.2
Based on this case, we need to sharpen the diagnostic of neck lymph nodes enlargement, especially in children. The history taking, physical examination, and radiological examination are triple instruments to achieve diagnostic. The pathological examination was the gold standard to distinguish the lesion as benign or malignant. We can do fine needle aspiration biopsy as a less invasive method to evaluate neck lymph nodes enlargement.
Conclusion
Inchildren, enlarged neck lymph nodes must be considered as a metastasis lesion of thyroid. Although thyroid carcinoma is rare in children, we can do fine needle aspiration biopsy to evaluate the origin of enlargement. It can reduce the increase in cancer staging and the risk of metastasis. The most common thyroid cancer in children was papillary thyroid carcinoma.
References
- Lang S, Kansy B. Cervical lymph node diseases in children. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2014;13:1–27. doi:10.3205/cto000111
- Vaisman F, Corbo R, Vaisman M. Thyroid carcinoma in children and adolescents-systematic review of the literature. J Thyroid Res. 2011;2011:Article ID 845362. doi:10.4061/2011/845362
CrossRef - Chan CM, Young J, Prager J, Travers S. Pediatric Thyroid Cancer. Adv Pediatr. 2017;64(1):171–190. doi:10.1016/j.yapd.2017.03.007
CrossRef - Francis GL, Waguespack SG, Bauer AJ, et al. Management Guidelines for Children with Thyroid Nodules. Thyroid. 2015;25(7):716–759. doi:10.1089/thy.2014.0460
CrossRef - Verburg FA, Van Santen HM, Luster M. Pediatric papillary thyroid cancer: Current management challenges. Onco Targets Ther. 2017;10:165–175. doi:10.2147/OTT.S100512
CrossRef - Parisi MT, Eslamy H, Mankoff D. Management of differentiated thyroid cancer in children: Focus on the American Thyroid Association pediatric guidelines. Semin Nucl Med. 2016;46(2):147–164. doi:10.1053/j.semnuclmed.2015.10.006
CrossRef - Piromchai P, Ratanaanekchai T, Kasemsiri P. Diagnosis and Treatment of Anaplastic Thyroid Carcinoma. Int J Clin Med. 2012;3(1):69–73. doi:10.4236/ijcm.2012.31016
CrossRef - Rubinstein JC, Dinauer C, Herrick-Reynolds K, Morotti R, Callender GG, Christison-Lagay ER. Lymph node ratio predicts recurrence in pediatric papillary thyroid cancer. J Pediatr Surg. 2019;54(1):129–132. doi:10.1016/j.jpedsurg.2018.10.010
CrossRef - Gayathri BN, Sagayaraj A, Prabhakara S, Suresh TN, Shuaib M, Mohiyuddin SMA. Papillary Thyroid Carcinoma in a 5-Year-Old Child—Case Report. Indian J Surg Oncol. 2014;5(4):321–324. doi:10.1007/s13193-013-0282-3
CrossRef - Agyekum EA, Ren YZ, Wang X, et al. Evaluation of Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma Using Clinical-Ultrasound Radiomic Machine Learning-Based Model. Cancers (Basel). 2022;14(21):5266. doi:10.3390/cancers14215266
CrossRef - Li D, Li J, Zhou J, Xiao Q, Gao H. Metastatic papillary thyroid carcinoma with no primary tumor in the thyroid gland: a case report and review of literature. Transl Cancer Res. 2022;11(1):299–305. doi:10.21037/tcr-21-1780
CrossRef

