
I Gede Bagus Gita Pranata Putra, Samuel Widodo* , I Wayan Wita, I Made Bakta and I Wayan Sudarsa
, I Wayan Wita, I Made Bakta and I Wayan Sudarsa
Department of Cardiology, Faculty of Medicine and Healthcare Warmadewa University, Denpasar City, Bali, Indonesia.
Corresponding Author E-mail:rgitazpranataputra@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2571
Abstract
The incidence of heart failure (particularly heart failure with reduced ejection fraction/HFREF) is increasing over time, especially in developing nations. Based on the most recent data from Riset Kesehatan Dasar 2020 (RISKESDAS/Baseline Health Research), heart failure has become the highest etiology of mortality for patients with heart disease in Bali. Moreover, in patients with chronic kidney disease that have already undergone hemodialysis, the incidence of heart failure is increasing to more than 80% of the population. The correlation between renal dysfunction and heart failure has been known extensively with the term “Cardiorenal syndrome”. However, there is a paucity of literature regarding the prevention of renal dysfunction in heart failure patients and the control of dyslipidemia risk factors for preventing renal dysfunction. Renal dysfunction is not only a cause of morbidity but also a risk factor for heart failure patients' mortality; therefore, prevention is essential for improving heart failure patients' prognosis. We conduct research to compare the lipid profiles of patients with acute renal dysfunction and those without acute renal dysfunction who have heart failure. Based on the results of the lipid profile, we enrolled 70 consecutive heart failure patients with dyslipidemia or non-dyslipidemia. The incidence of renal failure in the group with dyslipidemia is 84.2%. We found that acute renal dysfunction patients had a statistically significant (p<0.05) increase in dyslipidemia compared to non-renal dysfunction patients, particularly with high LDL levels. The association between statin therapy and a low incidence of acute renal failure in patients with heart failure was statistically significant (p<0.05), according to additional findings from our study.
Keywords
Cardiorenal Syndrome; Dyslipidemia; Heart Failure; Renal Dysfunction; Statin Therapy
Download this article as:| Copy the following to cite this article: Putra I. G. B. G. P, Widodo S, Wita I. W, Bhakta I. M, Sudarsa I. W. The Comparison of Lipid Profile in Heart Failure Patients with and without Acute Renal Dysfunction. Biomed Pharmacol J 2022;15(4). |
| Copy the following to cite this URL: Putra I. G. B. G. P, Widodo S, Wita I. W, Bhakta I. M, Sudarsa I. W. The Comparison of Lipid Profile in Heart Failure Patients with and without Acute Renal Dysfunction. Biomed Pharmacol J 2022;15(4). Available from: https://bit.ly/3Whv6ng |
Introduction
The prevalence of cardiovascular events is 10 times higher in patients with renal failure compared to the general population, and it will increase over time in patients with end-stage renal disease.1,2 Moreover, the mortality rate associated with renal failure is highest in patients with cardiovascular disease.3 The cycle (cardio-renal crosstalk) will repeat and worsen in patients who have already been diagnosed with heart failure and dyslipidemia.3
Patients with chronic kidney disease have a high prevalence of dyslipidemia, but the relationship between dyslipidemia and acute renal failure incident in heart failure patients remains controversial. In recent decades, it has become clear that heart failure and renal dysfunction are also related to systemic inflammatory activation and dyslipidemia. The research is conducted to determine whether dyslipidemia is associated with acute renal dysfunction in heart failure patients, as there is considerable inconsistency among studies with different settings regarding the relationship between lipid profile and renal dysfunction in heart failure patients. Heart failure is regarded as a progressive condition alongside renal dysfunction. According to Cole et al., (2018), 20–57% of patients with chronic heart failure and 30–67% of individuals with acute decompensated heart failure have renal impairment. In fact, heart failure events (particularly HFREF) will reduce cardiac output and renal perfusion. An increase in HDL level is associated with a normal glomerular filtration rate and a decreased risk of kidney dysfunction, according to a study conducted in the United Kingdom involving 114 participants in 2020. Furthermore, it has been proved that a 17 mg/dL increase in HDL concentration is equivalent to a 0.8% decrease in eGFR and a low risk for eGFR 60 mL/min/1.73 m2.1,2 Lipid abnormalities in patients with acute renal dysfunction accelerates atherosclerosis, leading to cardiovascular complications.3 Hence our objective is to determine whether dyslipidemia is independently associated with acute renal dysfunction events in heart failure patients.
Materials and methods
This study was approved by the local ethics committee of Sanjiwani General Hospital of Gianyar (PEPK/I/2020). Patients provided written informed consent, and all clinical research was carried out in accordance with the Declaration of Helsinki’s basic principles. The study design is a cross-sectional observational study from January 2020 to December 2021. Participants were 70 heart failure patients that undergo treatment in ED (Emergency Department) and/or ICCU (Intensive Cardiovascular Care Unit). The total sample is using the equation.
The level of significance for the confidence interval (CI) at 95% (zα) is 1.960 and power value (zβ) is 0.842. P-value is determined by dividing the odds ratio that is considered clinically significant by the formula P= R/1+R for value 3/4, and Q value = 1-P is 1/4. Based on this formula, the minimum number of samples is 69.92 rounded up to 70.
The inclusion criteria are patients with signs and symptoms of heart failure according to the Framingham criteria for heart failure, as well as patients with a history of statin use and/or dyslipidemia at the time of their initial presentation. Patients with a previous history of renal failure or dialysis are excluded from this study.
All statistical analyses were performed using version 23.0 of SPSS (IBM, USA). All P-values were calculated using a two-tailed test, and p<0.05 was identified as statistically significant. In the setting of heart failure, Chi-square analysis was used to compare the lipid profiles of patients with and without acute renal failure and multivariate analysis was conducted using multiple regression to evaluate specifically the significance test was determined at p-value < 0.05. Data precision is determined by CI at 95%.
Results and Discussion
Baseline characteristics of participants included age, gender, biochemical measurements, and medical history. The number of samples participating in this study was 70 patients according to the sampling formula, with 48 males and 22 females. The sex distributions are shown in the table below. We measured biomedical parameters using a biochemical automatic enzyme analyzer, including creatinine, blood urea nitrogen (BUN), fasting blood glucose (FPG), TC, TG, high-density lipoprotein (HDL) and LDL in the Clinical Laboratory Sanjiwani Hospital. All covariates were measured once at baseline.
Table 1: Sex Distributions
| Sex | Numbers | Percentages (%) |
| Female | 22 | 31.4 |
| Male | 48 | 68.6 |
| 70 | 100 |
The baseline characteristic according to lipid profile status was shown in the table below. Meanwhile, patients with dyslipidemia were 59 people out of 70 samples (84.3%), and males predominate with dyslipidemia (42 cases). Similar results were founded in previous epidemiological data that show the incidence of dyslipidemia is more common in men. The number of patients with acute renal failure was 62 people (88.6%) with the majority of male. And the number of patients who previously used statin therapy amounted to 24 patients (34.3%). All the characteristics of the lipid profile and acute renal failure event in the study are described in Tables 2 and 3 below.
Table 2: Lipid Profile Characteristic
| Dyslipidemia | Numbers | Percentages (%) |
| Yes | 59 | 84.3 |
| No | 11 | 15.7 |
| 70 | 100 |
Table 3: Acute Renal Failure Characteristic
| Acute Renal Failure | Numbers | Percentages (%) |
| Yes | 62 | 88.6 |
| No | 8 | 11.4 |
| 70 | 100 |
Our research also shows among 62 patients enrolled that the number of patients taking statins (not considering the type and the dosage of statin medication) while had acute renal failure was 21 patients (33.8%), while those who were not taking statins and had acute renal failure were 41 patients (66.1%). Furthermore, from the data analysis result, it was found that there was a relationship between statin therapy with attenuated risk of acute renal failure in heart failure patients (p<0.05) which is shown in table 4 below. Recent studies in which high-intensity statin therapy was used more frequently showed that statins increase the risk of acute renal failure. An example the last large multinational observational study by Dormuth, et al. 2013 (n=2.008.003) shows an increased risk of acute renal failure within two years of statin initiation among high-intensity statin users (high-intensity statin defined by daily doses of ≥10 mg rosuvastatin, ≥20 mg atorvastatin, or ≥ 40 mg simvastatin) compared to users of statin at lower potency, but only among people without CKD at baseline.
Table 4: Patient with Acute Renal Failure and Statin Therapy
|
Acute Renal Failure |
||||
| Yes | No | Total | P Value | |
| Statin Yes | 21 | 3 | 24 | |
| No | 41 | 5 | 46 | 0.005 |
| Total | 62 | 8 | 70 | |
In this study, 55 patients with dyslipidemia also had acute renal failure, and as shown in tables 5 and 6, there is a relationship between dyslipidemia and acute renal failure. In addition, the data analysis revealed a correlation between dyslipidemia and an increased risk of acute renal failure in patients with heart failure, p<0.05. Multiple comparisons between non-ARF and ARF lipid profiles are given in Table 7.
Table 5: Patient with Acute Renal Failure and dyslipidemia
| Acute Renal Failure | |||
| Yes | No | Total | |
| Dyslipidemia Yes | 55 | 4 | 59 |
| No | 7 | 4 | 11 |
| Total | 62 | 8 | 70 |
Table 6: Association between Dyslipidemia and Acute Renal Failure
| Acute Renal Failure | |||||
| Dyslipidemia | HDL | LDL | Total Cholesterol | TG | |
| P Value | |||||
| Acute Renal |
0.004 |
0.839 |
0.041 |
0.840 |
0.10 |
| Failure | |||||
The concentrations of Total Cholesterol (TC), High-Density Cholesterol (HDL-C), Low-Density Cholesterol (LDL-C) and Triglycerides (TG) were shown in table 7. All statistical analyses were performed using SPSS, version 23.0 (IBM, USA). All p-values were two-tailed, and p<0.05 was considered to indicate statistical significance. Multivariate linear regression analysis was used to evaluate the association between dyslipidemia and acute renal failure event.
Table 7: Multiple comparisons of lipid profiles between non-ARF and ARF
| Parameters | Non ARF | ARF | p-Value |
| Total cholesterol (mg/dl) | 184.10 + 20.2 | 186.2 + 21.3 | >0.005 |
| HDL-C (mg/dl) | 40.34 + 5.20 | 41.23 + 4.3 | >0.005 |
| LDL-C (mg/dl) | 119.51 + 22.3 | 150.34 + 25.2 | <0.005 |
| Triglyceride (mg/dl) | 123.2 + 28.3 | 119.2 + 30.3 | >0.005 |
From this result, can be concluded that dyslipidemia is associated with a high incidence of acute renal failure. In the multiple regression analysis, a high LDL-C level was the most significant predictor of acute renal failure (p<0.05). Dyslipidemia is commonly known for patients with chronic kidney disease but shows varying patterns in various populations of patients with chronic kidney disease. Similar research was also proposed by Rahmawati et al., (2021), nevertheless, the study correlates dyslipidemia with kidney failure in general, without looking for dyslipidemia with acute renal failure in heart failure patients setting. The study was conducted in Dr. Soetomo General Public Hospital Surabaya and involved 68 subjects. According to the study, 37% of study participants had higher than normal levels of triglycerides and total cholesterol. On the other hand, roughly 60% of the individuals had lower levels of HDL cholesterol and higher levels of LDL and non-HDL cholesterol. According to statistical calculations, the female group’s mean value for total cholesterol, LDL cholesterol, and non-HDL cholesterol was considerably higher (p<0.05).4
Another study done by Farhan et al., (2016) aimed to analyze the correlation between stages 4 and 5 of chronic kidney disease with the incidence of dyslipidemia at Fatmawati Central General Hospital Jakarta in 2016.5 The design was a cross-sectional study using a simple randomized technique. Data were collected using the patient’s medical record. 80 people were chosen as the subject of the study, for the population were patients with chronic renal failure at Fatmawati Central General Hospital in 2016. The results showed that the majority of the subject (i.e., 22 subjects 73.33%) with stage 4 chronic kidney disease had a low level of LDL, while subjects with stage 5 chronic renal disease had high levels of LDL as many as 36 patients (72%). Stages 4 and 5 of chronic renal failure were significantly correlated with the incidence of dyslipidemia (p=0.002) according to the findings of the bivariate analysis with the Chi-square test (Farhan et al., 2016).5
Pritee et al., (2017) conduct research similar to ours on the prevalence of dyslipidemia in patients with acute renal failure. The study found that individuals with acute renal failure had significantly (p<0.05) higher levels of total cholesterol, TG, and VLDL than those without acute renal failure. Patients with acute heart failure had extremely low HDL levels. However, it was discovered that the incidence of acute renal failure was connected with high total cholesterol, high LDL, and low HDL.6
Acute renal failure incidence is increased by dyslipidemia due to abnormal lipolysis, to a decrease in the activity of lipoprotein lipase and hepatic TG lipase enzymes up to 50% of normal function. 7 Another pathomechanism that explains the correlation of dyslipidemia with acute renal failure is the role of dyslipidemia in kidney injury in experimental mice subject fed to a high-cholesterol diet.7 The study showed the presence of sclerotic glomeruli in mice with a high-cholesterol diet compared to mice without a high-cholesterol diet.8 Furthermore, in mice models with a high-cholesterol diet, lipid deposits in the glomeruli were found to be correlated with a high level of proteinuria.8 This lipid deposition can directly damage the glomerular basalis membrane that stimulates and activates mesangial cells.7,8 The mesangial cells subsequently release chemokines that trigger a proinflammatory cascade and profibrotic processes, creating a continuous cycle for the progression of acute renal failure in dyslipidemia patients.7,8
 |
Figure 1: Complex pathogenesis of acute renal failure in patients with heart failure (Hatamizadeh P, Fonarow GC, 2013).12 |
The correlation between dyslipidemia and increased inflammatory response (low-grade chronic inflammation) is also suspected as another cause.9 The cardiorenal syndrome involves complex interactions at a molecular level, causing inflammatory processes in blood vessels, atherosclerosis process, cardiac fibrosis, and hypertrophy. 9 Over the past several decades, it has been shown that systemic inflammatory activation has had a significant impact on patients with chronic renal failure and heart failure. The inflammatory process provides protection and accelerates the healing process from a physiological aspect.9,10 It is possible for the same mechanism to produce the opposite consequence, which should give protection and speed up recovery but instead causes injury and organ damage. Heart failure and chronic kidney failure, or both, have a reciprocal effect and progressively decrease both functional state and prognosis.9,10
From the hemodynamic side, the pathogenesis of acute renal failure in patients with heart failure were cause fluid retention physiologically it should work at low pressures, and when these two diseases happened, it’s pathophysiologically, forced e fluid on venous pressure and interstitial space rise several times above the normal value.7,8 In this high-pressure environment, it will cause biomechanical stress for blood vessels stretching and even more, tissue congestion will exacerbate the inflammatory process and further worsen the functional structure of vital organs such as the heart, blood vessels, and kidneys.9 An increase in systemic inflammatory biomarkers correlated with a decrease in functional and clinical severity in coronary artery disease and chronic kidney disease, and otherwise, a decrease in these biomarkers correlated with better clinical outcomes.9,10 The circulating biomarker molecule is not inert but a bioactive molecule that exerts direct and often causes overlapping adverse effects on the affected tissue.7-10
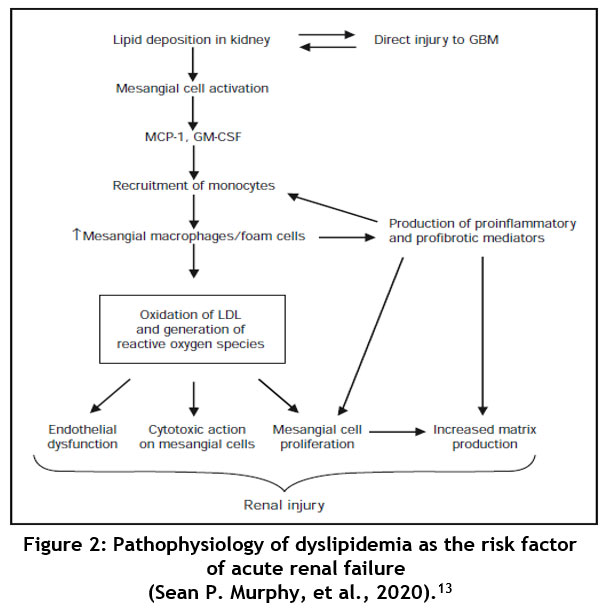 |
Figure 2: Pathophysiology of dyslipidemia as the risk factor of acute renal failure |
(Sean P. Murphy, et al., 2020).13
Conclusion
In conclusion, we found that dyslipidemia (particularly high LDL-C level) is associated with acute renal failure events in individuals with heart failure setting. And patients who are receiving statin therapy are associated with lower incidence of acute renal failure in the setting of heart failure condition. This demonstrated that uncontrolled LDL-C level might contribute to the propensity of renal dysfunction, so as dyslipidemia therapy can be recommended for a patient with heart failure, focusing on LDL-C levels that reduce the risk of acute renal failure in patients who are suffering from heart failure.
Conflict of Interest
There is no conflict of interest.
Funding Sources
There is no funding Sources
References
- Piotr Ponikowski. 2016. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal (2016)37, 2129–2200
CrossRef - Hong Zhang, Shuang Shi, Xiu Juan Shao. 2019. Association Between Lipid Profile and Renal Dysfunction in The Heart Failure Kidney Blood Press Res 2019;44:52–61
CrossRef - Liffert Vogt, Sripal Banglore, Rana Fayyad. 2019. Atorvastatin Has a Dose-Dependent Beneficial Effect on Kidney Function and Associated Cardiovascular Outcomes: Post Hoc Analysis of 6 Double-Blind Randomized Controlled Trials. J Am Heart Assoc
- Rahmawati Siti, et , 2021. Dyslipidemia in Chronic Kidney Disease Patients at Dr. Soetomo Hospital Surabaya. Media Penelitian dan Pengembangan Kesehatan, Vol. 31 No. 1, Maret 2021, 9 – 16
CrossRef - Wibawanto Farhan et al., 2016. Corelation of CKD Stage 4 and 5 with Dyslipidemia on Chronic Kidney Disease Patients in Fatmawati Genaral Hospital. Jurnal Profesi Medika Vol. 12, No. 2018
- Pritee Gopalrao Pendkar, Tushar Vaijanathrao Bansode. 2017. Dyslipidemia in Acute Renal Failure (ARF). International Journal of Clinical Biochemistry and Research, October- December 2017;4(4):354-356
- Rajiv 2007. Effects of Statins on Renal Function. Mayo Clin Proc. 2007;82(11):1381-1390
CrossRef - Ter Maaten JM, Damman K, Verhaar MC, Paulus WJ, Duncker DJ, Cheng C, van Heerebeek L, Hillege HL, Lam CS, Navis G, Voors AA: Connecting heart failure with preserved ejection fraction and renal dysfunction: the role of endothelial dysfunction and Eur J Heart Fail 2016;18:588-598.
CrossRef - Lanktree MB , Thériault S, Walsh M, Paré G: HDL Cholesterol, LDL Cholesterol, and Triglycerides as Risk Factors for CKD: A Mendelian Randomization Study. Am J Kidney Dis 2018;71:166-172
CrossRef - Ter Maaten JM, Damman K & Verhaar MC 2016. Connecting heart failure with preserved ejection fraction and renal dysfunction: the role of endothelial dysfunction and inflammation. Eur J Heart Fail;18:588-598.
CrossRef - Victoria C & Marian G 2008. Oxidative stress and inflammation, a link between chronic kidney disease and cardiovascular disease. Kidney International 74 (Suppl 111), S4–S9
CrossRef - Hatamizadeh P, Fonarow GC & Budoff MJ. Cardiorenal syndrome: pathophysiology and potential targets for clinical management. Nat Rev Nephrol. 2013;9:99–111. doi: 10.1038/nrneph.2012.279
CrossRef - Murphy S 2020. Inflammation in Heart Failure. Journal of The American College of Cardiology Vol. 75, No. 11
CrossRef

