
Manuscript accepted on :16-05-2022
Published online on: 09-06-2022
Plagiarism Check: Yes
Reviewed by: Dr. Nawaj Pathan
Second Review by: Dr. Ankur Singh Bist
Final Approval by: Dr. H Fai Poon
Ivan Rolland Karkada1,2, Urban John Arnold D'souza2,4*, Zainal Arifin bin Mustapha2 and Jaiprakash Mohanraj2,4
1School of Medicine, MAHSA University, Malaysia
2Faculty of Medicine and Health Sciences, Universiti Malaysia Sabah, Malaysia
3Faculty of Medicine, Department of Physiology, Father Muller Medical Collage, India
4School of Medicine, International Medical University, Malaysia
Corresponding Author E-mail: urbandsouza@fathermuller.in
DOI : https://dx.doi.org/10.13005/bpj/2417
Abstract
Background and objective: The importance of exercise and knowledge of emotional intelligence (EI) is gaining pace in academia, which is a positive development. Only a few single-blind research studies on the benefits of exercise and Emotional intelligence have indicated their effects on educational attainment among primary school children, but there are very few reports from young adult students. This longitudinal study aims to develop an intervention protocol to investigate the differential association between induced moderate physical exercise combined with emotional intelligence awareness on academic performance among 18-24-year-old private medical university students. Methods: Students are voluntarily enrolled in two groups: TEST (n = 180) and CONTROL (n = 180) based on inclusion criteria along with applicable consent’s and ethical clearance. The groups' baseline data mapping was completed in three phases. For the TEST group, baseline data was obtained in three stages during Phase-1; -, which is the pre-intervention phase: Anthropometric data, haemoglobin concentration, and cardiorespiratory measurements were all measured in Stage 1. (Lab-based data). Stage 2: two questionnaires were used, one to measure EI awareness and the other to assess learning styles (VARK). Stage 3 entailed the simultaneous recording of pre-intervention academic grades, of a said end block examination for both TEST and CONTROL groups. Phase 2: This is the intervention phase, which included only two components for the TEST group: the first was a moderate exercise regime (BRISK WALKING) of 2-3 sessions per week for about 30 minutes per session, and the second was addressing EI awareness. Which refers to knowing the current status of EI level, and fostering EI knowledge through various teaching-learning methods. Following the end of Phase -1 baseline data mapping, the two intervention components for the TEST group run concurrently for about 6months/24weeks, for the TEST group. Phase-3: is the post-intervention phase which included repeating of Phase-1; Stages 1, 2, and 3 for the TEST group, as well as a concurrent record and analysis of post-intervention academic grades, of the final professional examination for both TEST and CONTROL groups was done after Phase-2. The outcomes of Phase-1 and Phase-3 differential association compared. Results: The Statistical Package for Social Science (SPSS) Version 21.0 software was used to analyse all data from phases 1 and 3. A statistically significant correlation was found between the TEST group (p = 0.0001) and the CONTROL group (p = 0.406) when the pre-intervention period of multifactorial components subjected to intervention was compared to the post-intervention period. Conclusion: Intervention protocol with combined effect of emotional intelligence awareness and induced moderate physical exercise (BRISK WALKING) has shown significant improvement in academic grades.
Keywords
Academics; Emotional Intelligence; Fitness; Health
Download this article as:| Copy the following to cite this article: Karkada I. R, D'souza U. J. A, Mustapha Z. A. B, Mohanraj J. Academic Performance Improves with Emotional Intelligence Awareness and Physical Exercise among Medical Students. Biomed Pharmacol J 2022;15(2). |
| Copy the following to cite this URL: Karkada I. R, D'souza U. J. A, Mustapha Z. A. B, Mohanraj J. Academic Performance Improves with Emotional Intelligence Awareness and Physical Exercise among Medical Students. Biomed Pharmacol J 2022;15(2). Available from: https://bit.ly/3xjGJz7 |
Introduction
In today’s academically demanding world, many multifactorial components such as nutritional status (example: iron concentration in the blood), cardiorespiratory fitness, muscular exercise, learning styles, and cognitive status (emotional intelligence) play a critical role in the outcome of academic performance as a successful indicator of achievement. A variety of methods are considered to asses ones academic progress based on results. One such psychometric tool used to differentiate between individuals’ performances is the “measurement.” Academic proficiency measured by IQ in pursuit of achievement was once thought to be synonymous with success. The fact that theoretical insight based on intelligence alone is insufficient for critical thinking has long been recognized; however, recent research reveals that, while intelligence is required for academic achievement, a trainable emotional mind makes a significant difference in success 1
Emotional intelligence (EI) is one of the quantifiable variables. In 1990, EI was realized to play a vital role in human intelligence 1,2,3,4,5. The EI may influence academic performance in school children and it is twice as important as intelligence quotient (IQ) in workplace performance 2 .In 1990, Salovey and Mayer formulated the functional operational definition of EI 6 . When compared to IQ, research over the years has demonstrated that EI is trainable, as Goleman reported in 1995. Contrary to the earlier understanding ,recent studies have revealed EI as a better predictor of success than IQ 1 . Gorgich et al. (2016) suggested that a possible training on EI development is desirable based on their findings on the association between EI and academic achievements 7. Greater awareness of the importance of EI and its incorporation into academics is desirable for improving empathy, practical skills, and academic performance among health students 6,8,9.
According to a systematic review by karkada et al., 2020 10, EI is associated with academic performance. The majority of the studies were cross-sectional studies in health-related students, indicating that there may be a link between EI and academic performance. The majority of these studies reported the ad hoc comparisons of EI with academic performance, either in the first or last year, and no training or awareness program was made available prior to the studies. On the other side, one study 11 found that as students progressed to the next academic year, their EI and academic performance decreased, which is an important finding in the field of education 11,12,13,14,15,16,17.
Iron is one of the most important micronutrients because it is required for many neuro-metabolic activities such as neurotransmitter synthesis, oxygen transport, mitochondrial functions, DNA biosynthesis, and myelin sheath formation, all of which contribute to the overall development of the nervous system 18 . Consequently, any deficiency in dietary supplements, such as iron, will have a negative impact on hemoglobin production. Such low levels of hemoglobin concentration will affect the oxygen-carrying capacity of the blood, resulting in impaired memory and learning capacities, as well as general growth and development, which in some cases may be caused by a cerebral infarct 19,20 . Iron deficiency has been linked to a reduction in dopamine neurotransmission, which can be reflected in cognitive functions associated with motor activity, problem-solving ability, and academic performance 21,22,23. In addition to fatigue and poor memory, attention deficit related to mitochondrial damage in brain neurogenic cells 24 and low academic accomplishment is possible consequences of reduced cognitive function 25,26. Aside from lowering overall health, new research investigations have revealed that youngsters with low hemoglobin profiles have a significant impact on their academic performance in school. Iron deficiency is associated with poor cognitive performance in children and adolescents 27,28,29,30,22,31,32,33,34,35,36,37,21,23. Previous research has revealed that low exam scores in schoolchildren may be associated with microcytic anemia, a blood disorder (Oski, 1993). Most studies stated that anemia is negatively associated with academic performance and nutritional supplements such as iron, which can improve hemoglobin level and thereby may improve academic performance 24.
Modern outcome-based education (OBE) is concerned with improving students’ academic performance through the use of kinesthetic learning techniques. In reference to cardiopulmonary fitness, physical activities are also important in maintaining an individual’s overall health and well-being. The benefits of exercise for weight loss are well recognized, as evidenced by several studies 38,4. Similarly, 3 revealed that students who frequently engage in strength exercise may contribute to academic performance (Keating et al., 2013). Furthermore, Sævarsson et al. (2017) 5 reported that weekly exercise improves the academic performance in 9-year-old school children 2,39,40,5.
Scientometric analysis from 2000 to 2021, reveals very minimal research knowledge on the role of EI and physical exercise in association with academic performance among medical students. The majority of the studies were cross-sectional in nature, with no proper training guidelines provided before their study, either for EI awareness or for exercise regime, nor any standardization of the research methods. When homogeneity among examinations was considered, some matched EI at the start of each year and some at the end of each year, demonstrating a lack of an increasing relationship between the two variables. Most previous studies were conducted with elementary school children, whereas such studies have been reported less frequently among medical student cohorts in general 4. It is critical to investigate and improve students’ perceptions of the benefits of the aforementioned criteria (exercise and EI awareness) in long term implementation. This will ultimately help to improve academic achievement and overall well-being. As a result, the purpose of this study is to determine if there is a long-term association between these multifactorial variables such as EI awareness, an induced physical exercise regime, with normal hemoglobin concentration (nutritional status), and physical fitness index with academic performance.
Materials and Methods
Study design
This longitudinal study involved three phases: (1) Phase-1: pre-intervention; (2) Phase-2: Intervention phase; (3) Phase-3: post-intervention phase, A total of 360 (n = 360) MBBS undergraduate’s students who differed in gender, nationality, and age were enrolled with prior informed consent and approval of relevant ethical clearance (Ref No: RMC/EC08/2018).They were then subjected to screening depending on the set inclusion and exclusion standards based on convenient sampling technique and were further grouped into TEST (T) and CONTROL (C) groups. Each group consisted of 180 (n = 180) students.
In Phase-1, the TEST group was subjected to the following: (1) Stage 1: recording lab-based data; (2) Stage 2: recording questionnaires inputs; (3) Stage 3: recording pre-intervention academic grades, (stipulated module exam) whereas the CONTROL group was only subjected to Stage 3, which consolidated to form baseline data for pre-intervention phase-1.
In Phase-2, only the TEST group received an intervention protocol that is (a) EI measurement and awareness and (b) induced moderate physical exercise regime.
In Phase-3, the TEST group was subjected to a repeat recording of Phase-1: Stage-1, Stage-2: EI measurements and Stage-3 with post-intervention academic grades (final year end professional exam), whereas for CONTROL group only Stage-3 was implemented.
Phase-1: Pre-Intervention
The Phase-1 pre-intervention phase was conducted in three stages:
Stage 1: involved the collection of lab-based data (for the TEST group). Students who agreed to participate in the study were briefed about the research design before being grouped and brought into lab in batches of 30 to be accommodated into six rotating stations. Each station had five students at a given time in the clinical Physiology laboratory. In the Station-1: students signed informed consent; Station-2: students filled in two validated questionnaires that collected information about their demographic details, exercise habits, diet, EI awareness status, and learning styles; Station-3: students measured their anthropometric data (height and weight); Station-4: students measured Harvard step test score; Station-5: students measure their peak flow rate as PFT indicator, values of both station 4 &5 compound to cardiopulmonary fitness ; Station-6: students measured their hemoglobin concentration and oxygen saturation (as an indicator for nutritional status)
Stage 2: questionnaires were filled out (for the TEST group). The EI was measured using The Profile of Emotional Competence (PEC) questionnaire 41. And learning style was measured using the VARK questionnaire (Copyright V.7.8-2014) held by VARK Learn Limited, Christchurch, New Zealand) ( Figure 1; steps 4 & 5)
Stage 3: Pre-intervention academic grade data collection and analysis from the chosen continuous assessment Module Exam for both the TEST and CONTROL groups. ( Figure 2; Pre-grades)
Data generated at the end of Phase-1 reveals a baseline association between EI awareness, learning styles, current types of exercise habits, nutritional status, cardiorespiratory fitness for the TEST group and also comparative academic performance across gender for both TEST and CONTROL (Figure 1; steps 4-7) prior to intervention phase, feedback of which given to students.
Phase-2: Intervention protocol
After completing baseline mapping under Phase-1, the TEST group was subjected to two intervention protocols for the next six months: Moderate brisk walk Exercise-Protocol (MEP) and EI awareness–Protocol (EIP).
Moderate brisk walk Exercise-Protocol (MEP)
Students enrolled attended a lecture session on the basic physiology of physical exercise and its benefits. Following that, the students were given practical instruction on the recommended induced brisk walking of 2-3 sessions/week for 30 minutes/session for the next six months at their own convenient time, preferably in the morning or evening. Students self-recorded their exercise activities in a reflective log sheet under the supervision of research assistance/co-researchers for future analysis.
Emotional Intelligence Protocol (EIP)
During the pre-intervention phase, students were advised to complete a standard vetted internalized (Cronbach’s alpha, 0.7) EI and learning style (VARK) questionnaire to measure their prior EI level and learning style upon enrolment. Students’ EI and learning style results were then analyzed and feedback was given to the students so that they could work on the areas that need improvement. The students then attended a lecture series on emotional awareness and its benefits, according to the delivery mode, and continued to implement and practice the knowledge attained (Figure 1; step 8).
Phase-3: Post-Intervention
The Phase-3 Post-intervention phase was conducted in three steps: After the completion of intervention Phase-2, the TEST group was subjected to
Step 1: Which is repeat measurements of stage 1 and 2 of phase-1 after intervention period followed by (Figure 1; steps 4 & 5)
Step 2: Post-intervention academic grade data collection and analysis from the Final Professional Exam for both the TEST and CONTROL groups (Figure 2; Post-grades)
Step 3: Comparison of measurement results of step1 of phase-3 with stage 1&2 of phase-1 for TEST group and comparison of pre and post academic grades for both TEST and CONTROL group to investigate their association ,that is step 2 of phase-3 with stage -3 of phase -1(Figure 1; steps 8 & 9).
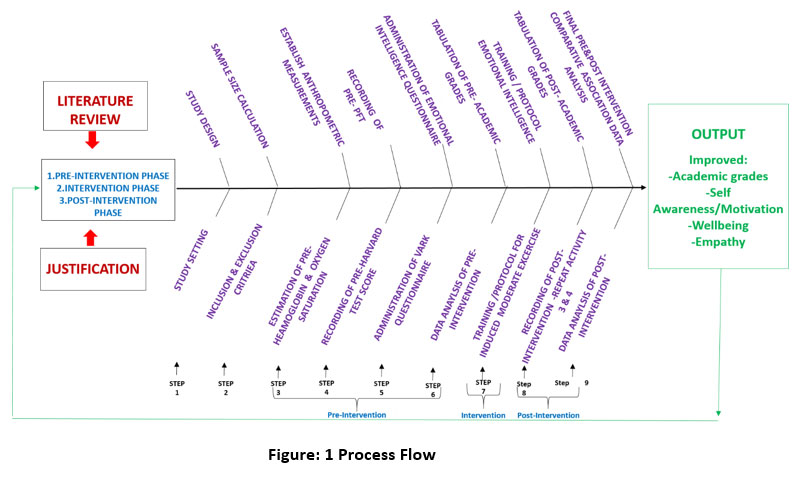 |
Figure 1: Process Flow. |
Results
The final combined data analysis was carried out using Statistical Package for Social Science (SPSS) version 21.0 software. Numerical variables were described as mean ± standard deviation (SD), whereas categorical variables were described as frequency/percentage. The online form, questionnaire, lab reports, and academic grades revealed the following: Descriptive statistics: (Categorical variable) Frequencies or percentage.
The data from Phase-3 was compared to that of Phase-1 to determine the association of the intervention’s combined effect on academic performance for both the TEST and CONTROL groups.
The TEST and CONTROL groups each consisted of about 180 students, with the majority of 107 females (59.4%) and 73 males (40.6%). This difference in gender distribution was reflected in the general natural student’s enrolment in the course. Demographic descriptive analysis of categorical variables for the TEST group reveals 64.3% resided in the hostel, while 35.7% were day scholars. In terms of diet, 63.2% followed a mixed diet, 33.5% were non-vegetarians, and 3.3% were pure vegetarians. In terms of self-physical exercise, 63.8% performed self-directed exercise, while 36.2% did not exercise at all. Further analysis of the type of self-directed exercise among those who mentioned YES reveals that 35.7% did aerobic exercise, 10.3% did resistance type of exercise, while 17.8% did both types of exercise. Mean age of this group being 20.15(±1.301).
Pre (Baseline data ) and Post-Intervention data comparison-Inferential statistics analysis of nutritional status, physical fitness and emotional intelligence -Chi-squared – for the TEST group:
The Chi-squared test analysis was used to determine the association between hemoglobin concentration, oxygen saturation, pulmonary function test (peak expiratory flow rate), Physical fitness index (Harvard step test) among individual gender PRE (as baseline) and POST-interventions, with a p-value of <0.05 considered statistically significant.
There was no any significant association in regard to hemoglobin concentration comparison between pre baseline data record compared to post hemoglobin concentration after intervention phase in males (p = 0.247) expect for females which was significant (p = 0.00001) (normal values of hemoglobin concentration for female- <12 gm/dL – low Hb and > 12 gm/dL normal Hemoglobin. similarly, 13 gm/dL for males). Participants with lower hemoglobin concentrations were referred to a clinic for further investigation and follow-ups.(Table 1.1).
Table 1: 1. Chi square analysis for Pre and Post haemoglobin estimation in male and female.
| Male | Female | ||||||||
| Haemoglobin Pre intervention | Haemoglobin Post intervention | X2 | p value | Haemoglobin Pre intervention | Haemoglobin Post intervention | X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Low | 1 | 17 | 3.098 | .247 | Low | 16 | 17 | 18.613 | 00001* |
| Normal | 0 | 55 | – | – | Normal | 8 | 66 | – | – |
| Total | 1 | 72 | – | – | Total | 24 | 83 | – | – |
There was no any significant association in regard to oxygen saturation comparison between pre baseline data record compared to post oxygen saturation after intervention phase in males (p = 0.301) and females (p = 1.000), (oxygen saturation of 95% and above is considered as normal and that of below 95% is considered as low).(Table 1.2).
Table 1: 2. Chi square analysis for Pre and Post oxygen saturation in male and female.
| Male | Female | ||||||||
| Oxygen saturation Pre intervention | Oxygen saturation Post intervention | X2 | p value | Oxygen saturation Pre intervention | Oxygen saturation Post intervention | X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Low | 0 | 4 | 1.947 | .301 | Low | 5 | 10 | .003 | 1.000 |
| Normal | 23 | 46 | – | – | Normal | 30 | 62 | – | – |
| Total | 23 | 50 | – | – | Total | 35 | 72 | – | – |
There was no any significant association in regard to pulmonary function test (peak expiratory flow(PEF) comparison between pre baseline data record compared to post pulmonary function test after intervention across gender (p = 0.363), (peak expiratory flow value of 400–700L/min is considered as normal and that of below 400 L/min is considered as low) (Table 1.3).
Table 1: 3. Chi square analysis for Pre and Post Pulmonary function test (PFT) with Gender.
| Pre-intervention | Post-Intervention | ||||||||
| Gender | PFT
Pre intervention |
X2 | p value | Gender | PFT
Post intervention |
X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Female | 57 | 50 | 6.824a | .012* | Female | 49 | 58 | 1.011 | .363 |
| Male | 53 | 20 | Male | 39 | 34 | ||||
| Total | 110 | 70 | Total | 88 | 92 | ||||
There was significant association in regard to Harvard test scores comparison between pre baseline data record compared to Harvard test scores after intervention phase in males (p = 0.023) and females (p = 0.00001), (HTS value of 55 is considered as normal and that of below 55 is considered as low) .(Table 1.4).
Table 1: 4. Chi square analysis for Pre and Post Harvard step test among male and female.
| Male | Female | ||||||||
| Harvard score test Pre intervention | Harvard score test Post intervention | X2 | p value | Harvard score test Pre intervention | Harvard score test Post intervention | X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Low | 11 | 14 | 6.379 | .023* | Low | 7 | 28 | 15.408 | .00001* |
| Normal | 8 | 40 | Normal | 0 | 72 | ||||
| Total | 19 | 54 | Total | 7 | 100 | ||||
The independent –sample t-test analysis was used to determine association between global EI scores across gender with a p-value of <0.05 considered statistically significant.
There was no any significant association in regard to emotional intelligence scores comparison between pre-intervention(p=0.255) grades (baseline) data record compared to post-intervention (p = 0.230) grades after intervention phase across gender and also there was no any significant association in regard to global emotional intelligence scores across gender (p = 0.872). .(Table 2.1,2.2,2.3, 2.4).
Pre (Baseline data ) and Post-Intervention data comparison -Inferential statistics analysis of academic grades: Pre-intervention vs Post-intervention test grades across gender for both CONTROL & TEST groups:
The Chi-square test of analysis was used to determine the association between pre and post -intervention grade across gender in CONTROL and TEST groups, with a p-value of <0.05 considered statistically significant.
The CONTROL group pre-test descriptive analysis reveals, out of the 180 participants (107 females and 73 males), 120 passed (66 females and 54 males) and 60 failed (41 females and 19 males).
The TEST group pre-test descriptive analysis reveals, out of the 180 participants (107 females and 73 males), 115 passed (79 females and 36 males) and 65 failed (28 females and 37 males) (Figure 2,3).
The CONTROL group post-test descriptive analysis reveals, out of the 18 participants 0 (107 females and 73 males), 127 passed (73 females and 54 males) and 53 failed (34 females and 19 males).
The TEST group post-test descriptive analysis reveals, out of the 180 participants (107 females and 73 males), 157 passed (103 females and 54 males) and 23 failed (4 females and 19 males) (Figure 2,3).
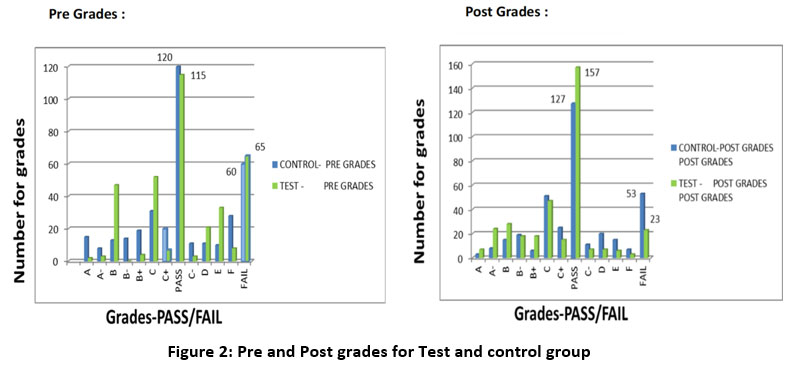 |
Figure 2: Pre and Post grades for Test and control group. |
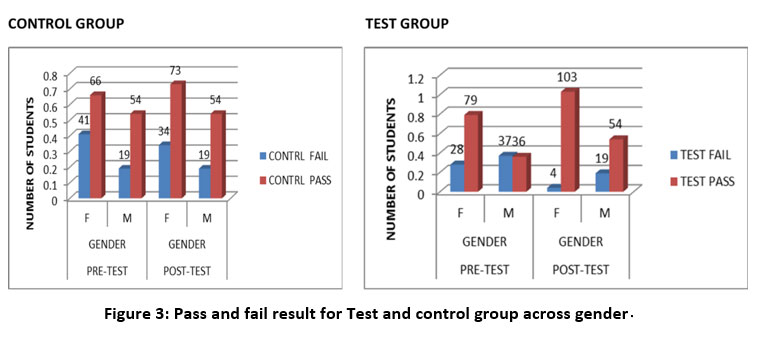 |
Figure 3: Pass and fail result for Test and control group across gender. |
There was no any significant association in regard to academic grades; Pre-intervention grades (baseline) data record of CONTROL(p=0.107) and TEST (p=0.911) in comparison to post-intervention grades of CONTROL (p=0.406) expect for TEST which was significant (p = 0.00001) across gender. (Table 1.5,1.6).
Table 1: 5. Chi square analysis for Pre-Intervention grade across gender for Control and Test group.
| Control group | Test group | ||||||||
| Pre
Intervention grade |
Gender | X2 | p value | Pre
Intervention grade |
Gender | X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Fail | 41 | 19 | 2.950 | .107 | Fail | 28 | 37 | .012 | .911 |
| Pass | 66 | 54 | Pass | 79 | 36 | ||||
|
Total |
107 | 73 | Total | 107 | 73 | ||||
Table 1: 6. Chi square analysis for Post-Intervention grade across gender for Control and Test group
| Control group | Test group | ||||||||
| Post intervention
grade |
Gender | X2 | p value | Post intervention
grade |
Gender | X2 | p value | ||
| Low | Normal | Low | Normal | ||||||
| Fail | 34 | 19 | .690 | .406 | Fail | 4 | 19 | 19.344 | .00001* |
| Pass | 73 | 54 | – | – | Pass | 103 | 54 | – | – |
| Total | 107 | 73 | – | – | Total | 107 | 73 | – | – |
Table 2: 1. Descriptive Statistics of Global Emotional intelligence for Test group
| Descriptive Statistics | |||||
| N | Minimum | Maximum | Mean | Std. Deviation | |
| Global_score | 180 | 132.00 | 212.00 | 160.8556 | 14.63528 |
| Valid N (listwise) | 180 | ||||
Table 2: 2. Global Emotional intelligence score across gender for Test group.
| Global score Vs across gender
|
||||
| Global score | MEAN | SD | t Test value | p value |
| Gender –Male
Female |
160.6389
161.0000 |
14.35889
14.88146 |
-0.162 | 0.872 |
Table 2: 3. Global Emotional intelligence score for Pre and Post-Intervention grade for Test group.
| Global score Vs Pre-intervention grade | ||||
| Global Score | MEAN | SD | t test value | p value |
| Pre-test – Fail
Pass |
159.2000
161.7913 |
13.45618
15.23874 |
1.142 | 0.255 |
Table 2: 4. Global score Vs Post-intervention grade.
| Global Score | MEAN | SD | t test value | p value |
| Post-test – Pass
Fail |
164.1200
160.3290 |
16.41219
14.31696 |
1.203 | 0.230 |
Discussion
In today’s educational environment, it is critical to identify an ideal doable and achievable well-defined process that would result in stable student wellbeing as well as improved academic grades, while also being user-friendly and motivated to yield positive results, particularly in this generation of students.
Based on the limited research data available on the individual element of EI and the contribution of various types of physical exercise to educational improvements at the primary level educational setting, the following conclusions can be drawn: To test the hypothesis, the researchers devised a process and tested whether combining EI awareness with calculated induced moderate physical exercise (BRISK WALKING) administered for approximately 30 minutes per session, 3-4 times a week would result in improved wellbeing among students, which would then promote and enhance academic performance among the tertiary medical university students.42,43,44,45,46,47 .
So, our research aimed at developing a statistically proved design PROCESS with a concept to combine EI awareness along with moderate physical exercise regime among 18-24 years old tertiary medical university students to enhance their academic performance.
According to the research design, about 360 students were enrolled in this research to understand the difference in association of the research outcomes between pre-intervention period compared to post intervention period, in line the sample size was calculated based on [C]correlation factor (r-value) using the standard formula (Total sample size n = [(Zα+Zβ) /C (r) ]2 + 3 =____). The sample size is calculated using the r-value of previously published articles for each parameter in the study, such as EI, learning style, physical fitness, etc. The parameter with the highest r-value (r = 0.206) 48 was chosen as a feasible set point, yielding a final value of 180. Therefor the TEST group consisted of 180 students based on their willingness to participate in the research and go through a lab investigation followed by adherence to intervention protocols. In contrast to the TEST group, students in the CONTROL group were selected randomly with gender similarity to that of the TEST group.
The socio-demographic and anthropometric diversity of the study of both the cohort was most likely similar in ambiance like the average age of the TEST group was about 20.15 years, while that of the CONTROL group was around 21.5 years with majority of them residing in hostel. The overall TEST group height (cm) was 164.43 ± 9.058 and weight (kg) was 62.34 ± 14.779, with the individual distribution of males’ height (cm) being 172.38 ± 6.852 and males’ weight (kg) being 68.91 ± 13.755 and females’ height (cm) being 159.0 ±5.774 and females’ weight (kg) being 57.86 ± 13.796. In terms of TEST group diet , the majority of them was prominent mixed diet and also already engaged in some form of self-directed exercise (Table 1) which enabled the researchers of implementing one of the intervention strategies of induced exercise with the minimal logistical hassle.
Result analysis of baseline data(pre-intervention) compared with that of post-intervention reveals that there were no significant changes in terms of nutritional status (hemoglobin concentration and oxygenation saturation) expect for females in relation to hemoglobin concentration. Likewise, physical fitness revealed significant changes across the gender (Harvard step test) with no changes in respiratory component was observed.
In terms of questionnaires, the implemented VARK questionnaire 49 revealed that the majority of participants were of the Aural category, followed by the Kinesthetic category; accordingly, teaching and learning methodologies were aligned likewise to suit the learning process during the intervention period. For EI awareness measurement, The Profile of Emotional Competence (PEC) 41 self-report ability test questionnaire was used. Spearman’s correlation analysis (mean, SD) and significance of the ten subscales of the questionnaire based on the five domains of EI construct revealed that 1) identifying own emotions (15.617 ± 2.3854) and 2) identifying other emotions (14.589 ± 2.3536) had r = -0.236 and p = 0.001 (moderately negative correlation & significant); 3) understanding own emotions (17.478 ± 3.335) and 4) understanding other emotions (17.478 ± 3.335) had r = 0.231 and p = 0.002 (moderately positive correlation & significant); 5) expression own emotions (16.15 ± 2.3073) and 6) listening to other emotions (16.289 ± 2.471) had r = 0.243 and p= 0.001 (moderately positive correlation & significant); 7) regulation of own emotions (15.7 ± 3.7978) and 8) regulation of other emotions (15.839 ± 3.1942) had r = 0.305 and p = 0.0001 (moderately positive correlation & significant); 9) utilization of own emotions (17.2 ± 2.9718) and 10) utilization of other emotions (14.461±4.1567) had r = 0.133 and p= 0.075 (moderately positive correlation & not significant). Moreover, no significant difference (p = 0.872) was observed in EI between genders in this cohort,(Table 2.1) in contrast to a few studies that have reported females to have higher EI than males 50,51,52,53,54,55.Likewise, comparing the EI global score to academic performance among the TEST group revealed that, there was no statistically significant changes seen even though slight change in p value was observed in post-intervention(p=0.230) academic performance compared to pre-intervention (p = 0.255) academic performance (Table 2.1,2.2). It’s our assumption with more duration and increased sample size we may see significant changes in this regard.
Finally, after six months of the intervention period, a comparison of pre-intervention academic performance data with that of post-intervention data revealed no statistically significant association between academic grades holistically between TEST and CONTROL group in spite of numerical difference in grades among the groups. This could be due to too many categorical values involved, however when compared with gender across the group the difference observed was significant.
Across gender for CONTROL (p = 0.107) and TEST group p-value (p = 0.911) in the pre-intervention period was not significant. (Table 1.5). However, in the post-intervention period, a statistically significant association was observed between academic grades across gender for the TEST group (p = 0.0001) in comparison to the CONTROL group (p = 0.406) (Table 1.6).
Based on the positively associated comparative results, one can postulate that moderate brisk walking exercise improves cardiorespiratory fitness 2,3 by maintaining optimal ventilation-perfusion ratio (V/Q) at the lung and blood capillary interface. The V/Q ratio is important because it is one of the most important factors in maintaining normal arterial blood oxygen and carbon dioxide levels. Moderate exercise increases oxygen uptake and carbon dioxide output up to a factor of twenty above resting values, and this increase in gas exchange is matched by an increase in cardiac output up to some six-fold demands of these gases to and from exercising muscles. During exercise, blood is shunted to other organs, prioritizing exercising muscle and brain tissues. Such physical activities would further aid in the release of endorphins in the central nervous system and pituitary glands, which would enhance overall body functions and possibly aid in memory retention 30. Similarly, cognitive functions and emotions play an important role, as recent studies have shown a recognizable interplay between them.
Further, a systematic literature review in 2016 by Gutiérrez-Cobo et al 56 found that EI may improve cognitive functions concerning performance tests (64.28%) and that when using a self-report ability instrument as a measure, participants with higher EI performed better in cognitive tasks (30.77%) whereas self-report mixed tests had about 37.5% of positive results 56. Both of these scenarios administered together in unison may be the possible reason for positive results.
Conclusion
In summary, data analysis of pre- and post-intervention period of the TEST group revealed a significant difference in improving academic performance prior to intervention period compared with post intervention period, perhaps contributed holistically by adequate tissue oxygenation due to constant oxygen saturation based on stable hemoglobin concentration reflecting nutrition status aided by appropriate cardiorespiratory fitness (assessed by Harvard score test and PFT measurements) achieved through prescribed exercise regime alongside with understanding and handling of emotional intelligence may have awakened the central nervous system areas involved in learning and memory which may have played a vital role in improving academic performance in the long run in comparison to CONTROL Group. Based on the data analysis report in this study, we can conclude that the combined effect of EI awareness with induced moderate physical exercise in line with improved oxygenation and cardio-respiratory fitness is ideal for improving academic grades.
Acknowledgment
We acknowledge UMS for providing access to library facilities for sourcing resource materials and also thank Dr. Pallav Sengupta for formatting/editing, Dr. Sowmya for assisting in data collection and analysis.
Author Contributions
IRK, UJD, and ZM all contributed to the study’s design, review, and conception. The manuscript was drafted, edited, reviewed by IRK, UJD, ZM, and JP. All of the authors have given their consent for submission.
Recommendation
Further research is recommended to study in multiple higher educational settings, such as private and public with a diversified cohort, study their relationship, and follow-up until the completion of their program, which may enable us to understand the holistic impact of the research outcome in their progressive undergraduate study years. However, it is also recommended to determine the research outcome if the frequency and duration of the exercise protocol together with other modes of aerobic exercises such as swimming and jogging are increased in addition to brisk walking.
Limitation
Due to logistical constraints, this research was conducted only at one private health university. The reluctance of some universities in sharing the academic grades of their students, as well as obtaining approved ethical clearance and permission from multiple universities, was time-consuming and difficult to incorporate within the research time frame. Furthermore, the exam patterns and mode of conduction of exams and their assessment weightage, i.e., cut-off pass mark, varied across the university in different exams. Another important challenge is coordinating the timing, funding, and personnel needed for the research in a large cohort.
Conflict of Interest
The authors declared that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Sources
UMS Grant (GRANT: UMSGreat-GUG0251-1/2018).
References
- Low, G.R., and Nelson, D. (2005). Emotional intelligence: The role of transformative learning in academic excellence. Texas study of secondary Education 14, 41-44.
- Zanesco, A., and Antunes, E. (2007). Effects of exercise training on the cardiovascular system: pharmacological approaches. Pharmacology & therapeutics 114, 307-317.
CrossRef - Keating, X.D., Castelli, D., and Ayers, S.F. (2013). Association of weekly strength exercise frequency and academic performance among students at a large university in the United States. The Journal of Strength & Conditioning Research 27, 1988-1993.
CrossRef - Li, J.W., O’connor, H., O’dwyer, N., and Orr, R. (2017). The effect of acute and chronic exercise on cognitive function and academic performance in adolescents: A systematic review. Journal of science and medicine in sport 20, 841-848.
CrossRef - Sævarsson, E.S., Svansdottir, E., Sveinsson, T., Asgeirsdottir, T.L., Arngrimsson, S.A., and Johannsson, E. (2017). Organized leisure-time sport participation and academic achievement in preadolescents. Scandinavian journal of public health 45, 861-868.
CrossRef - Salovey, P., and Mayer, J.D. (1990). Emotional intelligence. Imagination, cognition and personality 9, 185-211.
CrossRef - Gorgich, E., Barfroshan, S., Ghoreishi, G., Balouchi, A., Nastizaie, N., and Arbabisarjou, A. (2016). The association of self-assessed emotional intelligence with academic achievement and general health among students of medical sciences. Glob J Health Sci 8, 55776.
CrossRef - Akerjordet, K., and Severinsson, E. (2010). The state of the science of emotional intelligence related to nursing leadership: an integrative review. Journal of Nursing Management 18, 363-382.
CrossRef - Batt-Rawden, S.A., Chisolm, M.S., Anton, B., and Flickinger, T.E. (2013). Teaching empathy to medical students: an updated, systematic review. Academic Medicine 88, 1171-1177.
CrossRef - Karkada, I.R., D’souza, U.J.A., and Mustapha, J. (2020). Relationship of Emotional Intelligence and Academic Performance among Medical Students: Systematic Review. Universal Journal of Educational Research 8, 72-79.
CrossRef - Austin, E.J., Evans, P., Goldwater, R., and Potter, V. (2005). A preliminary study of emotional intelligence, empathy and exam performance in first year medical students. Personality and individual differences 39, 1395-1405.
CrossRef - Austin, E.J., Evans, P., Magnus, B., and O’hanlon, K. (2007). A preliminary study of empathy, emotional intelligence and examination performance in MBChB students. Medical education 41, 684-689.
CrossRef - Chew, B.H., Zain, A.M., and Hassan, F. (2013). Emotional intelligence and academic performance in first and final year medical students: a cross-sectional study. BMC medical education 13, 1-10.
CrossRef - Naeem, N., Van Der Vleuten, C., Muijtjens, A.M., Violato, C., Ali, S.M., Al-Faris, E.A., Hoogenboom, R., and Naeem, N. (2014). Correlates of emotional intelligence: results from a multi-institutional study among undergraduate medical students. Medical Teacher 36, S30-S35.
CrossRef - Aithal, A.P., Kumar, N., Gunasegeran, P., Sundaram, S.M., Rong, L.Z., and Prabhu, S.P. (2016). A survey-based study of emotional intelligence as it relates to gender and academic performance of medical students. Education for Health 29, 255.
- Ranasinghe, P., Wathurapatha, W., Mathangasinghe, Y., and Ponnamperuma, G. (2017). Emotional intelligence, perceived stress and academic performance of Sri Lankan medical undergraduates. BMC medical education 17, 1-7.
CrossRef - Wijekoon, C.N., Amaratunge, H., De Silva, Y., Senanayake, S., Jayawardane, P., and Senarath, U. (2017). Emotional intelligence and academic performance of medical undergraduates: a cross-sectional study in a selected university in Sri Lanka. BMC medical education 17, 1-11.
CrossRef - Camaschella, C. (2017). New insights into iron deficiency and iron deficiency anemia. Blood reviews 31, 225-233.
CrossRef - Dowling, M.M., Quinn, C.T., Rogers, Z.R., and Buchanan, G.R. (2010). Acute silent cerebral infarction in children with sickle cell anemia. Pediatric blood & cancer 54, 461-464.
CrossRef - Teni, M., Shiferaw, S., and Asefa, F. (2017). Anemia and its relationship with academic performance among adolescent school girls in Kebena District, Southwest Ethiopia. Biotechnology and Health Sciences 4, 1-8.
CrossRef - Bryan, J., Osendarp, S., Hughes, D., Calvaresi, E., Baghurst, K., and Van Klinken, J.-W. (2004). Nutrients for cognitive development in school-aged children. Nutrition reviews 62, 295-306.
CrossRef - Lozoff, B., Brittenham, G.M., Wolf, A.W., Mcclish, D.K., Kuhnert, P.M., Jimenez, E., Jimenez, R., Mora, L.A., Gomez, I., and Krauskoph, D. (1987). Iron deficiency anemia and iron therapy effects on infant developmental test performance. Pediatrics 79, 981-995.
CrossRef - Walker, S.P., Wachs, T.D., Gardner, J.M., Lozoff, B., Wasserman, G.A., Pollitt, E., Carter, J.A., and Group, I.C.D.S. (2007). Child development: risk factors for adverse outcomes in developing countries. The lancet 369, 145-157.
CrossRef - Kusumastuti, F.D.T., Sutaryo, S., and Mulatsih, S. (2014). Correlations between hemoglobin, serum ferritin, and soluble transferrin receptor levels in children aged 6-59 months. Paediatrica Indonesiana 54, 122-126.
CrossRef - Konofal, E., Lecendreux, M., Arnulf, I., and Mouren, M.-C. (2004). Iron deficiency in children with attention-deficit/hyperactivity disorder. Archives of pediatrics & adolescent medicine 158, 1113-1115.
CrossRef - Lozoff, B., Jimenez, E., and Smith, J.B. (2006). Double burden of iron deficiency in infancy and low socioeconomic status: a longitudinal analysis of cognitive test scores to age 19 years. Archives of pediatrics & adolescent medicine 160, 1108-1113.
CrossRef - Oski, F.A., Honig, A.S., Helu, B., and Howanitz, P. (1983). Effect of Iron Therapy on Behavior. Pediatrics 71, 877.
CrossRef - Dallman, P.R., Yip, R., and Johnson, C. (1984). Prevalence and causes of anemia in the United States, 1976 to 1980. Am J Clin Nutr 39, 437-445.
CrossRef - Aukett, M.A., Parks, Y.A., Scott, P.H., and Wharton, B.A. (1986). Treatment with iron increases weight gain and psychomotor development. Arch Dis Child 61, 849-857.
CrossRef - Groner, J.A., Holtzman, N.A., Charney, E., and Mellits, E.D. (1986). A randomized trial of oral iron on tests of short-term memory and attention span in young pregnant women. J Adolesc Health Care 7, 44-48.
CrossRef - Lozoff, B., Jimenez, E., and Wolf, A.W. (1991). Long-term developmental outcome of infants with iron deficiency. N Engl J Med 325, 687-694.
CrossRef - Idjradinata, P., and Pollitt, E. (1993). Reversal of developmental delays in iron-deficient anaemic infants treated with iron. Lancet 341, 1-4.
CrossRef - Pollitt, E. (1993). Iron deficiency and cognitive function. Annu Rev Nutr 13, 521-537.
CrossRef - Oski, F.A. (1993). Iron deficiency in infancy and childhood. N Engl J Med 329, 190-193.
CrossRef - Booth, I.W., and Aukett, M.A. (1997). Iron deficiency anaemia in infancy and early childhood. Arch Dis Child 76, 549-553; discussion 553-544.
CrossRef - Looker, A.C., Dallman, P.R., Carroll, M.D., Gunter, E.W., and Johnson, C.L. (1997). Prevalence of iron deficiency in the United States. Jama 277, 973-976.
CrossRef - Grantham-Mcgregor, S.M., and Ani, C.C. (1999). The role of micronutrients in psychomotor and cognitive development. Br Med Bull 55, 511-527.
CrossRef - Donnelly, J.E., Honas, J.J., Smith, B.K., Mayo, M.S., Gibson, C.A., Sullivan, D.K., Lee, J., Herrmann, S.D., Lambourne, K., and Washburn, R.A. (2013). Aerobic exercise alone results in clinically significant weight loss for men and women: midwest exercise trial 2. Obesity (Silver Spring) 21, E219-228.
CrossRef - Nouchi, R., Taki, Y., Takeuchi, H., Hashizume, H., Nozawa, T., Sekiguchi, A., Nouchi, H., and Kawashima, R. (2012). Beneficial effects of short-term combination exercise training on diverse cognitive functions in healthy older people: study protocol for a randomized controlled trial. Trials 13, 200.
CrossRef - Niermann, C.Y., Kremers, S.P., Renner, B., and Woll, A. (2015). Family Health Climate and Adolescents’ Physical Activity and Healthy Eating: A Cross-Sectional Study with Mother-Father-Adolescent Triads. PLoS One 10, e0143599.
CrossRef - Brasseur, S., Grégoire, J., Bourdu, R., and Mikolajczak, M. (2013). The Profile of Emotional Competence (PEC): development and validation of a self-reported measure that fits dimensions of emotional competence theory. PLoS One 8, e62635.
CrossRef - Tully, M.A., Cupples, M.E., Chan, W.S., McGlade, K. and Young, I.S., 2005. Brisk walking, fitness, and cardiovascular risk: a randomized controlled trial in primary care. Preventive medicine, 41(2), pp.622-628.
- Harveson, A.T., Hannon, J.C., Brusseau, T.A., Podlog, L., Papadopoulos, C., Durrant, L.H., Hall, M.S. and Kang, K.D., 2016. Acute effects of 30 minutes resistance and aerobic exercise on cognition in a high school sample. Research Quarterly for Exercise and Sport, 87(2), pp.214-220.
- Azeem, K., 2011. Effect of twelve weeks brisk walking on blood pressure, body mass index, and anthropometric circumference of obese males. Int J Med Health Biomed Bioengineer Pharma Engineer, 5(11), pp.530-532.
- Chen, C.K., Ismail, N.S. and Al-Safi, A.A., 2016. Effects of brisk walking and resistance training on cardiorespiratory fitness, body composition, and lipid profiles among overweight and obese individuals. Journal of Physical Education and Sport, 16(3), p.957.
- Chien, M.Y., Wu, Y.T., Hsu, A.T., Yang, R.S. and Lai, J.S., 2000. Efficacy of a 24-week aerobic exercise program for osteopenic postmenopausal women. Calcified tissue international, 67(6), pp.443-448.
- Gordon, C.D., Wilks, R. and McCaw-Binns, A., 2013. Effect of aerobic exercise (walking training on functional status and health-related quality of life in chronic stroke survivors: a randomized controlled trial. Stroke, 44(4), pp.1179-1181.
CrossRef - Barchard, K.A., 2003. Does emotional intelligence assist in the prediction of academic success?. Educational and psychological measurement, 63(5), pp.840-858.
CrossRef - Leite WL, Svinicki M, Shi Y.(2010) Attempted validation of the scores of the VARK: Learning styles inventory with multitrait–multimethod confirmatory factor analysis models. Educational and psychological measurement. Apr;70(2):323-39
CrossRef - Arora S, Ashrafian H, Davis R, Athanasiou T, Darzi A, Sevdalis N. Emotional intelligence in medicine: a systematic review through the context of the ACGME competencies. Med Edu 2010;44(8):749-64.
CrossRef - Wagner PJ, Mosley GC, Grant MM, Gore JR, Owens CL. Physicians’ emotional intelligence and patient satisfaction. 2002.
- Aithal AP, Kumar N, Gunasegeran P, Sundaram SM, Rong LZ, Prabhu SP. A survey- based study of emotional intelligence as it relates to gender and academic performance of medical students. Edu Health 2016;29(3):255.
- Wijekoon CN, Amaratunge H, de Silva Y, Senanayake S, Jayawardane P, Senarath U. Emotional intelligence and academic performance of medical undergraduates: a cross- sectional study in a selected university in Sri Lanka. BMC Med Edu 2017;17(1):176.
- Austin EJ, Evans P, Magnus B, O’Hanlon K. A preliminary study of empathy, emotional intelligence and examination performance in MBChB students. Med Edu 2007;41(7):684-9.
- Austin EJ, Evans P, Goldwater R, Potter V. A preliminary study of emotional intelligence, empathy and exam performance in first year medical students. Personal Ind Diff 2005;39(8):1395-405.
- Gutiérrez-Cobo, M.J., Cabello, R., and Fernández-Berrocal, P. (2016). The Relationship between Emotional Intelligence and Cool and Hot Cognitive Processes: A Systematic Review. Front Behav Neurosci 10, 101.
CrossRef

