
Manuscript accepted on :15-10-2021
Published online on: 04-11-2021
Plagiarism Check: Yes
Reviewed by: Dr. Ana Golez
Second Review by: Dr. Mohamed Ali
Final Approval by: Dr. Fai Poon
T S Subbiah , Athira Gopinathan*and Balamurugan Ramachandran
, Athira Gopinathan*and Balamurugan Ramachandran
Department of General Surgery, SRM Medical College Hospital and Research Centre, SRM Institute of Science and Technology, SRM Nagar, Kattankulathur - 603203, Kancheepuram, Chennai, Tamil Nadu India, 603203.
Corresponding Author E-mail: tssismyname@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2316
Abstract
Trauma is the second largest cause of disease worldwide accounting for more than 16 % of global burden 1. By the next decade, the World Health Organization (WHO) estimates that trauma will be the leading cause of Years of Potential Life Lost (YPLL) amongst the world population. With advancement in infrastructure and economic prosperity, accidental trauma due to vehicular accidents has become more commonplace. A majority of victims of motor vehicular accidents present with Blunt abdominal trauma, which due to the complexity in diagnosis and management, presents with significant morbidity and mortality2. Introduced in the 1970s in Europe, point of care Ultrasonographic examination of the abdomen in trauma called as FAST (Focussed Assessment with Sonography for Trauma) has become a routine in emergency rooms worldwide 3. The Blunt Abdominal Trauma scoring system was developed to better diagnose intra-abdominal injury after blunt abdominal trauma 4. This study is aimed in comparing the findings of FAST and BATSS in predicting intra-abdominal injury accurately.
Keywords
Abdominal Trauma ; Blunt Abdominal Injury; Blunt Abdominal Trauma Scoring System (BATSS); Focussed Assessment with Sonography for Trauma (FAST); Intra-abdominal injury; Trauma surgery
Download this article as:| Copy the following to cite this article: Subbiah T.S, Gopinathan A, Ramachandran B. Comparison of Blunt Abdominal Trauma Scoring System (BATSS) versus FAST in assessment of Blunt Trauma Abdomen. Biomed Pharmacol J 2021;14(4). |
| Copy the following to cite this URL: Subbiah T.S, Gopinathan A, Ramachandran B. Comparison of Blunt Abdominal Trauma Scoring System (BATSS) versus FAST in assessment of Blunt Trauma Abdomen. Biomed Pharmacol J 2021;14(4). Available from: https://bit.ly/3bEX4UC |
Introduction
Blunt abdominal trauma may occur due to vehicular accidents, accidental fall, assault, workplace injuries, sporting injuries and explosive injuries. Due to its initially dormant presentation, blunt abdominal trauma is often overlooked 5, unless looked for deliberately. This prolongs the time required to arrive at a diagnosis and subsequent delay in beginning aggressive treatment, making this condition a one with poor outcomes.
Despite the large strides made in diagnosis, infrastructure and development of protocols in trauma management, the morbidity and mortality remains at large 6. Factors contributing to this may include increased interval between point of trauma and hospitalization, unavailability of adequate equipment or trained personnel, delay in arriving at a diagnosis, lack of infrastructure for providing supportive and intensive care post operatively and associated traumatic injury to the brain, spine, pelvis or chest 7.
This study has been chosen to analyse the efficacy of Blunt Abdominal Trauma Scoring System (BATSS) in assessment of blunt trauma to the abdomen in patients presenting at SRM Medical College Hospital & Research Centre, Kancheepuram District, Tamil Nadu, India.
Materials and Methods
The study was carried out in Department of General Surgery, SRM Medical College Hospital & Research Centre, SRM Institute of Science and Technology from May 2018 to September 2019. All injured were brought to an emergency resuscitation area where primary-survey, resuscitation, and a secondary –survey in a standard, method were conducted. The Focussed Assessment with Sonography for Trauma (FAST) investigation was performed during primary-survey, after securing airway and establishing adequate oxygenation/ventilation.
The FAST investigation was classified as positive (clearly showing fluid on at least one window), or negative. No quantitative score system will be used for the quantity of fluid seen.
Patients were scored based on a 24 point Blunt Abdominal Trauma Scoring system (BATSS) 4.
| Criteria | Score |
| Abdominal pain | 2 |
| Abdominal Tenderness | 3 |
| Chest wall signs | 1 |
| Pelvic fracture | 5 |
| FAST Scan positive | 8 |
| Systolic Blood Pressure > 100 mmHg | 4 |
|
Pulse Rate > 100/min |
1 |
The findings of FAST and BATSS were correlated with CECT Abdomen which was taken as the gold standard. Patients who were treated conservatively on admission were followed up for a period of one week. Results were analysed using SPSS 18 software.
Results
A total of 100 cases of blunt abdominal trauma were studied of which 56% were male and 44 % were female. Of these patients, a majority of 48 % were between the ages 21-40.
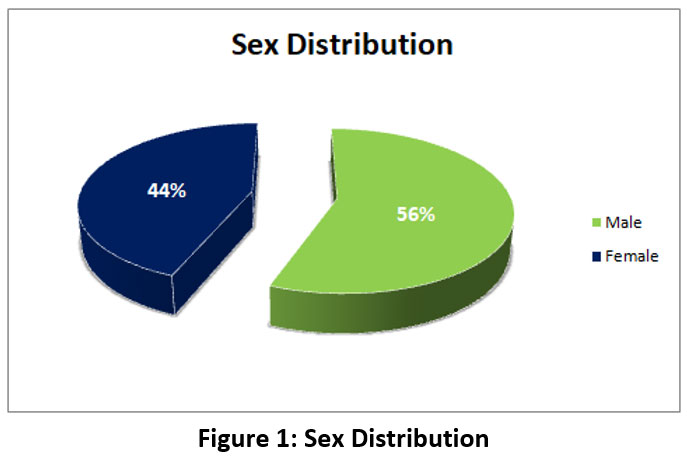 |
Figure 1: Sex Distribution |
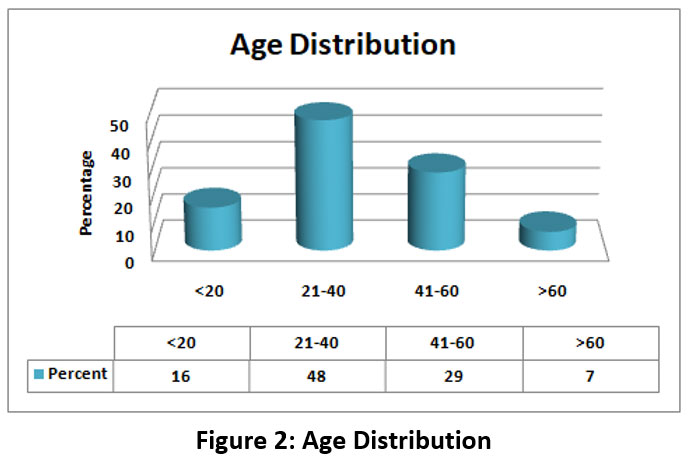 |
Figure 2: Age Distribution |
On classification by mode of injury, Patients sustaining blunt abdominal trauma due to Road traffic accidents formed a major portion at 86 %, followed by fall from height at 8% and assault at 6%.
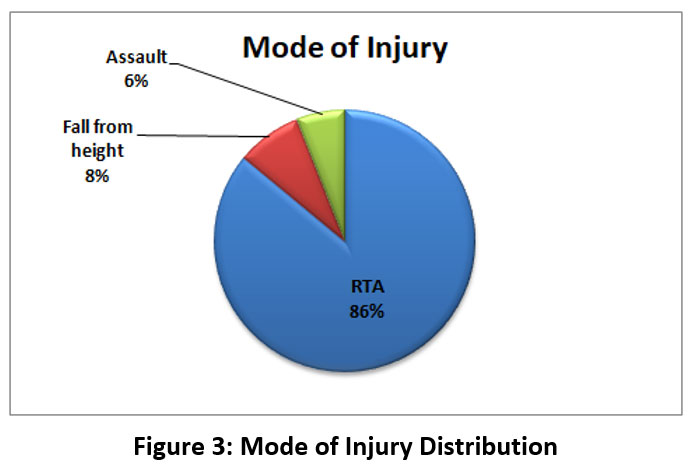 |
Figure 3: Mode of Injury Distribution |
Findings of FAST
A positive FAST scan was detected in 36 % of patients. CECT abdomen done revealed intra-abdominal injury in 41 %. On comparison of FAST with CECT Abdomen as gold standard, FAST had a sensitivity of 87.8 %, Specificity of 100 % and area under Receiver Operating curve ( ROC) of 93.9 %.
 |
Figure 4: Findings of FAST |
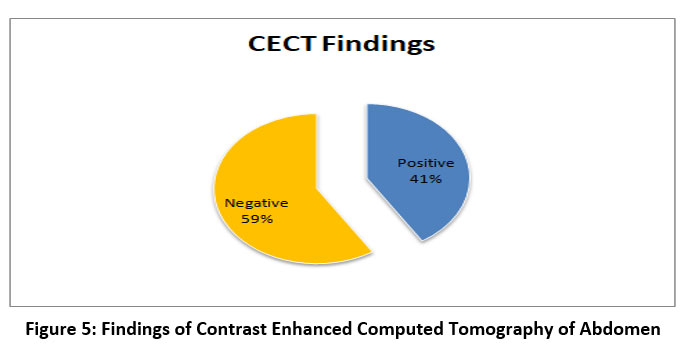 |
Figure 5: Findings of Contrast Enhanced Computed Tomography of Abdomen |
Based on the findings of CECT Abdomen, the organs injured were distributed was as follows:
Table 1: Distribution of observed Organ injuries
| ORGAN | NUMBER OF PATIENTS |
| Splenic injury | 16 |
| Renal injury | 11 |
| Liver injury | 8 |
| Small Bowel injury | 3 |
| Bladder injury | 2 |
| Colon injury | 1 |
| TOTAL | 41 |
On Comparison of FAST and CECT Abdomen Findings:
Table 2: Comparison of FAST and CECT Abdomen.
| FAST | CECT ABDOMEN FINDINGS | |
| Positive for IAI | Negative | |
| Positive | 36 | 0 |
| Negative | 5 | 59 |
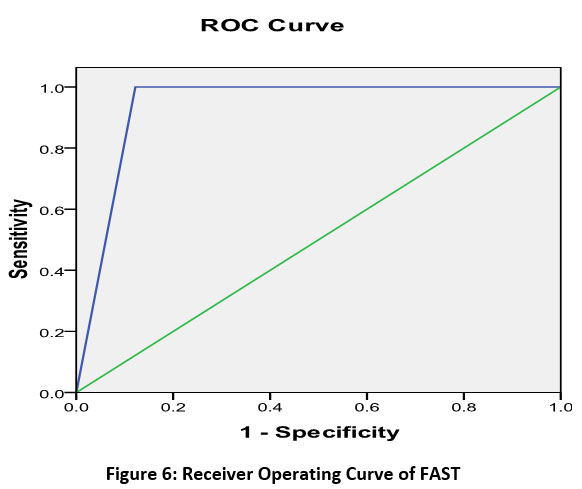 |
Figure 6: Receiver Operating Curve of FAST |
Blunt Abdominal Scoring System (BATSS) Findings
Based on the clinical examination and pre-existing BATSS scoring, patient scores were calculated.
Based on their BATSS scores were classified as (4):
Low risk (score < 8) – 58 %
Intermediate risk (8 -11) – 14 %
High Risk (<11) – 28 %
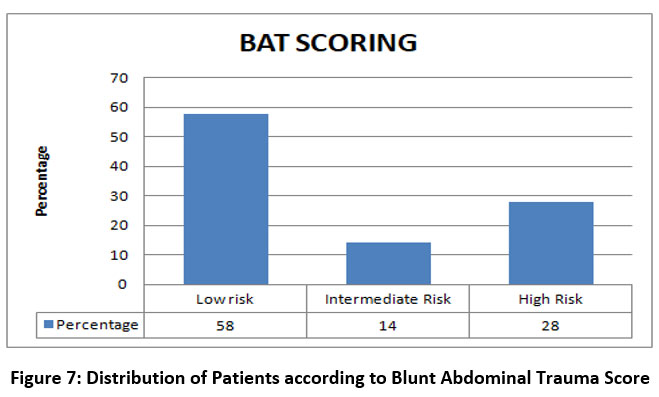 |
Figure 7: Distribution of Patients according to Blunt Abdominal Trauma Score |
On comparison to Contrast Enhanced Computed Tomography of Abdomen, the findings were as follows:
Table 3: Comparison of BATSS with CECT Abdomen
| BATSS | CECT ABDOMEN | |
| POSITIVE FOR IAI | NEGATIVE FOR IAI | |
| LOW RISK | 0 | 58 |
|
INTERMEDIATE RISK |
13 | 1 |
|
HIGH RISK |
28 | 0 |
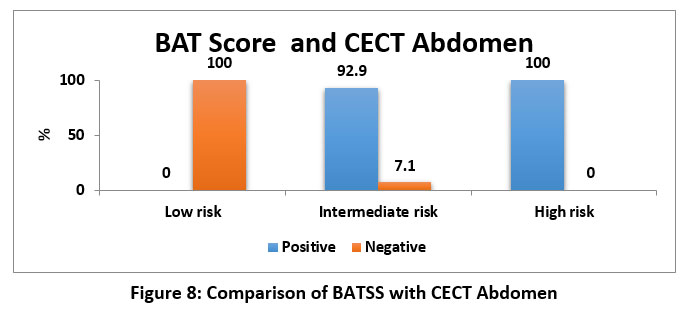 |
Figure 8: Comparison of BATSS with CECT Abdomen |
Intermediate and high risk groups form the majority of cases with intra-abdominal injury, hence were taken as a positive predictor for intra-abdominal injury, based on which the following were calculated.
Sensitivity – 100%, Specificity – 98.3%
Receiver Operating curve (ROC) – Area under curve: 99.2%
 |
Figure 9: Receiver Operating Curve of BATSS |
On Comparison of FAST and BATSS
Table 4: Comparison of FAST and BATSS
| FAST | BAT SCORE | ||
| LOW RISK(<8) | INTERMEDIATE RISK (8-11) | HIGH RISK
(>11) |
|
| POSITIVE | 0 | 8 | 28 |
| NEGATIVE | 58 | 6 | 0 |
It was observed that of the patients included in this study, those with intermediate and high risk BAT score had more probability of a positive FAST scan.
Management
Of the 100 patients, 61 were managed conservatively and 39 cases required surgical intervention in the form of a laparotomy. These were compared to the FAST scan results and their BAT Score.
Table 5: Comparison of FAST and TREATMENT OUTCOMES
| MANAGEMENT | FAST | |
| Positive | Negative | |
| Laparotomy | 34 | 5 |
| Conservative | 2 | 59 |
Table 6: Comparison of BAT Score and TREATMENT OUTCOMES
| MANAGEMENT | BAT SCORE | ||
| LOW RISK(<8) | INTERMEDIATE RISK (8-11) | HIGH RISK
(>11) |
|
| Laparotomy | 1 | 10 | 28 |
| Conservative | 57 | 4 | 0 |
Discussion
The range of patients studied was from 17 to 74 and the mean age of the study group was 35.89 years. The maximum distribution of cases was found between the ages of 21-40 with 48%, followed by 41-60 years at 29% and lesser than 20 years accounting for 16% and those greater than 60 years accounted for 7% of cases. It was observed that cases of ages lesser than 60 accounted for 77% of victims. With 56% of males suffering from BAT, it is observed that majority of the victims are of the young male demographic which translates into maximum Years of Potential Life Lost (YPLL) – a trend seen in developing economies 8.
Trauma sustained as a result of road traffic accidents forms a lion’s share of victims sustaining blunt abdominal trauma followed by accidental fall from height and assault. Making the young male who has sustained blunt trauma to the abdomen due to RTA the typical victim presenting to our casualty room 9.
On admission and resuscitation, FAST was done at point of resuscitation and detected free fluid in 36% of patients. In Hemodynamically stable patients, CECT Abdomen showed that Spleen is the most common organ to be injured 10.
| Splenic injury | 39 % |
| Renal injury | 26.8 % |
| Liver injury | 19.5 % |
| Small bowel injury | 7.31 % |
| Bladder injury | 4.87 % |
| Colon injury | 2.43 % |
BAT Score was calculated with minimum value of 6 and maximum value of 23. The mean was found to be 9.42. On dividing the cases into low risk, intermediate risk and high risk, the mean scores were 6.03, 11 and 15.64 respectively.
The findings of FAST were compared to that of CECT Abdomen in identifying intra-abdominal injury. Sensitivity was found to be around 88%(11), corroborating with published studies, with variation in sensitivity between studies due to the investigation being operator dependent. Specificity was found to be 100%. The positive predictive value and negative predictive values were found to be 100% and 92.2% respectively. On plotting the receiver operating curve (ROC), the area under the curve was calculated at 93.9%, reaffirming that FAST being a good diagnostic investigation for predicting intra-abdominal injury.
The scores of BATSS were analysed, with intermediate and high risk scores being taken as good predictors of intra-abdominal injury. On comparison with CECT abdomen findings, BATSS was found to have a sensitivity of 100%, specificity of 98.3 %, a positive predictive value of 97.6% and a negative predictive value of 100%. On plotting the receiver operating curve (ROC), the area under the curve was calculated at 99.2%, which brings us to the conclusion that BATSS is a better predictor of intra abdominal injury compared to FAST.
Conclusion
The following conclusions can be drawn from our study:
Clinical examination with radiography and ultrasonography form the pillars of assessment of trauma patients on immediate arrival.
The combination of these three has been used to develop this scoring system which gives appropriate weightage to each of the contributing factors, summing up to a 24 point scoring system.
CECT is the current gold standard for the evaluation of patients with Blunt abdominal trauma due to its high sensitivity
The Blunt Abdominal Trauma Scoring System (BATSS) with high sensitivity and specificity comparable to that of CECT, has shown that scores greater than 12 are an extremely high predictor for laparotomy.
A value of 8 or less in BATSS scoring systems are associated with no mortality and no need for laparotomy and no need for further imaging after FAST.
This scoring will help in better triage of the trauma patient on arrival and reduce the need for further imaging and reduce the time interval between arrival and surgical intervention.
With reduction in need for further imaging, it also provides additional benefit by reducing exposure to unnecessary radiation, administration of contrast and reduction in costs, overcrowding of casualty departments and possibility of immediate referral to a tertiary care trauma centre due to inadequate infrastructure to manage a case of blunt abdominal trauma.
This study might offer more perspective on management of blunt abdominal trauma if done as a multi-centre trial. The role of diagnostic laparoscopy may also be included in further studies as there has been significant proliferation of laparoscopic training amongst general surgeons and will extend the scope of this study We conclude by stating that the Blunt Abdominal Scoring System (BATSS) is an excellent predictor of intra-abdominal injury and can be used as a tool by physicians/paramedics in referral/monitoring of high risk patients in a resource limited setting.
Acknowledgement
No funding was received for this study
Conflict of Interest
The authors declare no conflict of interest regarding this study
Funding Source
No funding was obtained
References
- Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J Public Health. 2000 Apr;90(4):523–6.
CrossRef - O’Rourke MC, Landis R, Burns B. Blunt Abdominal Trauma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 [cited 2020 Nov 3]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK431087/
- Radwan MM, Abu-Zidan FM. Focussed Assessment Sonograph Trauma (FAST) and CT scan in blunt abdominal trauma: surgeon’s perspective. Afr Health Sci. 2006 Sep;6(3):187–90.
- Shojaee M, Dolatabadi AA, Sabzghabaei A, Malekirastekenari A, Faridaalaee G, Yousefifard M, et al. New scoring system for intra-abdominal injury diagnosis after blunt trauma. Chin J Traumatol. 2014 Feb 1;17(1):19–24.
- Broder J. Chapter 10 – Imaging Abdominal and Flank Trauma. In: Broder J, editor. Diagnostic Imaging for the Emergency Physician [Internet]. Saint Louis: W.B. Saunders; 2011 [cited 2020 Nov 3]. p. 578–611. Available from: http://www.sciencedirect.com/ science/article/pii/B9781416061137100109
CrossRef - Prasanth J. Prospective study comparing the clinical abdominal scoring system (CASS) with blunt abdominal trauma severity scoring (BATSS) in predicting the necessity of laparotomy in cases admitted with blunt abdominal trauma in GRH, Madurai [Internet] [masters]. Madurai Medical College, Madurai; 2018 [cited 2020 Nov 1]. Available from: http://repository-tnmgrmu.ac.in/9505/
- Caragounis E-C, Xiao Y, Granhed H. Mechanism of injury, injury patterns and associated injuries in patients operated for chest wall trauma. Eur J Trauma Emerg Surg. 2019;ePub(ePub):ePub.
CrossRef - Arumugam S, Al-Hassani A, El-Menyar A, Abdelrahman H, Parchani A, Peralta R, et al. Frequency, causes and pattern of abdominal trauma: A 4-year descriptive analysis. J Emerg Trauma Shock. 2015;8(4):193–8.
CrossRef - N RP, R KKT, G D. Challenges in management of blunt abdominal trauma: a prospective study. Int Surg J. 2018 Sep 25;5(10):3298–304.
CrossRef - Mehta N, Babu S, Venugopal K. An Experience with Blunt Abdominal Trauma: Evaluation, Management and Outcome. Clin Pract [Internet]. 2014 Jun 18 [cited 2020 Nov 3];4(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4202181/
CrossRef - Savatmongkorngul S, Wongwaisayawan S, Kaewlai R. Focused assessment with sonography for trauma: current perspectives. Open Access Emerg Med OAEM. 2017 Jul 26;9:57–62.
CrossRef

