Malignant Head and Neck Tumors in Basrah: A Clinicopathological Study
 , Hayder S. Hashim2, Sawsan S. Al-Haroon1, Ahmed M. Al-Abbasi3 and Suadad A. Al-Nakshabandi1
, Hayder S. Hashim2, Sawsan S. Al-Haroon1, Ahmed M. Al-Abbasi3 and Suadad A. Al-Nakshabandi1 1Department of Pathology and Forensic Medicine, College of Medicine, University of Basrah, Basrah, Iraq
2Department of Otorhinolaryngology-Head and Neck Surgery, Al-Basrah Teaching Hospital, Basrah, Iraq
3Department of surgery, College of Medicine, University of Basrah, Basrah, Iraq
Corresponding Author E-mail: abeer.ali.almowali@gmail.com
DOI : http://dx.doi.org/10.13005/bpj/2376
Download this article as:
![]()
Malignant tumors of the head and neck exhibit a wide range of histological characteristics and involve multiple locations, therefore considered as a diverse collection of site-specific malignancies. The aim of the study was to evaluate key clinicopathological characteristics of head and neck malignancies in Basrah. In this retrospective study, the histopathological reports of 564 cases with head and neck malignancies were diagnosed in Basrah from 2012 to 2017. All of the cases were analyzed according to the patient's age and gender, as well as the location and histological type of the tumor. The patients' mean age of presentation was 46.45 ±20.75 SD, with about two third of the cases at or over 40 years of age and about 53.19% of cases were males. About 11.52% of the patients were in the age of children and adolescents. Head and neck lymph nodes were the most frequent site (30.67%) involved by malignant tumors, followed by the thyroid gland (20.21%), skin and soft tissues (12.77%), larynx (10.82%) and oral cavity (7.8%), respectively, and the most frequent type of malignancy was squamous cell carcinoma. Hence, the study revealed that head and neck malignancies in Basrah are mainly a disease of elderly, with slight male predominance. Head and neck lymph nodes, followed by thyroid gland, skin and soft tissue, larynx and oral cavity, were the commonest sites, respectively, and squamous cell carcinoma was the most frequent malignant tumor.
KEYWORDS:Basrah; Clinicopathological; Head and neck; Malignancies; Male Predominance; Squamous cell carcinoma
Introduction
Malignancies of the head and neck form a diverse category of site specific tumors that frequently have an aggressive behavior1,2. Such malignant tumors were considered as the sixth most common malignancy around the world with more than 550,000 cases diagnosed each year and approximately 300,000 deaths3,4. The region of the head and neck is complex and malignancies arising from this region can be classified into several anatomical sites: malignancies arising from the nasal cavity and paranasal sinuses, diagnosed each year and approximately 300,000 deaths3,4. The region of the head and neck is complex and malignancies arising from this region can be classified into several anatomical sites: malignancies arising from the nasal cavity and paranasal sinuses, nasopharynx, hypopharynx, larynx, oral cavity, oropharynx, ear, salivary glands, thyroid gland, head and neck lymph nodes, odontogenic tumors, craniofacial bones, skin, soft tissues and paraganglionic system2,5,6. Squamous cell carcinomas arising from the mucosa of the upper aerodigestive tract account for the vast majority of head and neck malignancies1,7,8. However, other types of malignancies of epithelial origin, as well as mesenchymal, lymphoid, endocrine, neural and other cellular backgrounds, do exist9. Most head and neck malignancies, particularly squamous cell carcinoma, are linked to tobacco and alcohol intake10. Furthermore, poor oral sanitation and infection with human papillomavirus are recognizable risk factors for tongue, tonsils and oropharyngeal malignancies11,12,13.The risk of head and neck malignancies increases with age, and literature review revealed that the mean age of presentation was mainly in the 5th-6th decade for the Asian population, while the 7th-8th decade was the mean age of presentation for the North American population14. In addition to age influence, studies show that gender also may play a role and noticed that such malignancies were more in males than females, in general14,15.
Oral and pharyngeal cancers have a significant impact on worldwide affliction of malignancies that is primarily owed to the extensive usage of cigarettes and alcohol and in fact are regarded as the sixth most prevalent cancer worldwide16. Generally speaking, oral cavity squamous cell carcinoma represents the largest group of head and neck malignancies17.
Literature review displays little information concerning head and neck malignancies in Basrah, and most studies were concerned with malignancies of certain sites, mainly the oral cavity. Thus, this study was conducted to explore some epidemiological features of head and neck malignancies in Basrah including most of head and neck regions (even the thyroid gland, bones, skin ,soft tissue and head and neck lymph nodes were included) with a focus on certain clinico-pathological features. Such observations are mandatory to assist global tactics for cancer control.
Materials and Methods
Our data were collected from the histopathological reports of 564 cases with head and neck malignancies diagnosed in Al-Haroon private pathological lab in Basrah from 2012 to 2017 and were retrospectively evaluated. These reports contained information on the morphology and location of the malignant tumors in addition to name, age, gender and complaint of each patient. The study adopted the following exclusion criteria: reports with non-conclusive diagnosis, fine needle aspirate cytology, benign tumors, esophageal malignancies, central nervous system and eye tumors. All of the cases were analyzed according to the patient’s age and gender, as well as the location and histological type of the tumor. The malignant tumors were classified from anatomical point of view as follow: Larynx, oral cavity, oropharynx, nasopharynx, hypopharynx, ear, sinonasal, head and neck lymph nodes, salivary glands and thyroid gland in addition to skin, soft tissue and bone malignant tumors. Data were analyzed by means of SPSS software (Version 24) using the chi-square test. Statistical significance was defined as a P-value of less than 0.05.
Results
A total of 564 specimens of head and neck malignant tumors were submitted to histopathological examination in Al-Haroon private pathological lab in Basrah from 2012 to 2017. The age of the patients ranged from 4 months to 90 years old, with the youngest being the 4-months old infant with neck fibrosarcoma and the oldest were two 90 years old patients, one suffering from Non-Hodgkin lymphoma of a cervical lymph node while the other had oral squamous cell carcinoma. The mean age of patients‘ presentation was 46.45 ± 20.75 SD, with about two third of the patients at or above 40 years of age and the range (51-60) years being the most frequent age of presentation, which was closely tailed by (61-70) years, as shown in table 1, whereas 11.52% of patients were children and adolescent.
Approximately 46.81% of patients were females and 53.19% were males, as in table1, having a male to female ratio of (1:0.88). Most patients had carcinomas (69.33%), followed by lymphomas ( 26.06%), then sarcomas (3.37% ), respectively, as in table 1, the term (others) referred to cases of undifferentiated malignant tumors. Head and neck lymph nodes were the commonest site involved by malignant tumors (secondaries or lymphomas) (30.67%), followed by the thyroid gland (20.21%), skin and soft tissues (12.77%), larynx (10.82%) and oral cavity (7.8%), respectively (the top five malignancies in descending order), as in table 1. After excluding lymph nodes, skin and soft tissue malignancies, the oral cavity was the commonest site regarding malignant head tumors (with the tongue being the commonest location), while the region of the ear was the least affected site (0.71%), as in table 1.
Table 1: Patients distribution based on clinical-demographic criteria and tumors‘ type and site
| Variables | Number of patients | Percent |
| Age group | ||
| 0-10 | 33 | 5.85 |
| 11-20 | 44 | 7.8 |
| 21-30 | 69 | 12.23 |
| 31-40 | 66 | 11.7 |
| 41-50 | 88 | 15.6 |
| 51-60 | 106 | 18.79 |
| 61-70 | 102 | 18.09 |
| 71-80 | 44 | 7.8 |
| 81-90 | 12 | 2.13 |
| Gender | ||
| Female | 264 | 46.81 |
| Male | 300 | 53.19 |
| Tumor type | ||
| Carcinoma | 391 | 69.33 |
| Sarcoma | 19 | 3.37 |
| Lymphoma | 147 | 26.06 |
| Others | 7 | 1.24 |
| Tumor site | ||
| Thyroid gland | 114 | 20.21 |
| Head and neck lymph nodes | 173 | 30.67 |
| Larynx | 61 | 10.82 |
| Oral cavity | 44 | 7.8 |
| Oropharynx | 12 | 2.13 |
| Nasopharynx | 33 | 5.85 |
| Hypopharynx | 8 | 1.42 |
| Sinonasal | 11 | 1.95 |
| Salivary glands | 14 | 2.48 |
| Ear | 4 | 0.71 |
| Skin and soft tissue | 72 | 12.77 |
|
Bone |
18 |
3.19 |
In males, the (51-60) years age group was the most frequent age of presentation, closely followed by (61-70) years, while females were mostly presented in the age group of (61-70) years, closely tailed by (41-50) years, as shown in table 2, the relation between age distribution and gender was statistically not significant.
Table 2: Age distribution of malignant tumors in relation to gender
| Range of age | Gender distribution | |||
| Males | Females | |||
| Number | Percent | Number | Percent | |
| 0-10 | 15 | 5 | 18 | 6.82 |
| 11-20 | 24 | 8 | 20 | 7.58 |
| 21-30 | 33 | 11 | 36 | 13.64 |
| 31-40 | 32 | 10.67 | 34 | 12.88 |
| 41-50 | 44 | 14.67 | 44 | 16.67 |
| 51-60 | 64 | 21.33 | 42 | 15.91 |
| 61-70 | 54 | 18 | 48 | 18.18 |
| 71-80 | 28 | 9.33 | 16 | 6.06 |
| 81-90 | 6 | 2 | 6 | 2.27 |
| Total | 300 | 100% | 264 | 100% |
The evaluation of the relation between the histological type and site of the malignant tumor revealed that carcinoma was the predominant malignancy of all sites excluding the head and neck lymph nodes and oropharynx, where lymphoma was the predominant type, as displayed in table 3. The relation was statistically significant.
Table 3: Site distribution of malignant tumors in relation to tumor’s type
| Site | Type of malignant tumor | |||||||
| Carcinoma | Sarcoma | Lymphoma | Others | |||||
| Number | Percent | Number | Percent | Number | Percent | Number | Percent | |
| Thyroid gland | 113 | 99.12 | 1 | 0.88 | 0 | 0 | 0 | 0 |
| Head and neck lymph nodes | 45 | 26.01 | 0 | 0 | 126 | 72.83 | 2 | 1.16 |
| Larynx | 61 | 100 | 0 | 0 | 0 | 0 | 0 | 0 |
| Oral cavity | 43 | 97.73 | 1 | 2.27 | 0 | 0 | 0 | 0 |
| Oropharynx | 2 | 16.67 | 0 | 0 | 10 | 83.33 | 0 | 0 |
| Nasopharynx | 29 | 87.88 | 0 | 0 | 4 | 12.12 | 0 | 0 |
| Hypopharynx | 8 | 100 | 0 | 0 | 0 | 0 | 0 | 0 |
| Sinonasal | 5 | 45.45 | 3 | 27.27 | 2 | 18.18 | 1 | 9.09 |
| Salivary glands | 9 | 64.29 | 0 | 0 | 2 | 14.29 | 3 | 21.43 |
| Ear | 3 | 75 | 1 | 25 | 0 | 0 | 0 | 0 |
| Skin and soft tissue | 63 | 87.5 | 8 | 11.11 | 1 | 1.39 | 0 | 0 |
| Bone | 10 | 55.56 | 5 | 27.78 | 2 | 11.11 | 1 | 5.56 |
Histological evaluation of the malignant tumors revealed that squamous cell carcinoma was the most frequent type (26.42%), followed by papillary carcinoma (17.38%), Hodgkin lymphoma (14.54%), Non-Hodgkin lymphoma (11.52%) and basal cell carcinoma (8.87%), that were the top five histological subtypes, respectively, as shown in Figure 1. The study also revealed that papillary carcinoma was the commonest malignancy of the thyroid gland, lymphoma (mainly Hodgkin lymphoma) was the commonest malignancy in head and neck lymph nodes, squamous cell carcinoma was nearly the only type of malignancy found in the larynx and hypopharynx, and was the commonest malignancy in the oral cavity and ear, meanwhile, Non-Hodgkin lymphoma in oropharynx, nasopharyngeal carcinoma in nasopharynx, embryonic rhabdomyosarcoma in sinonasal region, mucoepidermoid carcinoma in the salivary glands, basal cell carcinoma in skin and soft tissue and secondary squamous cell carcinoma in bone, where the most frequent malignancies in these sites, as shown in table 4.
 |
Figure 1: The histological types of malignant tumors |
Table 4: The commonest malignant tumor according to tumor‘s site
| Site | The most frequent malignant tumor | Number of cases | Percent | Other malignant tumors | Percent | Total number of cases |
| Thyroid gland | Papillary carcinoma | 98 | 85.96 | 16 | 14.04 | 114 |
| Head and neck lymph nodes | Hodgkin lymphoma | 82 | 47.4 | 91 | 52.6 | 173 |
| Larynx | Squamous cell carcinoma | 60 | 98.36 | 1 | 1.64 | 61 |
| Oral cavity | Squamous cell carcinoma | 39 | 88.64 | 5 | 11.36 | 44 |
| Oropharynx | Non Hodgkin lymphoma | 10 | 83.33 | 2 | 16.67 | 12 |
| Nasopharynx | Nasopharyngeal carcinoma | 25 | 75.76 | 8 | 24.24 | 33 |
| Hypopharynx | Squamous cell carcinoma | 8 | 100 | 0 | 0 | 8 |
| Sinonasal | Embryonic rhabdomyosarcoma | 3 | 27.27 | 8 | 72.73 | 11 |
| Salivary glands | Mucoepidermoid carcinoma | 4 | 28.57 | 10 | 71.43 | 14 |
| Ear | Squamous cell carcinoma | 3 | 75 | 1 | 25 | 4 |
| Skin and soft tissue | Basal cell carcinoma | 50 | 69.44 | 22 | 30.56 | 72 |
| Bone | Secondary squamous cell carcinoma | 10 | 55.56 | 8 | 44.44 | 18 |
The study also revealed that carcinomas were more common in patients with the age within (51-70) years, sarcomas were more common within (0-10) years, while lymphomas were more in the ages among (11-30) years, as in table 5, and the relation between age distribution and type of malignant tumor was statistically significant. It is also worth mentioning that about 66.15% of children and adolescents in the study had lymphoma.
Furthermore, lymphomas were more frequent in males, sarcomas were slightly more in males, while carcinomas were nearly equal in both genders, as in table 5, the relation between gender distribution and type of malignant tumor was statistically not significant. The study also displayed that all malignant tumors were more frequent above 40 years of age except head and neck lymph nodes and thyroid gland malignancies that were more frequently involved below the age of 40 years, as in table 6, the relation between tumor‘s site and age distribution was statistically significant. Moreover, all tumors were more frequent among females except for malignancies of the head and neck lymph nodes, larynx, oropharynx, nasopharynx and hypopharynx which were more frequent among males, as shown in table 7, in fact the thyroid gland was the commonest site involved in females, followed by head and neck lymph nodes, as compared to males where head and neck lymph nodes were the commonest site, followed by the larynx, the relation between tumor‘s site and gender distribution was statistically significant.
Table 5: Age and gender distributions of patients according to the type of malignant tumor
| Variable
|
Type of malignant tumor | |||||||
| Carcinoma | Sarcoma | Lymphoma | Others | |||||
| Range of age | Number | Percent | Number | Percent | Number | Percent | Number | Percent |
| 0-10 | 2 | 0.51 | 6 | 31.58 | 21 | 14.29 | 4 | 57.14 |
| 11-20 | 13 | 3.32 | 2 | 10.53 | 29 | 19.73 | 0 | 0 |
| 21-30 | 41 | 10.49 | 1 | 5.26 | 27 | 18.37 | 0 | 0 |
| 31-40 | 48 | 12.28 | 1 | 5.26 | 16 | 10.88 | 1 | 14.29 |
| 41-50 | 67 | 17.14 | 3 | 15.79 | 17 | 11.56 | 1 | 14.29 |
| 51-60 | 88 | 22.51 | 3 | 15.79 | 14 | 9.52 | 1 | 14.29 |
| 61-70 | 86 | 21.99 | 2 | 10.53 | 14 | 9.52 | 0 | 0 |
| 71-80 | 36 | 9.21 | 1 | 5.26 | 7 | 4.76 | 0 | 0 |
| 81-90 | 10 | 2.56 | 0 | 0 | 2 | 1.36 | 0 | 0 |
| Gender | Number | Percent | Number | Percent | Number | Percent | Number | Percent |
| Male | 199 | 50.9 | 10 | 52.63 | 87 | 59.18 | 4 | 57.14 |
| Female | 192 | 49.1 | 9 | 47.37 | 60 | 40.82 | 3 | 42.86 |
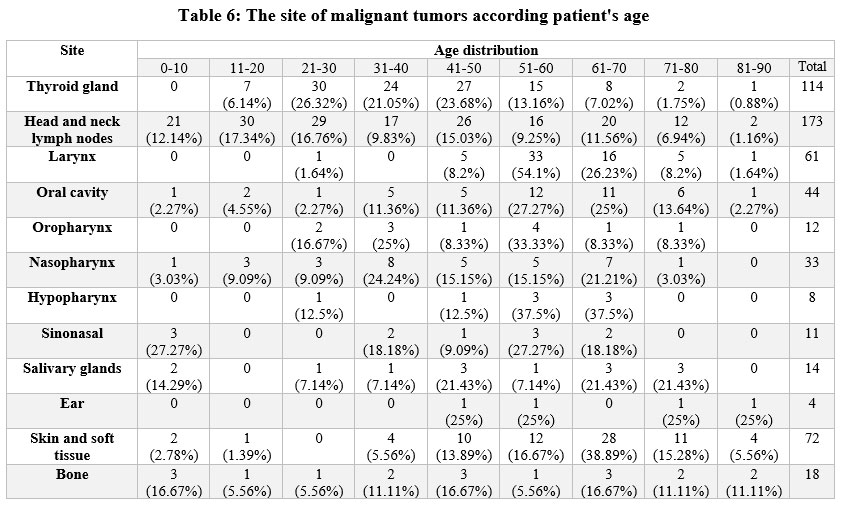 |
Table 6: The site of malignant tumors according patient’s age |
Table 7: The site of malignant tumors according to patient’s gender
| Site | Gender | ||||
| Male | Female | Total | |||
| Number | Percent | Number | Percent | ||
| Thyroid gland | 42 | 36.84 | 72 | 63.16 | 114 |
| Head and neck lymph nodes | 104 | 60.12 | 69 | 39.88 | 173 |
| Larynx | 51 | 83.61 | 10 | 16.39 | 61 |
| Oral cavity | 18 | 40.91 | 26 | 59.09 | 44 |
| Oropharynx | 9 | 75 | 3 | 25 | 12 |
| Nasopharynx | 20 | 60.61 | 13 | 39.39 | 33 |
| Hypopharynx | 6 | 75 | 2 | 25 | 8 |
| Sinonasal | 4 | 36.36 | 7 | 63.64 | 11 |
| Salivary glands | 6 | 42.86 | 8 | 57.14 | 14 |
| Ear | 1 | 25 | 3 | 75 | 4 |
| Skin and soft tissue | 31 | 43.06 | 41 | 56.94 | 72 |
| Bone | 8 | 44.44 | 10 | 55.56 | 18 |
This retrospective study is the first study carried out to highlight the occurrence of head and neck malignant tumors in correlation to clinical-pathological criteria in Basrah. Malignancies of head and neck involve several histological types and sites, and in our study, the thyroid gland, head and neck lymph nodes, skin, soft tissue and bone were assessed, in addition to the traditional head and neck regions like larynx, oral cavity, oropharynx, hypopharynx, nasophaynx, salivary glands, ear and sinonasal regions. The study revealed that about two third of the cases were at or above the age of 40 years at time of diagnosis in both males and females, in fact the most frequent age group was within the 6th decade closely followed by the 7th decade of life. Therefore malignant head and neck tumors were less common in young aged individuals less than 40 years of age, such results were consistent with the findings seen in other studies3,11,18,19,20,21,22,23,24. The study also revealed that the most frequent age group among males was (51-60) years, as compared to females (61-70) years.
Males were slightly more affected than females presenting a male to female ratio of (1:0.88), which in a way resembles results of other studies were males were more affected than females but most studies had a higher male to female ratio3,5,11,12,14,15,20,23,24,25,26,27. The male predominance could be attributed to some habits that have been regarded as risk factors for malignant tumors of head and neck like smoking and alcohol abuse that are strongly related to male gender and to some extent, may be attributed to the protective effect of estrogen exposure in females28. However, a study performed by Hamideh Kadeh et al. showed a female predominance in head and neck malignancies19.
Most of the cases were carcinomas, followed by lymphomas while sarcomas represent only a small fraction of cases, suggesting that most risk factors are carcinogenic agents, which is in agreement with several studies worldwide15,19,23. Nevertheless, a study in Nigeria reported by Y B Amusa et al. showed lymphoma to be the commonest head and neck malignancy but was mainly found in children29, which is similar to the findings in our study since about 66,15% of children and adolescents in the study suffered from lymphoma.
The top five sites involved by head and neck malignancies included head and neck lymph nodes, thyroid gland, skin and soft tissue, larynx and oral cavity, respectively, in a descending order. The result disagrees with several studies, some of which displayed the oral cavity as the commonest site3,5,15,21,22,27,29, others revealed the larynx as the commonest site11,14,24,26, some showed the skin to be the commonest site2,18,19, while a study performed in Bhutan by Phub Tshering et al. showed the thyroid gland to be the most effected site30.The differences from these studies may be contributed in part to the variation of genetic background and exposure to risk factors, in addition to the fact that our study included head and neck lymph nodes, thyroid gland, skin, soft tissue and bone, some of which were not included in most of the mentioned studies. As stated previously, after the exclusion of skin, soft tissue and lymph nodes malignancies, oral cavity malignant tumors were the commonest malignancies of the head, with squamous cell carcinoma being the commonest type which is similar to results of Hamideh Kadeh et al.19. The tongue was the most common location for oral cancer, that was in agreement with several studies11,18,26, although studies reported by Md Salahuddin Siddiqui et al.14 and Hamideh Kadeh et al.19 showed the buccal mucosa to be the commonest site, while Yasmin Bhurgri et al.22 exhibited the mucosa cheek as the commonest. The ear was the least affected site and this result is consistent with a study reported by Y B Amusa29.
Squamous cell carcinoma was the most frequent malignancy in our study, and is similar to many literatures done worldwide3,12,14,19,20,21,22,24,26,30. However, a study conducted by Khadijeh Abdal et al. showed basal cell carcinoma to be the commonest head and neck malignancy18. In addition, the study revealed that the top five most frequent histological types of malignant tumors were squamous cell carcinoma, papillary carcinoma, Hodgkin lymphoma, Non-Hodgkin lymphoma and basal cell carcinoma, in descending order, other histological types were less common.
Further sub site analysis in relation to the malignant tumor‘s histology, revealed that papillary carcinoma was the commonest malignancy of the thyroid gland that is supported by various studies2,11,30, and lymphoma was the commonest malignancy in head and neck lymph nodes that is similar to the finding reported by Rad M. et al.2. Squamous cell carcinoma was approximately the single type of malignancy identified in the larynx and hypopharynx that is close to findings of other studies11,26,30,and was the commonest malignancy in the oral cavity and ear which approximates the results of other researches11,30, meanwhile, lymphoma was the commonest malignancy in the oropharynx which is similar to the results of Mohammad Hasan Larizadeh et al.11 and Hamideh Kadeh et al.19, nasopharyngeal carcinoma in nasopharynx, that is similar to Phub Tshering results30, embryonic rhabdomyosarcoma in sinonasal region, mucoepidermoid carcinoma in the salivary glands resembling results of salivary glands in other studies2,11,30, basal cell carcinoma was the commonest malignancy in skin and soft tissue that is consistent with other observations2,19 and secondary squamous cell carcinoma was the commonest malignancy in bone, as reported by Rad M. et al.2.
In this study, patients diagnosed with carcinoma were older than those with lymphoma and sarcoma, which is consistent to other studies11. With the exception of the thyroid gland and head and neck lymph nodes, all other sites involved by malignant tumors were more frequent in patients above the age of 40 years i.e. the risk of malignancy in general, increases with age. Furthermore, thyroid gland followed by head and neck lymph nodes were the most frequent sites involved by malignant tumors in females, as compared to males where head and neck lymph nodes followed by the larynx were the most frequent sites.
Conclusion
The study revealed that head and neck malignancies in Basrah are mainly a disease of elderly, with slight male predominance. Head and neck lymph nodes, followed by thyroid gland, skin and soft tissue, larynx and oral cavity were the commonest sites involved, respectively, and squamous cell carcinoma was the most frequent malignancy.
Conflict of Interest
The authors declare no conflict of interests.
Funding Sources
There are no funding sources.
References
- Sara I. Pai, William H. Westra. Molecular Pathology of Head and Neck Cancer: Implications for Diagnosis,Prognosis, and Treatment.Annu Rev Pathol.2009; 4: 49–70 (2009).
- Rad M., Chamani G., Zarei MR., Hashemipour M. Epidemiological Aspects of Head and Neck Cancers in a Group of Iranian Population. Shiraz Univ Dent J. 2010; 10:50-56 (20010).
CrossRef - Rajab A AlZahrani. Epidemiological Study of Head and Neck Cancer in Al-Baharegion,South West of Saudi Arabia. J Otolaryngol Rhinol. 2020; 6(2):1-5.
CrossRef - Ilona Argirion,Katie R.Zarins, Kali Defever, Krittika Suwanrungruang, Joanne T. Chang,Donsuk Pongnikorn, et al. Temporal Changes in Head and Neck Cancer Incidence in Thailand Suggest Changing Oropharyngeal Epidemiology in the Region. Journal of Global Oncology.2019;5:1-11.
CrossRef - Maurício José Cabral Ruback, Ana Lívia Galbiatti, Lidia Maria Rebolho Batista Arantes, Gustavo Henrique Marucci, Anelise Russo, Mariangela Torreglosa Ruiz-Cintra,et al.Clinical and epidemiological characteristics of patients in the head and neck surgery department of a university hospital.Sao Paulo Med J. 2012; 130(5):307-13.
- Napadon Tangjaturonrasme, Patravoot Vatanasapt, Andrey Bychkov. Epidemiology of head and neck cancer in Thailand. Asia-Pac J Clin Oncol. 2018;14:16-22.
- Zahra Madjd, Sami Khalaf, Seta Sarkis, Elham Kalantari, Penelope Shihab, Khaled Al-Qaoud, et al. PREVALENCE OF HIGH-RISK HPV 16 IN ORAL SQUAMOUS CELL CARCINOMA AND ITS ASSOCIATION WITH SHH, GLI-1, AND GLI-2 OVEREXPRESSION: A GENOTYPING STUDY. Basrah Journal Of Surgery. 2016;22(2): 52-59.
CrossRef - Sandra Perdomo, Guillermo Martin Roa, Paul Brennan, David Forman, Mónica S. Sierra. Head and neck cancer burden and preventive measures in Central and South America. Cancer Epidemiology 44S (2016):S43–S52.
CrossRef - Natasha Cohen, Stacey Fedewa, Amy Y.Chen.Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofacial Surg Clin N Am 30 (2018): 381–395.
CrossRef - Nadarajah Vigneswaran, Michelle D. Williams. Epidemiological Trends in Head and Neck Cancer and Aids in Diagnosis. Oral Maxillofac Surg Clin North Am. 2014 May; 26(2): 123–141.
CrossRef - Mohammad Hasan Larizadeh, Mohammad Ali Damghani, Mohammad Shabani. Epidemiological Characteristics of Head and Neck Cancers in Southeast of Iran.Iranian Journal of Cancer Prevention. 2014; 2:80-6.
- Andreas Dittberner, Benedikt Friedl, Andrea Wittig, Jens Buentzel, Holger Kaftan,Daniel Boeger, et al. Gender Disparities in Epidemiology, Treatment, and Outcome for Head and Neck Cancer in Germany:A Population-Based Long-Term Analysis from 1996 to2016 of the Thuringian Cancer Registry.Cancers.2020;12(11):1-14.
CrossRef - JS Hocking, A Stein, EL Conway, D Regan, A Grulich, M Law, et al. Head and neck cancer in Australia between 1982 and 2005 show increasing incidence of potentially HPV-associated oropharyngeal cancers. British Journal of Cancer. 2011; 104: 886 – 891.
CrossRef - Md Salahuddin Siddiqui1, Rajeev Chandra, Abdul Aziz, Saurav Suman. Epidemiology and Histopathological Spectrum of Head and Neck Cancers in Bihar, a State of Eastern India.Asian Pacific Journal of Cancer Prevention.2012;13:3949-3953.
- Japhet M. Gilyoma, Peter F. Rambau, Nestory Masalu, Neema M. Kayange, Phillipo L.Chalya.Head and neck cancers: a clinico ‑pathological profile and management challenges in a resource‑limited setting.BMC Res Notes.2015; 8:772:1-9.
- Daniel M Saman. A review of the epidemiology of oral and pharyngeal carcinoma: update. Head Neck Oncolo. 2012; 4:1:1-7.
- Jin Soo Song, Patrick Vallance, Vincent Biron,Caroline C. Jeffery. Epidemiological trends of head and neck Cancer survivors in Alberta: towards improved understanding of the burden of disease. Journal of Otolaryngology – Head and Neck Surgery.2020;49:46:1-6.
- Khadijeh Abdal, Samira Mostafazadeh, Marziyeh Darvishi. The frequency of tumors of the head and neck in a 10-year period in Ilam, Iran. J Bas Res Med Sci. 2018; 5(4):22-27.
CrossRef - Hamideh Kadeh, Shirin Saravani, Babak Moradbeiki.Epidemiological aspects of head and neck cancers in a population of south east region of Iran. Caspian J of Dent Res.2015;4(2):33-39.
- S. Mamoudou Garba, H. Hami, H. Mahamadou Zaki, A. Soulaymani, H. Nouhou, A. Mokhtari, et al. Descriptive epidemiology of head and neck cancer in Niger:First results from the National Cancer Registry. Annals of Oncology.2020;31(6) ,S1352. :DOI:https://doi.org/10.1016 /j.annonc. 2020.10.277.
CrossRef - Mohammad Shadab Alam, Shahid Ali Siddiqui, Roshan Perween. Epidemiological profile of head and neck cancer patients in Western Uttar Pradesh and analysis of distributions of risk factors in relation to site of tumor. Journal of Cancer Research and Therapeutics. 2017; 13(3):430-435.
- Yasmin Bhurgri, Asif Bhurgri, Ahmed Usman, Shahid Pervez, Naila Kayani,Imtiaz Bashir,et al. Epidemiological Review of Head and Neck Cancers in Karachi. Asian Pacific J Cancer Prev.2006;7(2):195-200.
- Bukola F Adeyemi, Lola V Adekunle, Bamidele M Kolude, Effiong E U Akang, Jonathan O Lawoyin. Head and Neck Cancer—A Clinico pathological Study in a Tertiary Care Center. Journal of the National Medical Association.2008;100(6):690-697.
CrossRef - Andre´ Lopes Carvalho, Ineˆs Nobuko Nishimoto, Joseph A. Califano, Luiz Paulo Kowalski. Trends in incidence and prognosis for head and neck cancer in the United States: A site-specific analysis of the SEER database. Int. J. Cancer. 2005;114(5):806–816.
CrossRef - Esra Attar, Subhojit Dey, Ahmad Hablas, Ibrahim A. Seifeldin, Mohamed Ramadan,Laura S. Rozek, et al. Head and Neck Cancer in a Developing Country: A Population-Based Perspective Across 8 Years. Oral Oncol. 2010; 46(8): 591–596.
CrossRef - Kwang-Moon Kim, Young Mo Kim,Yoon-Sang Shim, Kwang Hyun Kim,Hyuck Soon Chang, Jong Ouck Choi, et al. Epidemiologic Survey of Head and Neck Cancers in Korea. J Korean Med Sci.2003 ;18:80-7.
- Sandra P. Perdomo, Paula A. Rodriguez, Jose A. Hakim, Yubelly Avello, David A. Suarez, Alberto Escallón,et al. Abstract 4193: Epidemiological and clinical description of head and neck cancer cases in Bogotá, Colombia.Cancer research. 2019 ;79 (13). DOI: 10.1158 / 1538-7445 .AM2019 – 4193.
- Dana Hashim, Samantha Sartori, Carlo La Vecchia, Diego Serraino, Luigino Dal Maso, Eva Negri, et al. Hormone factors play a favorable role in female head and neck cancer risk. Cancer Medicine. 2017; 6(8):1998–2007.
CrossRef - Y B Amusa, J K Olabanji, V O Akinpelu, S O Olateju, E A Agbakwuru, N Ndukwe,et al. Pattern of head and neck malignant tumours in a Nigerian teaching hospital–a ten year review. West Afr J Med.2004; 23(4):280-5.
- Phub Tshering, Sithar Dorjee, Tshering Dendup, Thinley Dorji, Dechen Wangmo. Epidemiological and histopathological characteristics of head and neck cancers in Bhutan from 2011 to 2017: a retrospective descriptive study. ecancer. 2020;14:1024.
CrossRef




