
Pompini Agustina Sitompul , Nina Mariana*, Ervan Budiman , Dian Wahyu Tanjung, Betha Ariesanty, Teguh Sarry Hartono, Jahiroh, Christine Ernita, Aninda Dinar, Anita Puspitasari, Herlina, Suliati, Farida Murtiani, Siti Maemun, Mohammad Syahriland Wahyu Budi Santosa
, Nina Mariana*, Ervan Budiman , Dian Wahyu Tanjung, Betha Ariesanty, Teguh Sarry Hartono, Jahiroh, Christine Ernita, Aninda Dinar, Anita Puspitasari, Herlina, Suliati, Farida Murtiani, Siti Maemun, Mohammad Syahriland Wahyu Budi Santosa
Sulianti Saroso Infectious Disease, Jakarta, Indonesia
Corresponding Author E-mail: mynayla09@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/2513
Abstract
Hospital workers were at high risk for SARS-CoV-2 infection and the first population with authorized access to the three doses of vaccination against SARS-CoV-2 antigen. The study was aimed to compare SARS-CoV-2 antibody levels among hospital workers receiving the three doses of Covid-19 vaccines with a history of Covid-19 infection versus those without a history of infection. A cross sectional study was conducted at the Sulianti Saroso Infectious Disease Hospital (SSIDH) in December 2021. The inclusion criteria were hospital workers in both subjects with and without previous Covid-19 infection and those who had received 3 doses of Covid-19 vaccines. Anti SARS-CoV-2 antibody levels measured by the Architect of SARS-CoV-2 IgG II Quant. There were 75 participants in the study, the median of anti SARS CoV-2 levels reported 8724.4 AU/mL (3396.8, 15773.2 AU/mL, Interquartile range). They were divided into 2 groups according to the status of prior Covid-19 infection, hospital workers with and without previous of Covid-19 infection. There was no significance difference in antibody less than 25.000 AU/mL between hospital worker with and without previous Covid-19 infection (p=1,000). Meanwhile, the median of antibody levels was seen in the interval between the 3rd dose of vaccine within 1 month; 2 to 3 months; 4 to 5 months before the antibody measurement (14576.5 AU/mL;12407.4 AU/mL; 5778.1 AU/mL, respectively). In this study, after three doses of Covid-19 vaccines, there was no significance difference in antibody levels of hospital worker with and without previous Covid-19 infection.
Keywords
Abbott Architect; Antigen; SARS-CoV-2; Vaccination
Download this article as:| Copy the following to cite this article: Sitompul P. A, Mariana N, Budiman E, Tanjung D. Y, Ariesanty B, Hartono T. S, Jahiroh J, Ernita C, Dinar A, Puspitasari A, Herlina H, Suliati S, Murtiani F, Maemun S, Syahril M. Quantitative Antibody Levels in Hospital Workers After Receiving Three Doses of Covid-19 Vaccines. Biomed Pharmacol J 2022;15(3). |
| Copy the following to cite this URL: Sitompul P. A, Mariana N, Budiman E, Tanjung D. Y, Ariesanty B, Hartono T. S, Jahiroh J, Ernita C, Dinar A, Puspitasari A, Herlina H, Suliati S, Murtiani F, Maemun S, Syahril M. Quantitative Antibody Levels in Hospital Workers After Receiving Three Doses of Covid-19 Vaccines. Biomed Pharmacol J 2022;15(3). Available from: https://bit.ly/3BouXa3 |
Introduction
The global pandemic was caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 We really need to control the spread of the outbreak and a global COVID-19 vaccination.1 Five vaccines (BioFarma, Pfizer, AstraZeneca, Moderna, Zifivax) had received the Indonesian Food and Drug Supervisory Agency (BPOM) emergency use authorization. In previous study, it was found that 2 doses vaccines could have only covered immunity needed for six months.1,2,3 Hence, many scientists concluded booster vaccine should be given to vulnerable group such as health worker as front liners in the pandemic era.1
Several Covid-19 vaccines have been developed that offer protection against infection by generating an immune response to the spike antigen of SARS-CoV-2.4 Previous study suggest that people who had history of COVID-19 are more vulnerable to get infected with Omicron variant. Thus, research on antibody responses to SARS-CoV-2 should be a priority in terms of prophylaxis and treatment.4,5 This study investigated the quantitative antibody against SARS-CoV-2 blood samples collected from Sulianti Saroso hospital worker who were infected with SARS-Cov-2 and who had received 3 doses of vaccine.
Methods
A cross sectional study was conducted in December 2021. We recruited a total 75 of Sulianti Saroso hospital workers in Jakarta, both participants with and without previous Covid-19 infection and who had received 3 doses of vaccine. The 3 types of doses were 2 doses of inactivated vaccine or viral vector vaccine and followed by 1 dose of mRNA or viral vector vaccine. The type of vaccine was based on covid-19 vaccines available in Indonesia. The interval between the time of previous Covid-19 infection and antibody test was 6 months. We used sampling techniques by non-probability sampling (purposive sampling) and the total population as a sample size.
Anti-SARS-CoV-2 antibody levels measured by the Architect of SARS-CoV-2 IgG II Quant.1,2 Serum from the blood samples was collected at the Sulianti Saroso Hospital laboratory. There was variation of the interval between vaccine dose 3 and antibody test (within 1 month; 2 to 3 months; 4 to 5 months before the antibody measurement). As an upper limit of quantitation of 25.000 AU/ml or 40.000 AU/ml by the manufacturer of some antibody test reports, therefore we decided to classify the level less than 25.000 AU/ml and greater than or equal to 25.000 AU/ml. We used an excel formula to divide the antibody level.
All of 75 participants are divided into 2 groups according to the status of prior Covid-19 infection (hospital workers with and without previous of Covid-19 infection). We used SPSS version 21 for statistical analysis. P value of > 0.50 was considered statistically significant. The Human Research Ethics Committee at Sulianti Saroso Hospital approved this study (approval number 44/XXXVIII.10/XII/2021). All participants provided written informed consent.
Results
Table 1 showed that among the 75 participants, mostly the age was less than 50 years. Aantibody response was mostly less than 25.000 AU/mL (86.7 %). The median of anti SARS CoV-2 levels reported 11815.2 AU/mL (4647.1, 16242.5 AU/mL, IQR). There was no significance difference in antibody levels of hospital worker with and without previous Covid-19 infection (p=1,000).
Table 1: Participants’ characteristics according to the status of prior Covid-19 infection.
| Participants’ characteristics | All participants
(N=75) n (%) |
With a history of Covid-19 infection
(N=41) n (%) |
Without a history of Covid-19 infection
(N=34) n (%) |
| Female | 55 (73.3) | 32 (78.1) | 23 (67.7) |
| Age less than 50 years | 60 (80) | 34 (82.9) | 26 (76.5) |
| Working in inpatient/outpatient care | 45 (60) | 30 (73.2) | 15 (44.1) |
| Comorbidity‖ | 17 (22.7) | 12 (29.3) | 5 (14.7) |
| Interval between the third vaccination and antibody measurement | |||
| 1 month | 14 (18.7) | 12 (29.3) | 2 (5.9) |
| 2 to 3 months | 20 (26.6) | 17 (41.4) | 3 (8.8) |
| 4 to 5 months | 41 (54.7) | 12 (29.3) | 29 (85.3) |
| Type of vaccines | |||
| Sinovac + Sinovac + Pfizer | 6 (8) | 6 (14.6) | 0 |
| Sinovac + Sinovac + Moderna | 68 (90.7) | 35 (83.4) | 33 (97.1) |
| AZ + AZ + AZ | 1 (1.3) | 0 | 1 (2.5) |
Note: AZ: Astra Zeneca
Table 2: Antibody levels according to the status of prior Covid-19 infection.
| Antibody level | All participants
(N=75) |
With a history of Covid-19 infection
(N=41) |
Without a history of Covid-19 infection
(N=34) |
P * |
| Antibody level (AU/mL), median (IQR) | 8724.4
(3396.8, 15773.2) |
11815.2
(4647.1, 16242.5) |
5392.05
(3382, 13356.8) |
0.110 |
| Antibody less than 25000 AU/mL, n (%) | 65 (86.7) | 36 (87.8) | 29 (85.3) | 1.000 |
| *P value from Wilcoxon-Mann-Whitney or Fisher exact test for comparisons between participants with a history of Covid-19 infection and those without a history of infection.
Abbreviation: IQR, interquartile range. |
||||
In this study, 74 (98,7%) of participants had received heterologous vaccines (2 doses of Sinovac plus Pfizer or Moderna) and 1 (1,3%) subject had received the three doses of Astra Zeneca. Figure 1. Showed that median of Sars-Cov-2 antibody levels after the three doses vaccine.
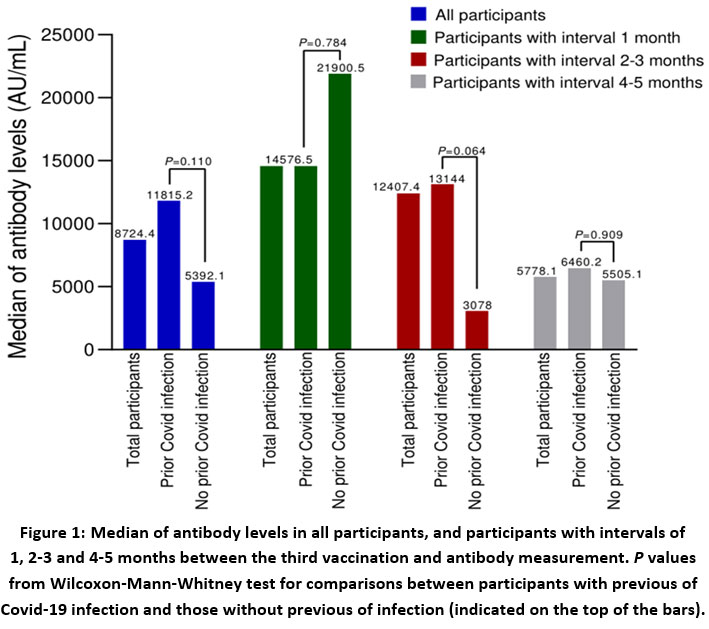 |
Figure 1: Median of antibody levels in all participants, and participants with intervals of 1, 2-3 and 4-5 months between the third vaccination and antibody measurement. |
P values from Wilcoxon-Mann-Whitney test for comparisons between participants with previous of Covid-19 infection and those without previous of infection (indicated on the top of the bars).
Discussion
In this study, 75 hospital workers at Sulianti Saroso hospital who received three doses vaccination was examined. We identified the participant’s characteristic by prior infection status. Participants who were previously infected showed no difference antibody responses after the third vaccination. To ensure the positive threshold for each assay in standardized international units, a dilution series for SARS-CoV-2 antibody was prepared.1 Abbott Architect.,1 recommended assay cut off was 56.2 AU/ml. Two weeks after the first dose and second dose, anti-spike IgG levels increased more than 100-fold and 10-fold, respectively.2 Peak antibody levels were observed 7 weeks after the first dose at 23,881 AU/ml (7,304 to more than 25,000 AU/ml, 10th to 90th percentile).1,2
In July 2021, The Government started to provide the third doses of vaccines for healthcare workers. Other countries such as Israel, the United States, the United Kingdom and Singapore have already provided the third doses of vaccine to the public 6-8 Three studies showed that after at least 12 days after the booster, the group that received the three doses had an 11.3 times lower risk of infection than the group that had not received the three doses of vaccine.6,7,8 In addition, the severity was also 19.5 times lower than the group that had not received the booster vaccine. 6-8
In this study, there was no significance difference in antibody levels of hospital worker with and without previous Covid-19 infection. Romero et al.,3 showed that of 168 health workers received the three doses by Pfizer vaccine. There was no significance difference in IgG-SARS-COV2 levels between the groups who have and who have not previously had COVID-19 within 1-7 days after the booster vaccine (p=0.011) or also after 21-28 days (p=0.011).3
Ali Hamady et al.,9 mentioned that antibody level, IgG and IgM will decrease several months after Covid-19 infection. Overall, IgM and IgG titers peak 2 to 3 weeks after symptom onset and decline to undetectable levels by 6 weeks for IgM, while IgG achieve a plateau before declining within 2 to 3 months.9 Therefore if booster doses of vaccine was gave more than 3 months after infection, it provided the same antibody value as subjects without previous Covid-19 infection. In general, vaccination induce higher antibody titers against SARS-CoV2 than natural infection. However, single-dose vaccination of patients with previous Covid-19 infection induced an increase in titers of anti-spike IgG, rivaling titers generated after three doses in infection-naïve subjects.9 The antibody responses after a single vaccine dose in those previously infected develop more rapidly and reaches greater titers. A phenomenon that occurred when anti spike IgG from previous SARS-CoV2 infection had decreased to low or undetectable levels, indicating immune memory despite reduced antibodies. 9
Our study in line with Gluck et al.,14 who mentioned that among 136 health workers infected during the first wave of Covid-19 and in the subgroup after three doses of vaccine about 1 year late, it induced high antibody levels in individuals with a previous Covid-19. Gluck et al.,14 also mentioned T cell-mediated response measured by ELISpot, detecting mainly T memory cells. However, what is the salient factor in long-term immunity to SARS-CoV-2? it is cellular or antibody-mediated immunity. Meanwhile, whether the differences shown between the various vaccines are of clinical relevance.14 In three doses, vaccinated individuals with previous Covid-19 infection showed significantly greater anti-body levels in mRNA vaccine recipients than in recipients of the vector-based vaccine (non mRNA vaccine). SARS-CoV-2-S-protein-reactive memory T cell counts were also numerically, but not significantly greater after vaccination with the mRNA vaccines than after vaccination with non mRNA vaccine (heterologous vaccine).10 That study was in line with the study of Callaway and Juno et al.10,11
In this study, the median of Sars-Cov-2 antibody levels based on the various interval between the third vaccination and antibody measurement (1 month, 2 to 3 months, 4 to 5 months) decrease gradually. This is in line with the model estimated by Doria-Rose et al.,12 which predicts antibodies from booster vaccines can last for up to 209 days.13 The limitation of our study is that the sample size was small and antibody testing from subjects was not performed on two time before and after third dose vaccine.
Conclusion
In this study, after three doses of Covid-19 vaccines, there was no significance difference in antibody levels of hospital worker with and without previous Covid-19 infection. However, develop a better understanding of characterizing antibody responses and evaluating antibody persistence in SARS-CoV-2 infection by longitudinal studies is needed.
Acknowledgement
We would like to thank the personnel at Sulianti Saroso Infectious Diseases Hospital, especially in Laboratory and Surveillance staff for recruiting the participants and for technical assistance related to this study.
Conflict of Interests
There is no conflict of interest.
Funding Sources
There is no funding sources.
References
- Benjamin TB, Andrew B, Susan LF, Erin AG, Pavitra R, Meei-L et al. Anti-SARS-CoV-2 Antibody Levels Measured by the AdviseDx SARS-CoV-2 Assay Are Concordant with Previously Available Serologic Assays but Are Not Fully Predictive of Sterilizing Immunity. Journal of Clinical Microbiology; 59: e00989-21. doi: 10.1128/JCM.00989-21 (2021)
CrossRef - Narasimhan M, Mahimainathan L, Araj E, Clark AE, Markantonis J, Green A, et al. Clinical Evaluation of the Abbott Alinity SARS-CoV-2 Spike-Specific Quantitative IgG and IgM Assays among Infected, Recovered, and Vaccinated Groups. Journal of Clinical Microbiology; 9: e00388-21. https://doi.org/10(2021)
CrossRef - Elena Romero-Ibarguengoitia M, Rivera-Salinas D, Guadalupe Hernández-Ruíz Y, Gabriela Armendariz-Vázquez A, González-Cantú A, Antonieta Barco-Flores I, et al. Effect of the third dose of BNT162b2 vaccine in quantitative SARS-CoV-2 spike 1-2 IgG antibody titers in healthcare workers. https://doi.org/10.1101/ 2021.10.20.21265269 accessed 20 Feb (2021)
CrossRef - Jia W, Nicole S, Philippa CM, Daniel A, Ruth S, John B et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nature Microbiology;140–1149 (2021)
- WHO. WHO Covid 19 Response. https://healthcluster.who.int/resources/covid-19-response, accessed 20 feb (2022)
- Yun-Kuan Thye A, Teng-Hern Tan L, Woan-Fei Law J, Letchumanan V. COVID-19 Booster Vaccines Administration in Different Countries;http://journals.hh-publisher.com/index.php/pmmb accessed 20 feb (2021)
- Bar-On YM, Goldberg Y, Mandel M, Bodenheimer O, Freedman L, Kalkstein N, et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. New England Journal of Medicine;385(15):1393–400 (2021).
CrossRef - Burckhardt RM, Dennehy JJ, Poon LLM, Saif LJ, Enquist LW. Are COVID-19 Vaccine Boosters Needed? The Science behind Boosters. Journal of Virology (2021)
CrossRef - Hamady A, Lee J, Loboda ZA. Waning antibody responses in COVID-19: what can we learn from the analysis of other coronaviruses? Springer;50:11-25 (2021)
CrossRef - Callaway E. Mixing Covid Vaccines Triggers Potent Immune Response. Nature; 593:491 (2021)
CrossRef - Juno JA, Wheatley AK. Boosting immunity to COVID-19 vaccines. Vol. 27, Nature Medicine. Nature Research;p. 1874–5 (2021)
CrossRef - Doria-Rose N, Suthar MS, Makowski M, O’Connell S, McDermott AB, Flach B, et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. New England Journal of Medicine;384(23):2259–61 (2021)
- Thomas SJ, Moreira ED, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. New England Journal of Medicine;385(19):1761–73 (2021)
CrossRef - Glück V, Grobecker S, Köstler J, Tydykov L, Bertok M, Weidlich T, et al. Immunity after COVID-19 and vaccination: follow-up study over 1 year among medical personnel. Infection 50:439–446 (2022).
CrossRef

