
Tamil selvan G1 , Kala Samayan1, Kumar J S2 Venkataraman P3, Muthukumaran G1, Ambethkar S1 and Balakrishnan D1
, Kala Samayan1, Kumar J S2 Venkataraman P3, Muthukumaran G1, Ambethkar S1 and Balakrishnan D1
1Department of Audiology and Speech-Language Pathology, SRM IST, Kattankulathur, Chengalpattu (Dt), Tamil Nadu, India.
2Department of General Medicine, SRM IST, Kattankulathur, Chengalpattu (Dt), Tamil Nadu, India
3Department of Research, SRM IST, Kattankulathur, Chengalpattu (Dt), Tamil Nadu, India.
Corresponding Author E-mail: kalas1@srmist.edu.in
DOI : https://dx.doi.org/10.13005/bpj/2525
Abstract
Diabetes Mellitus (DM) appears to be a risk factor for hearing loss. Meta-analyses of cross-sectional studies reported that diabetes had a greater risk of hearing impairment. Hearing loss and hemoglobin A1c (HbA1c), a glycemic management biomarker, have been linked in a few studies. HbA1c and hearing impairment as measured by a pure-tone average threshold of frequencies (500 Hz, 1 kHz, and 2 kHz), while the other two found a link between HbA1c and high-frequency hearing impairment. The goal of this study is to see if the amount of HbA1c level is linked to the occurrence of hearing loss. Participants were 430 of both genders between the ages of 21 to 60 years and based on the duration of HbA1c level. Results indicated that the higher HbA1c level patient had high-frequency hearing loss when compared to speech frequencies in both ears. As the HbA1c level increases an increase in the high-frequency hearing loss was also noticed. A positive correlation exists between the duration of diabetics and high-frequency hearing loss. Moreover, when diabetic duration increases, the hearing loss is more affected in extended high frequency, high frequency followed by speech frequency among uncontrolled DM than controlled DM in both ears. These findings suggest that proper glycemic management might help avoid diabetic hearing loss.
Keywords
Diabetic Mellitus; Duration; High-Frequency Hearing Loss; HbA1c
Download this article as:| Copy the following to cite this article: Selvan G. T, Samayan K, Kumar J. S, Venkataraman P, Kumaran G. M, Ambethkar S, Balakrishnan D. Effect of HbA1c Level on Hearing Sensitivity Among Patients with Diabetic Mellitus. Biomed Pharmacol J 2022;15(4). |
| Copy the following to cite this URL: Selvan G. T, Samayan K, Kumar J. S, Venkataraman P, Kumaran G. M, Ambethkar S, Balakrishnan D. Effect of HbA1c Level on Hearing Sensitivity Among Patients with Diabetic Mellitus. Biomed Pharmacol J 2022;15(4). Available from: https://bit.ly/3SnNV5X |
Introduction
Hearing is an essential element of everyday living, and its loss has a major impact on quality of life owing to decreased communication and functional abilities (Lin FR et al., 2011; Wilson et al., 2017)1,2. According to WHO estimates, around 360 million individuals, or 5% of the world population suffer from hearing loss, and this incidence is rising due to the growing older Adults (Deafness and Hearing Loss, 2020)3.
Hearing loss in adults can be caused by a variety of reasons, including age, genetics, neurological illnesses, vascular causes, metabolic problems, ototoxic medicines, noise, and diabetes mellitus. But age-related hearing loss cannot be reversed, it is critical to identify factors that may be avoided. Diabetes mellitus (DM) is a non-communicable endocrine condition that causes significant damage throughout the body. Diabetes is a chronic illness that, in its advanced stages, produces a variety of organ malfunctions or impairments in individuals with DM. Among the long-term consequences of diabetes include cardiovascular and peripheral vascular illnesses, neuropathy, nephropathy, retinopathy, and cerebrovascular problems (International Diabetes Federation, 2019)4.
Diabetes mellitus appears to be a risk factor for hearing loss, according to research. Subjects with diabetes had a greater risk of hearing impairment, according to meta-analyses of cross-sectional studies (Horikawa et al., 2013)5. Hearing impairment and hemoglobin A1c (HbA1c), a glycemic management measure, have been linked in three studies. (Michikawa et al., 2014; Kang et al., 2016)6,7. One of these studies found a positive dose-response connection between HbA1c and hearing impairment as measured by a pure-tone average threshold of mostly low frequencies, (Kim et al., 2017)8. Whereas the other two found that HbA1c was linked to high-frequency hearing impairment (Michikawa et al., 2014; Kang et al., 2016)6,7.
Hemoglobin A1c (HbA1c) is a non-enzymatic and slow glycolysis product of hemoglobin in the blood that is used to monitor long-term glycemic management in diabetics and to diagnose non-diabetic people. It’s also thought to represent the quality of patient follow-up control and suggest the danger of diabetic complications. Although HbA1c is less than 6% in those without diabetes, it can rise to more than 10% in people with uncontrolled diabetes (Schnell et al., 2017)9.
Microangiopathy is thought to be the primary cause of diabetic retinopathy, nephropathy, and neuropathy (Sen et al., 2015; Ooley et al., 2018; & Nemati et al., 2018)10,11,12. Microangiopathy is also thought to be a major cause of hearing loss in diabetics (Cohen Atsmoni et al., 2018)13. There is a link between HbA1c and hearing loss, according to research (Nagahama et al., 2018)14. By comparing the audiometric characteristics of the two groups, we were able to discover a link between HbA1c and hearing loss.
Sharma et al. (2022)15 Hearing loss was reported on higher frequencies, according to There was a link between hearing loss and HbA1c, which was strongest in the 10-13.9 percent range, although not statistically significant. While some studies found that diabetic people had a higher risk of hearing loss, others found no link between diabetes and hearing loss. By comparing the audiometric characteristics of the groups, we were able to discover a link between HbA1c and hearing loss. In HbA1c and auditory systems has been a lack in literature. Based on a few pieces of literature we aimed, to be a there is any relationship between the HbA1c and the degree of hearing loss among the controlled and uncontrolled DM.
Methods and Materials
In this study, 430 individuals had their HbA1c test values monitored and were taken for an audiological examination. The study excluded individuals with chronic otitis, ototoxicity, acoustic damage, cancer, prior ear surgery, neurological illness, and mental development abnormalities. Patients included in the age range of 21 to 60 years. Participants more than 60 years old were excluded from the research to rule out presbycusis and genetic predisposing factors. The research population of 430 participants was separated into two groups based on their HbA1c levels. Subjects with HbA1c levels of >5.5 to 6.9 were classified as Group 1 (Controlled Diabetes Mellitus); those with values of 7.0 and above were classified as Group 2 (Uncontrolled DM). The correlation between HbA1c blood test results and pure tone audiological test findings was statistically analyzed.
The Piano Inventies audiometer was used to conduct pure tone audiometry tests with frequency ranges of 250Hz, 500 Hz, 1 kHz, 2 kHz, 4 kHz, 8 kHz, 9 kHz, 10 kHz, 12 kHz, 14 kHz, and 16 kHz. The right and left ear threshold levels were tested individually. Pure tone averages of the subjects were determined for both ears. For each criterion, such as age and duration of DM, it was determined if there was a significant difference between the HbA1c groups of controlled DM and Uncontrolled DM.
Table 1: Pearson Chi-Square Tests of speech frequency and high frequency of both ears in controlled DM.
| Pearson Chi-Square Tests | |||||
| Gender | Severity | Age | DM age (months) | ||
| Right Speech Frequency (RSF)
500 Hz, 1kHz & 2kHz |
Chi-square | 1.128 | 2.497 | 22.995 | 16.276 |
| Df | 4 | 4 | 12 | 12 | |
| Sig. | .890a,b | .645a,b | .028a,b,* | .179a,b | |
| Right High & Extended High Frequency (RHF)
4kHz – 16 kHz
|
Chi-square | 2.494 | 5.864 | 29.335 | 25.537 |
| Df | 5 | 5 | 15 | 15 | |
| Sig. | .777a | .320a | .015a,b,* | .043a,b,* | |
| Left Speech Frequency (LSF)
500 Hz, 1kHz & 2kHz |
Chi-square | .456 | 6.301 | 8.749 | 7.573 |
| df | 4 | 4 | 12 | 12 | |
| Sig. | .978a | .178a | .724a | .818a,b | |
| Left High & Extended High Frequency (LHF)
4kH – 16 kHz |
Chi-square | 4.894 | 5.067 | 16.724 | 11.268 |
| df | 5 | 5 | 15 | 15 | |
| Sig. | .429a,b | .408a,b | .336a,b | .733a,b | |
Table 2: Pearson Chi-Square Tests of speech frequency and high frequency of both ears in Uncontrolled DM.
| Pearson Chi-Square Tests | |||||
| Sex | Severity of HbA1c | Age | Diabetic Months | ||
| Right Speech Frequency (RSF)
500 Hz, 1kHz & 2kHz |
Chi-square | 10.367 | 146.892 | 33.360 | 28.494 |
| Df | 5 | 10 | 15 | 15 | |
| Sig. | .065 | .000a,b,* | .004* | .001a,b,* | |
| Right High & Extended High Frequency (RHF)
4kHz – 16 kHz |
Chi-square | 6.583 | 6.092 | 38.499 | 58.594 |
| Df | 6 | 12 | 18 | 18 | |
| Sig. | .361a,b | .004a,b | .003a,b,* | .000a,b,* | |
| Left Speech Frequency (LSF)
500 Hz, 1kHz & 2kHz |
Chi-square | 5.239 | 20.262 | 31.078 | 12.685 |
| Df | 4 | 8 | 12 | 12 | |
| Sig. | .264 | .005a,b,* | .002a,* | 0.003a,b | |
| Left High & Extended High Frequency (LHF)
4kH – 16 kHz |
Chi-square | 8.192 | 12.326 | 37.778 | 18.034 |
| Df | 6 | 12 | 18 | 18 | |
| Sig. | .224a,b | .004a,b | .003a,b,* | .004a,b | |
Results and Discussion
The present aimed to study the relationship between the HbA1c level and the degree of hearing loss among controlled and uncontrolled diabetic Mellitus. The results have been discussed with HbA1c level, duration, and severity of the hearing loss.
Controlled DM
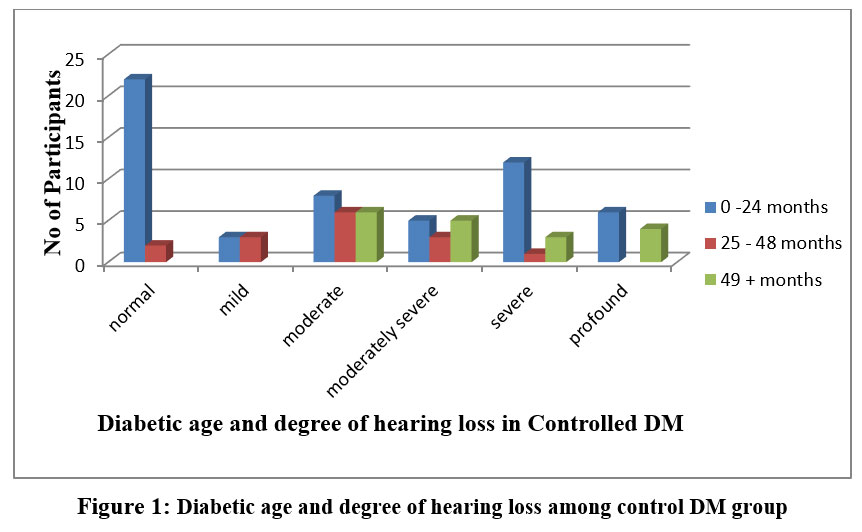 |
Figure 1: Diabetic age and degree of hearing loss among control DM group. |
Figure 1 shows that when the diabetic age increases the severity of hearing loss also increases among controlled DM
The present study found that to be a relationship between the length of the diabetic Mellitus and hearing loss, those with diabetes who have had the disease for longer than 10 years have higher hearing loss, particularly of the sensorineural variety. Contrarily, some other writers hypothesized that the length of the DM is substantially connected with hearing loss, meaning that the longer diabetes is present, the greater the risk of hearing loss stated by Uju IM et al. (2021)16.
Table 1 shows that there is a significant age difference (p<0.05) and duration (months) of controlled DM (p<0.05) in the Right high frequency. On the other hand, there is no significant difference between age and diabetic duration of Right speech frequency. But there is a significant difference in the age of the participants. There is no significant difference between age and diabetic duration of the left speech and high frequency among controlled DM. The present finding concurrent with past findings done by Horikawa et al. (2013)5 that the relationship between HbA1c level and diabetes problems, as well as a link between hypoglycemia and its diabetic complications. Moreover, diabetics who have adequate glycemic management may prevent diabetic-related hearing loss.
Uncontrolled DM
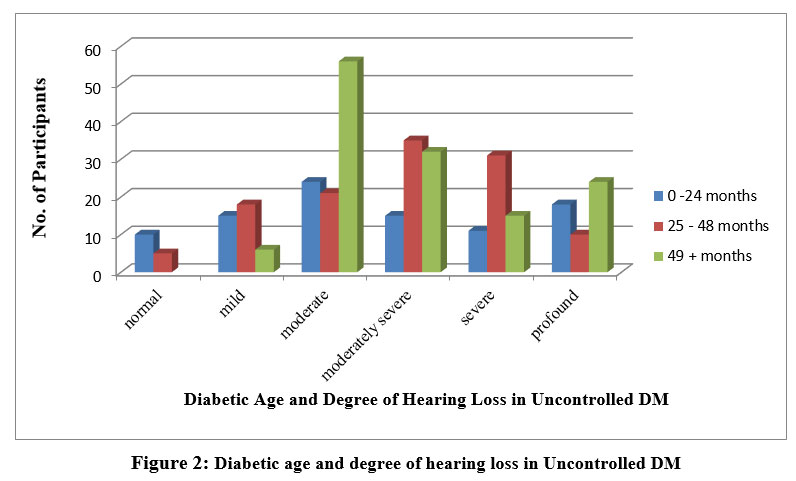 |
Figure 2: Diabetic age and degree of hearing loss in Uncontrolled DM |
The above Figure 2 shows that the high-frequency hearing loss increased when compared to speech frequency in both ears. When the diabetic duration has increased the severity of hearing loss (moderate to profound) is also increased among Uncontrolled DM in both ears. The present finding agrees with past findings were done by Kurien et al. (1989); Tay et al. (1995); Panchu et al. (2018);17,18,19 that the considerable link between HbA1c level and hearing loss and those with poorly managed diabetes suffer severe hearing loss due to high HbA1c levels.
These findings reveal a link between HbA1c levels in the blood and sensorineural hearing loss. According to this concept, the degree of diabetes might be a deciding factor for hearing loss. We compared the effects of diabetes on the cochlear system by performing a complete blood HbA1c (uncontrolled DM) level and audiological examination.
Above table 2 shows that, a significance of age (p = 0.004), duration of DM (months) (p 0.001) and severity of HbA1c (p 0.000) in Right speech frequency and high frequency hearing loss highly significance of HbA1c (p 0.004), Age of the participant (p 0.003) & duration of DM (p 0.000) in right ear. In similar table shows that a significant difference was observed in age (p-value 0.002), duration of DM (months) (p 0.003), and severity of HbA1c (p 0.005) in left speech frequency and high-frequency hearing loss highly significance of HbA1c (p0.004), Age of the participant (p 0.003) & duration of DM (p 0.004) in the left ear of uncontrolled DM by using multiple comparisons (Pearson Chi-Square Tests).
There is a paucity of research on the relationship between diabetes and hearing impairment symptoms (Ooley C, et al. 2017; Nagahama S et al 2018)11,14. There are studies documenting hearing loss in all frequencies. The current study shows that there is an association between the severity of HbA1C (controlled DM & uncontrolled DM) and hearing loss (speech frequency & high frequency) among diabetics Mellitus. In addition to research defining diabetes-related hearing loss as progressive, bilateral, and affecting high frequencies (Ren et al. 2017; Gupta et al. 2019)20,21.
According to Cohen Atsmoni S et al. (2019)13, reported that diabetes-related hearing loss would manifest itself mostly at high frequencies, as high-frequency specific parts of the cochlea may be more sensitive to ischemia alterations as a result of microvascular problems as well as this current study also found to be a similar finding of both speech frequency (500Hz, 1kHz & 2kHz), high-frequency hearing loss (4kHz & 8 kHz) and extended high-frequency hearing loss ((9kHz & 16 kHz)) among uncontrolled DM.
A quadratic relationship between HbA1c and the occurrence of high-frequency hearing impairment in this investigation. HbA1c levels, in particular, have been linked to high-frequency hearing damage. A relationship between HbA1c and high-frequency hearing impairment. Findings suggest that maintaining proper glycemic management might help to avoid diabetic hearing loss.
According to Sharma, R et al. (2022)15, there is a substantial link between type 2 diabetes and hearing loss. Hearing loss was found to be sensorineural, bilateral, mild to severe, and involving high-frequency and extended high-frequency thresholds in diabetics. The prevalence of SNHL and HbA1c were shown to have been significant relationship among uncontrolled DM.
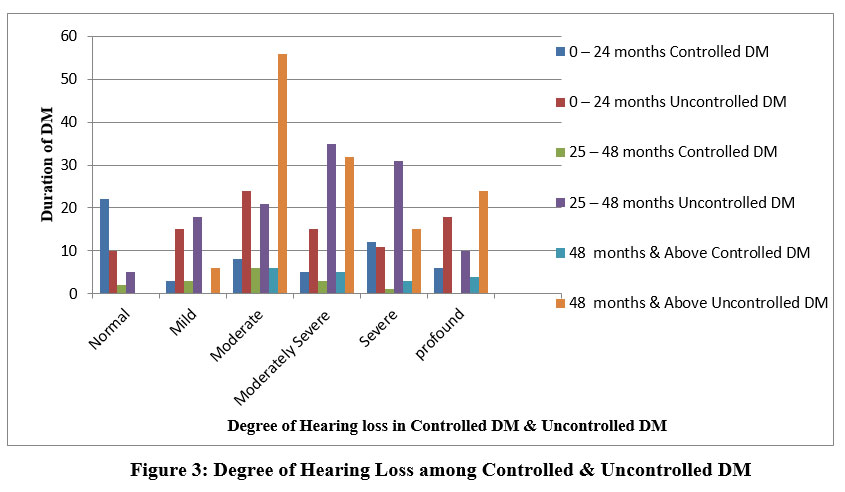 |
Figure 3: Degree of Hearing Loss among Controlled and Uncontrolled DM |
Figure 3 indicates that the degree of hearing loss is more in uncontrolled DM when compared to controlled DM. Moreover, if the diabetic duration is longer in diabetic patients, hearing loss is observed more in severity in both groups.
Conclusion
Diabetic Mellitus is a common metabolic disorder that affects several organs. The purpose of this study was to determine the level of hearing sensitivity in people with controlled and uncontrolled diabetes mellitus. The occurrence of bilateral mild to moderately severe high-frequency hearing loss was discovered to be an alarming indicator of the early start of hearing loss at the speech frequency spectrum in uncontrolled DM. As well, high-frequency and extended high-frequency audiometry (HFA) is an important diagnostic method for the early detection of hearing loss in patients with DM, according to the findings of this study. As a result, we urge the use of HFA as a standard Audiological test battery in patients with DM to track hearing sensitivity levels and progression.
Limitations of this study
Broader research that included people of all ages might result in a larger sample size and more data. However, because the sample size and age range were larger, we didn’t focus on the study’s age constraints. A higher sample size may not make a substantial difference in the conclusion. It may even make it more difficult to reach meaningful findings. A whole separate issue has to be addressed. Following the participants as a cohort for another five or 10 years can provide conclusive and uncontroversial findings. That is what the current investigators want to do at the next level of this study.
Conflict of Interest
The investigators do not have any conflicts of interest.
Funding Sources
There was no other source of funding for this research.
References
- Lin FR, Metter EJ, O’Brien RJ, Resnick SM, Zonderman AB, Ferrucci L: Hearing loss and incident dementia. Arch Neurol. 2011, 68:214-220. 10.1001/archneurol.2010.362
CrossRef - Wilson BS, Tucci DL, Merson MH, O’Donoghue GM: Global hearing health care: new findings and perspectives. Lancet. 2017, 390:2503-2515. 10.1016/S0140-6736(17)31073-5
CrossRef - Deafness and Hearing Loss. (2020). Accessed: January 11, 2020: http://www.who.int/newsroom/ fact-sheets/detail/deafness-and-hearing-loss.
- The IDF Diabetes Atlas, 9th edition. (2019). Accessed: August 9, 2020: http://www.diabetesatlas.org/en/.
- Horikawa C, Kodama S, Tanaka S, et al. Diabetes and risk of hearing impairment in adults: a meta-analysis. J Clin Endocrinol Metab 2013;98:51–8.
CrossRef - Michikawa T, Mizutari K, Saito H, et al. Glycosylated hemoglobin level is associated with hearing impairment in older Japanese: the Kurabuchi Study. J Am Geriatr Soc 2014;62:1231–7.
CrossRef - Kang SH, Jung DJ, Cho KH, et al. Association Between HbA1c Level and Hearing Impairment in a Nondiabetic Adult Population. Metab Syndr Relat Disord 2016;14:129–34.
CrossRef - Kim MB, Zhang Y, Chang Y, et al. Diabetes mellitus and the incidence of hearing loss: a cohort study. Int J Epidemiol 2017;46:717–26.
CrossRef - Schnell O, Crocker JB, Weng J: Impact of HbA1c testing at the point of care on diabetes management. J Diabetes Sci Technol. 2017, 11:611-617. 10.1177/1932296816678263
CrossRef - Sen S, Chakraborty R: Treatment and diagnosis of diabetes mellitus and its complication:
- Ooley C, Jun W, Le K, et al.: Correlational study of diabetic retinopathy and hearing loss. Optom Vis Sci. 2017, 94:339-344. 10.1097/OPX.0000000000001025
CrossRef - Nemati S, Hassanzadeh R, Mehrdad M, Sajedi Kia S: Hearing status in patients with type 2 diabetes mellitus according to blood-sugar control: a comparative study. Iran J Otorhinolaryngol. 2018, 30:209-218.
- Cohen Atsmoni S, Brener A, Roth Y: Diabetes in the practice of otolaryngology. Diabetes Metab Syndr. 2019, 13:1141-1150. 10.1016/j.dsx.2019.01.006
CrossRef - Nagahama S, Kashino I, Hu H, et al.: Haemoglobin A1c and hearing impairment: a longitudinal analysis using a large occupational health check-up data of Japan. BMJ Open. 2018, 8:e023220. 10.1136/bmjopen-2018-023220
CrossRef - Sharma, R., Choudhary, R., & Teharia, R. K. (2022). Correlation between sensorineural hearing loss and HbA1c in diabetes mellitus patients. European Journal of Molecular and Clinical Medicine, 9(1), 958-964.
- Uju IM, Afolabi S. (2021) Type 2 diabetes mellitus and hearing impairment as seen in a tertiary hospital in Port Harcourt. Int J Otorhinolaryngol Head Neck Surg. 2021 Apr;7(4):585-591 http://www.ijorl.com.
CrossRef - Kurein M, et al.Hearing threshold in patients with diabetes mellitus. Jlaryngol. Otol. 1989 Feb;103(2):164-8.
CrossRef - Tay H L, Ray N, Ohri R, Frootko N J. Diabetes mellitus and hearing loss. Clinical Otolaryngology & Allied Sciences. 1995;20(2):130-134.
CrossRef - Panchu P. Auditory acuity in type 2 diabetes mellitus. Int J Diabetes Dev Ctries. 2018;28:114-20.
CrossRef - Ren H, Wang Z, Mao Z, Zhang P, Wang C, Liu A, Yuan G: Hearing loss in type 2 diabetes in association with diabetic neuropathy. Arch Med Res. 2017, 48:631-637. 10.1016/j.arcmed.2018.02.001.
CrossRef - Gupta, S., Eavey, R. D., Wang, M., Curhan, S. G., & Curhan, G. C. (2019). Type 2 diabetes and the risk of incident hearing loss. Diabetologia, 62(2), 281-285.
CrossRef

