
Rohith R Nair1, Sonali Nandish2, Prathibha R. J3, Nandini N. M.4
1J.S.S. Medical College, Mysore, Karnataka, India 570015
2Department of Computer Science and Engineering, JSS Science and Technology University, Mysore, Karnataka, India 570006.
3Department of Information Science and Engineering, JSS Science and Technology University, Mysore, Karnataka, India 570006.
4Department of Pathology, JSS Medical College and Hospital, Constituent of JSSAHER, Mysore, Karnataka, India 570004.
Corresponding Author E-mail: nandinimanoli65@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2535
Abstract
The purpose of this study was to assess the utility of fine needle aspiration cytology (FNAC), immunocytochemistry(ICC) using estrogen receptor(ER) in diagnosing breast lesions. This was done by comparing it to histopathology with immunohistochemistry(IHC), which serves as the gold standard for diagnosing these lesions. To compare these modalities of investigation,50 samples were collected using FNAC and were compared to the same samples obtained by histopathology. For FNAC the results were as follows, Sensitivity=100%, Specificity=100%,Diagnostic Accuracy=100% Positive Predictive Value(PPV)=100% and Negative Predictive Value(NPV)=100% . For ICC using ER the results were as follows, Sensitivity=100%,Accuracy=100%,Positive Predictive Value=100%,Negative Predictive Value=100%. This indicates that FNAC and ICC using ER can be used as a reliable alternative to gold-standard diagnostic tests when the latter cannot be done due to a lack of resources or in circumstances where there is a need to perform a painless, minimally invasive procedure such as in inoperable breast carcinoma. This study also involved using text data analysis on FNAC reports. On analysis, it was found that the useful words were 11.35% of the data set, implying that the process of normalization, will result in the formation of condensed data, which can then be utilized for assisting clinical chart reviews and clinical decision support systems.
Keywords
Breast Cancer; ER; FNAC; Histopathology; ICC; Immunohistochemistry; Machine Learning(ML); Natural Language Processing(NLP); Text Data Analysis
Download this article as:| Copy the following to cite this article: Nair R. R, Nandish S, Prathibha R. J, Nandini N. M. Cytological Diagnostic and Prognostic Methods using Immunocytochemistry (Estrogen Receptor) for Surgical Management of Breast Cancer. Biomed Pharmacol J 2022;15(4). |
| Copy the following to cite this URL: Nair R. R, Nandish S, Prathibha R. J, Nandini N. M. Cytological Diagnostic and Prognostic Methods using Immunocytochemistry (Estrogen Receptor) for Surgical Management of Breast Cancer. Biomed Pharmacol J 2022;15(4). Available from: https://bit.ly/3TlFSIa |
Introduction
Breast Cancer is the most common cancer among Indian females with a mortality of 12.7 per 100,000 women1.
Fine needle aspiration cytology (FNAC) of breast lumps is an important component of the triple assessment of palpable breast lumps2. The advantages of utilizing cytological examination over traditional tissue samples are that it is a safe, simple, quick, and cost-effective diagnostic modality3. However, not all the diagnostic criteria are present every time and in such circumstances, a second diagnostic approach is needed4.
As early diagnosis is of great significance for the patient, any new diagnostic modality in addition to FNAC will enhance its accuracy. In view of this immunocytochemistry (ICC) can complement routine investigations4.
ICC is of great utility in such circumstances as its practical utilization includes characterization of poorly differentiated neoplasms, differentiation of primary from metastatic tumors, determination of sites of origin of metastatic lesions, and prognostic assessment5. An immunocytochemical assay (ICA) on estrogen receptor (ER) improves the accuracy of diagnosis and gives an admirable prognostic indication6. Usually, malignancy on FNAC is diagnosed by Papanicolaou-stained(Pap) smears, following which ICC using ER is done for confirmation and subsequent treatment. So, the immunocytochemical results are obtained in the later stages of patient management. However, they have a great clinical scope if reported within a short time7.
If ICC is used as an adjunct to FNAC, then appropriate information can be provided about the prognosis of breast cancer, helping the clinicians in selecting the right protocol for treatment, avoiding immediate surgical intervention, and essentially saving time and additional expenses8.
This study was done by collecting FNAC samples and subjecting some of these samples to immunocytochemistry using ER. Once this was done, we obtained the histopathology and immunohistochemistry(IHC) reports of the same samples. We then compared FNAC with histopathology and ICC with IHC to determine the diagnostic indices. Using the results of this comparison, we found that ICC on FNAC can be used as an alternative to IHC, to give reliable diagnostic information regarding breast lesions.
The most widely available form of medical data is in the form of text or literature. There is a need to process the medical literature that has been growing rapidly to locate and extract clinically useful information. To achieve this, Natural Language Processing(NLP)and Machine Learning(ML)approaches can be used. One such huge potential for the application of NLP and ML can be seen in the interpretation of breast cancer Electronic Health Records containing text data.
We can use the information obtained by this analysis for assisting clinical chart reviews, the application of which is currently limited by the lack of information in the form of records9.
Materials and Methods
Study Design: Observational Study
Sampling Technique: Convenient Sampling
Materials
FNAC
Disposable Syringe
Needles
Coplin Jar
Slides 75x25mm,1.45mm thick
Fixatives:95% Ethanol
Sterile Containers
Pencil for Marking
ICC
Tris Buffer Powder(QualigensTM ,India), Sodium Chloride, EDTA, Hydrogen Peroxide
Cooker for Antigen Retrieval
ER stain and Secondary Antibodies provided by PathnSitu(India)
Methodology
All the subjects, who were available and satisfied the inclusion and exclusion criteria, during the given period were selected for the study and subjected to further analysis.
| Inclusion Criteria | Exclusion Criteria |
| Patients in the age group 15-75
Patient with breast lumps |
Inadequate sample
Hemorrhagic samples |
The patients were advised for FNAC, and material obtained by this method in the needle hub was pushed onto 6-7 clean slides, which were marked by a diamond pencil. One slide was checked by Toluidine Blue for adequacy. Four out of the Six slides were put in fixative(95% alcohol) for Haematoxylin and Eosin(H&E) and Papanicolaou(Pap) staining. One slide was used for May Grunwald Giemsa stain(MGG).
The extra slide used was the electronically charged slide to perform immunocytochemistry(ICC) for estrogen marker(ER).FNAC smears were prepared on the charged slides directly. The smears thus obtained were fixed in 80% alcohol immediately. The smear was then washed and processed with the antigen retrieval technique. The slides were observed, diagnosed and a standard report according to the format was given.
This was then compared to the histopathology(HPE) processing from the biopsy of breast lumps, following which Sensitivity, Specificity, Accuracy, Positive Predictive Value, and Negative Predictive Value were determined.
Finally, the analysis was completed by using text data analysis.
Statistical Analysis
The demographic characteristic i.e., Age was represented by Arithmetic Mean and Standard Deviation.
The results of FNAC have been compared with histopathology obtained and that of ICC has been compared with IHC, using Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value, and Accuracy, along with the corresponding 95% Confidence Intervals.
FNAC compared to histopathology
| True Positive = FNAC diagnosis and histopathology of the lesion were suggestive of malignancy(a) | False Positive = FNAC diagnosis was suggestive of malignancy but on subsequent histopathology, the lesion was found to be benign(b) |
| False Negative =FNAC diagnosis was suggestive of a benign breast disease but on histopathology, the lesions were found to be malignant(c) | True Negative =both FNAC and histopathology of the lesion were suggestive of benign breast disease(d) |
Similarly, ICC was compared to IHC
| True Positive =ICC and IHC, both showed ER positive results
(a) |
False Positive =ICC suggestive of ER-positive but IHC suggestive of ER-negative
(b) |
| False Negative =IHC suggestive of ER-positive, ICC suggestive of ER-negative
(c) |
True Negative=ICC and IHC both showed ER-negative results
(d) |
Results and Discussion
The patient population consisted of all female patients in the age range of 18-74 years with a mean age of 46.3±13.782 years.
A total of 50 cases of FNAC breast were obtained during the given period of study.
Using FNAC, we were able to make correct diagnoses in all 50 cases. Out of those 28 were diagnosed as Malignant and 22 were diagnosed as benign. which were subsequently confirmed using the histopathological examination. In the data we collected, there was no case of malignancy that was diagnosed as benign by FNAC.
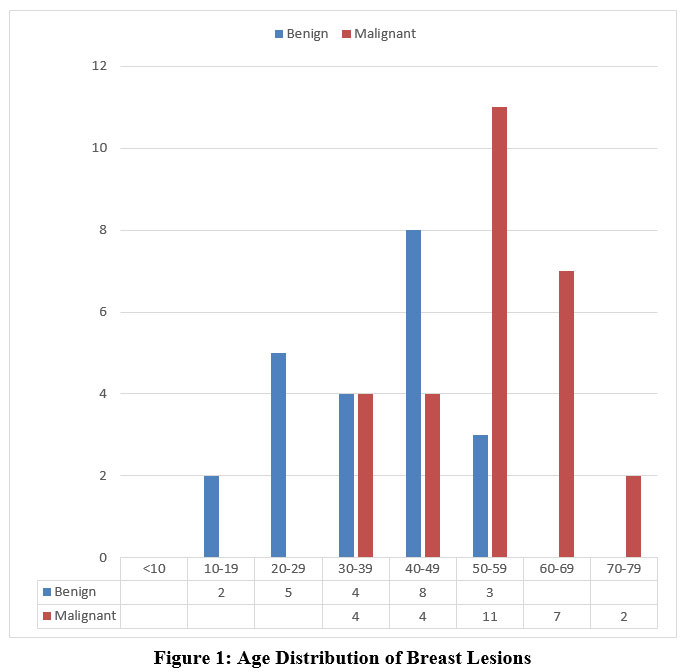 |
Figure 1: Age Distribution of Breast Lesions |
It was observed that benign breast lesions were most common in the 4th decade of life and the most common lesion was fibroadenoma. It was also observed that malignant lesions were more common in the 5th and 6th decades of life, wherein invasive ductal carcinoma was the most common lesion.
Table 1: Table of Comparison of fine needle aspiration cytology(FNAC) with histopathological examination(HPE).
| Histopathology
|
||||
| Positive | Negative | TOTAL | ||
| FNAC | Positive | 28(a) | 0(b) | 28 |
| Negative | 0(c) | 22(d) | 22 | |
| TOTAL | 28 | 22 | 50 |
Using the above data, we determined the Sensitivity, Specificity, Accuracy, Positive Predictive Value, and Negative Predictive value of FNAC as a diagnostic test for screening patients with breast lesions.
Sensitivity=100% (95% Confidence Interval=87.66% to 100%)
Specificity=100% (95% Confidence Interval= 56% to 100%)
Diagnostic Accuracy=100% (95% Confidence Interval= 89% to 100%)
Positive Predictive Value=100%
Negative Predictive Value=100%
Out of the 50 samples collected, ICC was performed on 25 samples. Out of these,16 cases were found to be malignant and 9 were benign. The cases which were diagnosed as malignant also underwent IHC and only those samples which had a gold standard (IHC) to be compared to, have been included in analyzing the results
Table 2: Comparison of immunocytochemistry(ICC) with immunohistochemistry(IHC)
| IHC | ||||
| Positive | Negative | TOTAL | ||
| Positive | 14(a) | 0(b) | 14 | |
| ICC | Negative | 0(c) | 2(d) | 2 |
| TOTAL | 14 | 2 | 16 |
We calculated the Sensitivity, Specificity, Accuracy, Positive Predictive Value, and Negative Predictive Value of ICC using ER as an adjunct to FNAC for diagnosing breast lesions.
Sensitivity=100% (95% Confidence interval= 84% to 100%)
Specificity=100%( 95% Confidence Interval= 81% to 100%)
Accuracy=100%( 95% Confidence Interval= 41% to 100%)
Positive Predictive Value(PPV)=100%
Negative Predictive Value(NPV) =100%
 |
Figure 2: FNAC: Fibroadenoma of the breast with Haematoxylin and Eosin(H&E) staining |
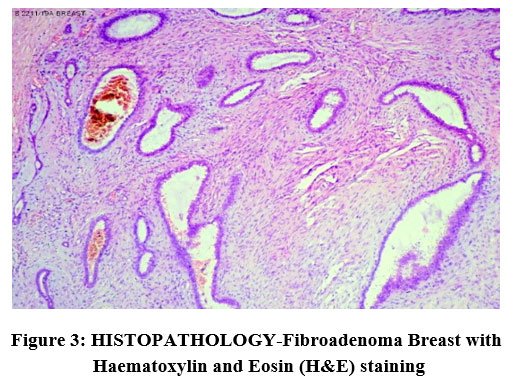 |
Figure 3: HISTOPATHOLOGY-Fibroadenoma Breast with Haematoxylin and Eosin (H&E) staining |
 |
Figure 4:Fibroadenoma of Breast, Immunocytochemistry-Negative Nuclear staining for Estrogen Receptor(ER) |
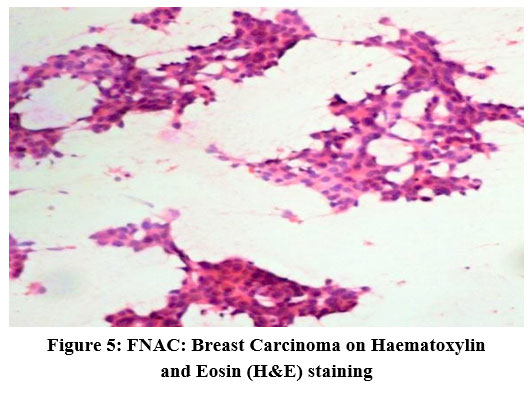 |
Figure 5:FNAC: Breast Carcinoma on Haematoxylin and Eosin (H&E) staining |
 |
Figure 6: Breast Carcinoma: Immunocytochemistry-Positive Nuclear Staining for Estrogen Receptor(ER) |
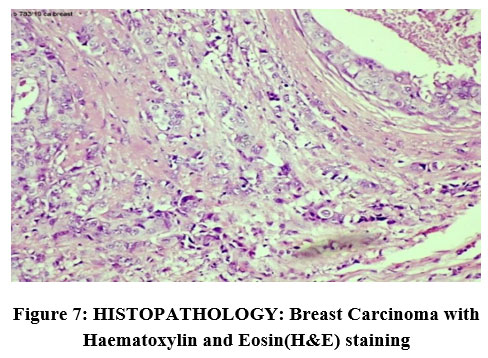 |
Figure 7: HISTOPATHOLOGY: Breast Carcinoma with Haematoxylin and Eosin(H&E) staining |
 |
Figure 8: Breast Carcinoma: Immunohistochemistry-Positive Nuclear Staining for Estrogen Receptor(ER) |
Text Data Analysis
Dataset: Out of the samples obtained,50 Text Reports of Breast Cancer patients have been considered in the study. The data has been analyzed with NLP approaches like Section segmentation, Sentence segmentation, and feature extraction approaches to fetch only the required characteristic features. The extraction of features has resulted in the removal of all types of noise and additional data.
Example: Sample Electronic Health Record(EHR) on Breast Cancer
Table 3: Sample EHR with free-text Results or Patient report
| SL No | Patient Name | Mobile | Department Unit | Address | Age | Gender | Description | Result/Patient Report |
| 1 | XYZ | 99999999 | Unit I | XYZ Town | 59 | F | FNAC ( CYTOLOGY) | The smear is highly cellular and shows malignant cells prominent pleomorphism, and eosinophilic cytoplasm. The smear has a pleomorphic nucleus with a high nucleo-cytoplasmic ratio, vesicular chromatin, and prominent nucleoli. |
The Result Section of the EHR was processed using the NLP approach and converted into a structured tabular form with the only required information as shown In Table 4 below.
Table 4: Result or Patient Report Section of Sample EHR converted to a structured form.
| Cellularity | Pleomorphism | Myoepithelial | N-C ratio | Nucleus | Nucleoli |
| High | Prominent | – | High | Pleomorphic | Prominent |
The reduction in the number of words is as shown in Figure 9 below
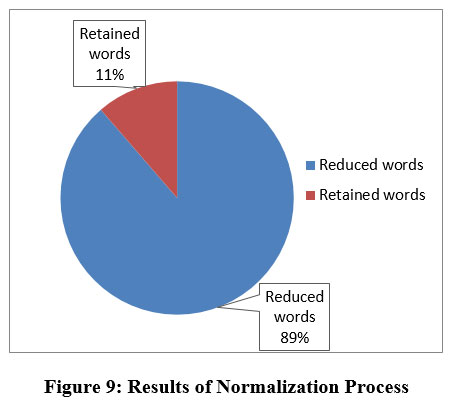 |
Figure 9: Results of Normalization Process |
Discussion
From our study, we found that the age distribution of breast lesions was such that benign breast disease was most common in the 4th decade of life and malignant lesions were most common in the 5th and 6th decades of life, this is in agreement with other studies in which the same trends can be observed10,11.
In our study 100% cytohistological correlation was seen in both benign and malignant cases, the Sensitivity of FNAC is 100%, the Specificity is 100%, the Accuracy is 100%, the Positive Predictive Value(PPV) is 100%, and the Negative Predictive Value(NPV)=100%.
The sensitivity and specificity of our study are found to be greater than the results seen in the meta-analyses by Wang et al.,12 This could be because, the sample size of our study is limited to 50, whereas the study performed by Wang et al., being a meta-analysis can be generalized to the population at large. The Accuracy of our study is in agreement with the literature available wherein Accuracy rates of 84%-99.5% have been reported13,14.
The study by Panjvani et al., has resulted in a value of 100% for Positive Predictive Value(PPV) and 97.85% for Negative Predictive Value(NPV), the study by Mišković et al., suggests a PPV of 95.5%, and NPV of 94.2%, and the study done by de Cursi et al., has resulted in a PPV of 99.6% and NPV of 97.6%, all of which are close to the values found in our study13-16. While histopathology is considered a gold standard, the presence of FNAC as an alternative for obtaining results of breast lesions, serves as a boon in resource-deficient areas because of its cost-effectiveness, rapid turnaround time, and repeatability17,18.
Our study also found that the use of ICC on FNAC sample has Sensitivity=100% ,Specificity=100%,Accuracy=100%,Positive Predictive Value(PPV)=100%,Negative Predictive Value(NPV) =100%.
These results of Specificity and PPV are in agreement with the literature, however, the Sensitivity and NPV obtained in our study are greater than what is reported by Geethamala et al., wherein Sensitivity of 96.3% and NPV of 95.7% have been reported4.
This diagnostic modality can be preferred over histopathology in cases of advanced inoperable tumors, ICC using ER can serve as a reliable test to assess the ER status of such a breast lesion following which the decision of selecting hormone therapy can be done. In a patient with advanced breast cancer, by avoiding histopathology we spare the patient the additional distress of an invasive procedure and instead get the necessary results by using a relatively painless, minimally invasive test like FNAC on which ICC can be performed directly. This is also in accordance with the guiding principle of improving the quality of life in patients with advanced breast carcinoma19.
When we performed ICC using ER, we found that better staining of the samples and hence better results were obtained when the FNAC sample was placed on the slide in the form of a button as opposed to a smear, before staining with ER (Figure 6). The sample also gave good results when there was little to no blood in it, so it is of great importance to obtain a bloodless sample for the same. It is also to be noted that a clinical correlation of the obtained FNAC sample will be helpful because non-neoplastic lesions such as lipoma, and mastitis need not undergo additional ICC using ER. As for the malignant cases, the results of ICC using ER were either reported as ‘POSITIVE’ or ‘NEGATIVE’. However, in the gold standard method of IHC using ER, the Allred Score is used to give a detailed assessment of the Hormone Receptor Status, which cannot be done using ICC.
Text Data Analysis: In the proposed work, medical text data used for the description of breast cancer were pre-processed to remove all types of noise and outliers. Normalization is a process by which the randomness and redundancy of text are reduced.
Conclusion
Fine needle aspiration cytology(FNAC) is a quick, cost-effective, minimally invasive, and accurate diagnostic method for the assessment of breast lumps, which can be done on an outpatient basis. FNAC provides good sensitivity, specificity, and positive and negative predictive values that are comparable to the gold standard, histopathology, especially in the hands of an experienced cytopathologist.
immunocytochemistry (ICC) using ER done on FNAC samples is of high diagnostic accuracy as well and can be used as an adjunct to assess the estrogen receptor(ER) status, which is of vital prognostic significance, without the invasiveness of a surgical biopsy.
Therefore, in resource-limited regions and with the aid of triple assessment, ICC on FNAC samples can be used instead of immunohistochemistry(IHC), especially in case of advanced inoperable carcinomas. Further studies on larger samples are needed to substantiate our findings.
Text Data Analysis: The normalization process reduces the number of words in reports of FNAC diagnoses. This condensed data can serve as an important component in the development of a large-scale clinical decision support system.
Acknowledgment
I would like to express my gratitude to Dr. Nandini N.M., Professor Department of Pathology, JSS Medical College and Hospital for guiding me throughout the project. I would like to thank Sonali Nandish, Department of Computer Science and Engineering, JSS Science and Technology University, Mysore and Prathibha R.J Department of Information Science and Technology, JSS Science and Technology University, Mysore for their assistance in Text Data Analysis.
I would like to thank Dr. Vijaya B., Head of the Department, Pathology JSS Medical College and Hospital for allowing me to collect the data and perform the research in their department.
A special thanks to the technicians of the department of pathology, Mr. Vasanth Kumar K.S., Mr. A.N. Channegowda, Mrs. Ritamurphy, Mrs. Sulochana M.S., Mrs. Babitha M.S , Ms. Anjali K.S. for their support without which I wouldn’t have been able to complete the research.
Conflict of Interest
None
Funding Source
Indian Council Of Medical Research(ICMR).
References
- Malvia S, Bagadi SA, Dubey US, Saxena S. Epidemiology of Breast Cancer in Indian women. Asia-Pacific Journal of Clinical Oncology. 2017;13(4):289–95.
CrossRef - Mane PS, Kulkarni AM, Ramteke RV. Role of fine needle aspiration cytology in diagnosis of breast lumps. Int J Res Med Sci. 2017 Jul 26;5(8):3506.
CrossRef - Al-Abbadi MA. Basics of cytology. Avicenna J Med. 2011;1(1):18–28.
CrossRef - Geethamala K, Murthy VS, Vani BR, Rao MS, Thejaswini MU, Padmaja KP. Comparison of Immunocytochemistry and Immunohistochemistry on Breast Carcinoma: A Boon or a Bane? J Lab Physicians. 2017;9(1):5–10.
CrossRef - Ronald A. DeLellis, Rana S. Hoda. Immunochemistry and Molecular Biology in Cytological Diagnosis Koss’ Diagnostic Cytology and Its Histopathologic Bases, Fifth Edition .Philadelphia : Lippincott Williams & Wilkins, :2006,1635–80.
- Reiner A, Neumeister B, Spona J, Reiner G, Schemper M, Jakesz R. Immunocytochemical Localization of Estrogen and Progesterone Receptor and Prognosis in Human Primary Breast Cancer. Cancer Res. 1990 Nov 1;50(21):7057–61.
- Dalquen P, Sauter G, Epper R, Kleiber B, Feichter G, Gudat F. Immunocytochemistry in Diagnostic Cytology. In: Pfitzer P, Grundmann E, editors. Current Status of Diagnostic Cytology. Berlin, Heidelberg: Springer; 1993. p. 47–80. (Recent Results in Cancer Research).
CrossRef - Mandal PK, Mondal SK, Roy S, Adhikari A, Basu N, Sinha SK. Immunocytochemistry: It’s role in diagnosis of undifferentiated neoplasms by fine needle aspiration cytology. J Cytol. 2013;30(2):121–4.
CrossRef - Sarkar S, Seshadri D. Conducting Record Review Studies in Clinical Practice. J Clin Diagn Res. 2014 Sep;8(9):JG01–4.
CrossRef - Sharma P, Choudhary M, Gupta S, Bharadwaj S. Fine Needle Aspiration Cytology in Palpable Breast Lumps: A Retrospective Study. SJPM. 2020 Feb 29;05(02):134–6.
CrossRef - Sandhu DS, Sandhu S, Karwasra RK, Marwah S. Profile of breast cancer patients at a tertiary care hospital in north India. Indian Journal of Cancer. 2010 Jan 1;47(1):16.
CrossRef - Wang M, He X, Chang Y, Sun G, Thabane L. A sensitivity and specificity comparison of fine needle aspiration cytology and core needle biopsy in evaluation of suspicious breast lesions: A systematic review and meta-analysis. The Breast. 2017 Feb 1;31:157–66.
CrossRef - Panjvani SI, Parikh BJ, Parikh SB, Chaudhari BR, Patel KK, Gupta GS, et al. Utility of Fine Needle Aspiration Cytology in the Evaluation of Breast Lesions. J Clin Diagn Res. 2013 Dec;7(12):2777–9.
CrossRef - Wilkinson EJ, Schuettke CM, Ferrier CM, Franzini DA, Bland KI. Fine needle aspiration of breast masses. An analysis of 276 aspirates. Acta Cytol. 1989 Oct;33(5):613–9.
- De Cursi JAT, Marques MEA, De Assis Cunha Castro CAC, Schmitt FC, Soares CT. Fine-Needle Aspiration Cytology (FNAC) is a reliable diagnostic tool for small breast lesions (≤ 1.0 cm): a 20-year retrospective study. Surgical and Experimental Pathology. 2020 Dec 7;3(1):29.
CrossRef - Mišković J, Zorić A, Radić Mišković H, Šoljić V. Diagnostic Value of Fine Needle Aspiration Cytology for Breast Tumors. Acta Clin Croat. 2016 Dec;55(4):625–8.
CrossRef - Ibikunle DE, Omotayo JA, Ariyibi OO. Fine needle aspiration cytology of breast lumps with histopathologic correlation in Owo, Ondo State, Nigeria: a five-year review. Ghana Med J. 2017 Mar;51(1):1–5.
CrossRef - Mitra S, Dey P. Fine-needle aspiration and core biopsy in the diagnosis of breast lesions: A comparison and review of the literature. Cytojournal. 2016 Aug 31;13:18.
CrossRef - Zhang B, Nilsson ME, Prigerson HG. Factors Important to Patients’ Quality of Life at the End of Life. Archives of Internal Medicine. 2012 Aug 13;172(15):1133–42.
CrossRef

