
Manuscript accepted on :28-03-2021
Published online on: 19-05-2021
Plagiarism Check: Yes
Reviewed by: Dr Mahtab Ahmad Khan
Second Review by: Dr. Rupachandra S
Final Approval by: Dr. em. Hans-Joachim Freisleben
Luis Darío-Martínez-Gamez1 , Elva Adelina Ibarra-Valencia2, María Angélica Meza-Ledesma3, Gilberto Flores-Vargas4 , Efraín Navarro-Olivos4, María de Jesús Gallardo-Luna4 and Nicolás Padilla-Raygoza4*
, Elva Adelina Ibarra-Valencia2, María Angélica Meza-Ledesma3, Gilberto Flores-Vargas4 , Efraín Navarro-Olivos4, María de Jesús Gallardo-Luna4 and Nicolás Padilla-Raygoza4*
1Department of Teaching, Community Hospital Apaseo el Alto, General Coordination of Public Health, Institute of Public Health from Guanajuato State. Apaseo el Alto, Mexico.
2Department of Epidemiology,Sanitary Jurisdiction III, General Coordination of Public Health, Institute of Public Health from Guanajuato State. Celaya, México.
3Community Hospital Apaseo el Alto, General Coordination of Public Health, Institute of Public Health from Guanajuato State. Apaseo el Alto, Mexico.
4Department of Research and Technological Development, Directorate of Teaching and Research, Institute of Public Health from Guanajuato State, Guanajuato, Mexico. CP36250.
Corresponding Author E-mail: npadillar@guanajuato.gob.mx
DOI : https://dx.doi.org/10.13005/bpj/2160
Abstract
The first reinfection in the world in Hong Kong, later in Europe (Holland, Belgium) and USA, was documented. In Mexico until November 2020 there are no medical articles that tell us about reinfection; in Celaya Guanajuato the case of a female patient presented with symptoms of COVID-19, 2 polymerase chain reaction in real time tests are performed, in the Laboratory of Public Health from Guanajuato State in an interval of time, less than 5 months; the first in June 2020, with a positive result, received symptomatic treatment and isolation at home for 14 days, negative IgG antibodies test 38 days later; the second time, she presented clinical data on COVID-19 in November From 2020. It was not find references about re-infections by SARS-CoV-2 in Mexico; in Celaya Guanajuato was presented the case of female patient who has symptoms of COVID-19, with new positive PCR, required hospitalization and high-flow oxygen therapy when presenting with pneumonia, was performed simple chest Computing tomography, IgG and IgM antibodies.The evolution was good with discharge from hospitalization 72 hours after admission, continuing his outpatient management until discharge.
Keywords
Polymerase Chain Reaction in Real Time; SARS-CoV-2; Re-infection; antibodies
Download this article as:| Copy the following to cite this article: Martínez-Gamez L. D, Ibarra-Valencia E. A, Meza-Ledesma M. A, Flores-Vargas G, Navarro-Olivos E, Gallardo-Luna M. D. J, Padilla-Raygoza N. Re-Infection by SARS-Cov-2 with in 5 Months: A Case Report. Biomed Pharmacol J 2021;14(2). |
| Copy the following to cite this URL: Martínez-Gamez L. D, Ibarra-Valencia E. A, Meza-Ledesma M. A, Flores-Vargas G, Navarro-Olivos E, Gallardo-Luna M. D. J, Padilla-Raygoza N. Re-Infection by SARS-Cov-2 with in 5 Months: A Case Report. Biomed Pharmacol J 2021;14(2). Available from: https://bit.ly/3ylJdwI |
Introduction
In December 2019, COVID-19 emerged in the city of Wuhan, China, and quickly spread throughout China and the world[1]. On February 27, 2020, the first case of COVID-19 was detected in Mexico, the cases were confirmed by mean of a real-time reverse transcription polymerase chain reaction (rRT-PCR). March 11, 2020 COVID was declared a pandemic [2].
In Mexico there is no publications to date confirming a reinfection by SARS-CoV-2. The first reinfection in the world was documented in Hong Kong, later in Europe (Holland, Belgium) and the USA in the State of Nevada with confirmed rRT-PCR and without immune disorders, 48 days after the first infection [3,4].
In a study of 111 recovered patients, 5% in China and 10% South Korea tested positive again, there is evidence that a COVID-19 reinfection is not possible within 7-10 days. China conducted a study in primates where it observed that there is no viral replication before 5 days after reinfection, indicating that the primary infection of SARS-CoV-2 could prevent subsequent infections [5]. On April 13, South Korea reported 116 positive COVID-19 cases for the second time [6].
Viral load has been shown to be high in most patients from the onset or even before the onset of symptoms, peaking after 3 to 5 days, then beginning to decrease significantly around the day. 10, to drop to undetectable levels around day 21, seroconversion (IgM and IgG) occurs in the first 7 days after symptoms onset in 40% to 50% of patients, and by day 15 in almost 100 % of them, although the results show great variability in terms of the moment of appearance of the antibodies[7].
The World Health Organization (WHO) defines reinfection as the process through which a person was once infected with SARS-CoV-2, stopped being infected, and is re-infected with SARS-CoV-2 [8].
Presentation of the case
48-year-old female, technical profession in social work, with class II obesity (body mass index 39), on June 13, 2020 she presented suddenly, cough, headache, diarrhea, chest pain and odynophagia. The oxygen saturation 92% with pulse oximetry; rRT- PCR through nasopharyngeal swab on June 17, 2020, with positive result for SARS-CoV-2, chest radiography without alterations (Figure 1); it was indicated, ambulatory treatment in home, paracetamol 500 mg every 8 hours, isolation for 14 days. Later he returned to his work without any complications. On July 21, 2020, a negative IgG antibody (0.7), negative IgM (0.3) antibody was measured.38 days after documenting the infection, she was given an influenza vaccine on September 20, 2020.November 6, 2020, five months after having presented COVID-19, she went to the Apaseo el Alto Community Hospital to the COVID Emergency Service where she was evaluated in TRIAGE, she presented anorexia, anosmia, dysgeusia, dyspnea on medium efforts, mild-moderate respiratory distress, with 5 days of evolution, hypoxia, oxygen saturation of 86%, improved to 92% with a 10-liter reservoir bag mask. alternating with non-invasive mechanical ventilation (NIV) continuous positive airway pressure (CPAP) mode with positive pressure at the end of expiration (PEEP) 10 cmH2O, fraction of inspired oxygen (FiO2) at 90% intermittently (every 8 hours for 2 hours), pharmacological treatment, clarithromycin 500 mg orally every 12 hours, Enoxaparin 60 mg subcutaneously every 24 hours, omeprazole 40 mg intravenously every 24 hours.
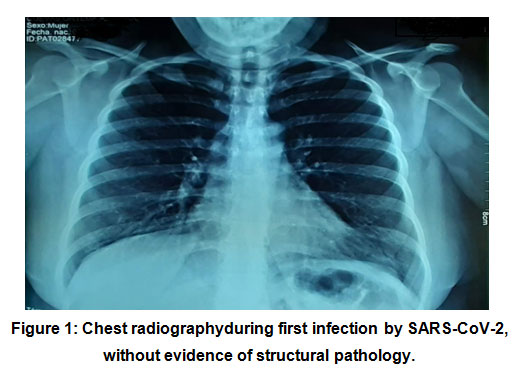 |
Figure 1: Chest radiographyduring first infection by SARS-CoV-2, with out evidence of structural pathology. |
Classification National Early Warning Score (NEWS 2): 4 points. Relationship index between arterial oxygen pressure and inspired oxygen fraction (PaO2 / FIO2): 193, immunoglobulin: positive IgG (22.0), positive IgM (1.0), high C-reactive protein (89.50), chest film (Figure 2) and simple computed chest tomography (Figure 3), a PCR test for SARS-CoV-2 was performed again, with nasopharyngeal swab, it was sent to the State Laboratory of Public Health of the State of Guanajuato, the result was positive for the second time with a cycle threshold (TC) of: 21, his discharge was decided due to clinical improvement 72 hours after admission, he required home oxygen, through nasal tips 3-5 liters for 15 days, he progressed to clinical improvement, oxygen was suspended and an open appointment was given to the emergency room 24 hours a day.
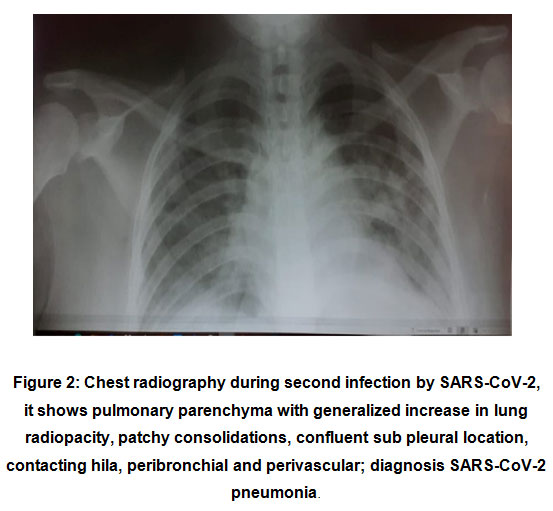 |
Figure 2: Chest radiography during second infection by SARS-CoV-2, it shows pulmonary parenchyma with generalized increase in lung radiopacity, patchy consolidations, confluent sub pleural location, contacting hila, peribronchial and perivascular; diagnosis SARS-CoV-2 pneumonia.. |
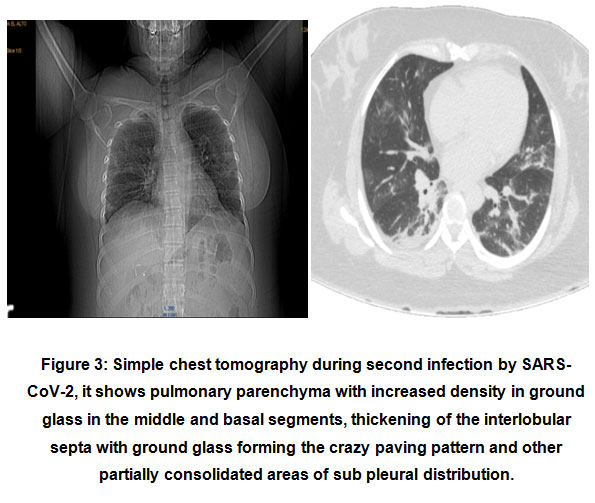 |
Figure 3: Simple chest tomography during second infection by SARS-CoV-2, it shows pulmonary parenchyma with increased density in ground glass in the middle and basal segments, thickening of the interlobular septa with ground glass forming the crazy paving pattern and other partially consolidated areas of sub pleural distribution. |
Discussion and review of literature
The patient presented 2 positive rRT-PCR tests for SARS-CoV-2, in a scenario of sustained generalized community transmission. In the case of a patient with a clinical picture of acute respiratory infection, in addition, a risk group for being health personnel, with no history of having generated immunity in the first documented infection, and given the scarce information about the generation of immunity in COVID-19 cases, it is evident that there are high possibilities that it is a reinfection when presenting clinical symptoms of COVID-19 and through the use rRT-PCR positive, which is the gold standard diagnostic method [9].
It recommends that patients with clinical suspicion of COVID-19, undergo a simple chest CT scan, specific nucleic acids by RT-PCR, and IgG and IgM antibodies to SARS-CoV-2 [10].
Antibody levels are highly dependent on time after exposure; it should to determine the level and specificity of the antibody against the specific protein at the time of reinfection. It is possible that the infection may not confer lasting immunity in some patients [11]. IgG and IgM are produced in the second week of infection [12,13].
In this case, 5 months after the first infection, a rRT- PCR test was performed for the second time with a positive result, positive IgG, positive IgM, which means that the patient has an acute but more advanced infection [14].
To et al. [15], reported that 14 days after the onset of symptoms, 94% of the patients had IgG antibodies against the NP protein and 88% had IgM antibodies against the same protein. Additionally, 100% of the patients had IgG antibodies against protein S and 94% had IgM antibodies against said protein. The researchers tried to study any possible correlation between antibody levels and the severity of the disease, however, no correlation was found.
The collection and storage of adequate samples from COVID-19 cases is a key point to ensure confirmation of reinfection. Only through the existence of at least two samples, can reinfection be confirmed.
The duration of immune protection against reinfection by SARS-CoV-2 in patients who have recovered from COVID-19 is a critical question unanswered to date [16].
Conclusion
The evidence to date suggests that this is a rare event. More studies are needed to determine the incidence of reinfection in the population in Mexico.
There is currently no solid evidence regarding confirmed cases of COVID-19 reinfection. There are publications worldwide that speak of cases, however, it is not clear if these cases are real reinfections or a reactivation of SARS-CoV-2, which had not been completely eliminated from the body.
The patient presented 2 positive rRT-PCR tests and clinical data of COVID-19 on both occasions, there is evidence that the patient did not present symptoms of primary infection by SARS-CoV-2 for more than 5 months.
We do not have the complete genomic sequencing of SARS-CoV-2, which indicates whether it is caused by different viral lineages, the question remains because the first test was not stored.
Consent to Publish
It was obtained the consent to publish clinical data and images from the patient.
Conflict of Interest
The authors declare no conflict of interest.
Funding Source
There is not any funding for this case report.
References
- Guan W, Ni Z, Hu Y,Liang W, Ou C, He J, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020; 382: 1708-1720. Doi: https://dx.doi.org/10.1056/NEJMoa2002032
CrossRef - Suarez V, Suarez-Quezada M,Oros-Ruiz S, Ronquillo de Jesús E. Epidemiologia de COVID-19 en México: del 27 de febrero al 30 de abril de 2020.Rev Clin Esp. 2020; 2020(8): 463-471. Doi: https://dx.doi.org/10.1016/j.rce.2020.05.007
CrossRef - wasaki A. What reinfections mean for COVID-19. Lancet Infect Dis. 2021; 21(1):3-5. Doi: https://dx.doi.org/10.1016/S1473-3099(20)30783-0.
CrossRef - Tillet RL, Sevinsky JR, Hartley PD, Kerwin H, Crawford N, Gorzalski A, et al. What reinfections mean for COVID-19. The Lancet Infectious Diseases. 2020; 21(1):52-58. Doi: https://doi.org/10.1016/S1473-3099(20)30764-7
CrossRef - Law SK, Albert WN Leung AWN, C Xu C. Is reinfection possible after recovery from COVID-19?.Hong Kong Med J. 2020; 26: 264-265. Doi: https://dx.doi.org/10.12809/hkmj208601
CrossRef - Alizargar Riesgo de reactivación o reinfección del nuevo coronavirus (COVID-19). J Formos Med Assoc. 2020; 119(6):1123. Doi: https://dx.doi.org/10.1016/j.jfma.2020.04.013
CrossRef - Díaz-Castrillón FJ, Toro-Montoya AI. SARS-CoV-2/COVID-19: The virus, the disease and the pandemicMedicina&Laboratorio 2020;24:183-205.Available in: https://docs.bvsalud.org/biblioref/2020/05/1096519/covid-19.pdf
CrossRef - Organización Panamericana de la Salud, Organización Mundial de la Salud. Orientaciones provisionales para la detección de casos de reinfección por SARS-CoV-2. Available in: https://www.paho.org/es/documentos/orientaciones-provisionales-para-deteccion-casos-reinfeccion-por-sars-cov-2.
- Karam M, Althuwaikh S, Alazemi M, Abul A, Hayre A, Barlow G, et al. Chest CT versus RT-PCR for the Detection of COVID-19: Systematic Review and Meta-analysis. medRxiv. 06.22.20136846 https://doi.org/10.1101/2020.06.22.20136846
CrossRef - Hernández‐Huerta MT, Pérez‐Campos Mayoral L, Sánchez- Navarro LM, Mayoral‐Andrade G, Pérez‐Campos Mayoral E, Zenteno E, et al. Should RT‐PCR be considered a gold standard in the diagnosis of COVID‐19?. J Med Virol. 2020. Doi: J Med Virol. 2020. Doi: https://dx.doi.org/10.1002/jmv.26228.
CrossRef - Stephens DS, McElrath MJ. COVID-19 and the Path to Immunity. 2020;324(13):1279-1281. Doi:https://dx.doi.org/ 10.1001/ jama.2020.16656
CrossRef - Cajamarca-Baron J, et al. SARS-CoV-2 (COVID-19) en pacientes con algún grado de inmunosupresión. Reumatol Clin. 2020.
CrossRef - Duggan NM, Ludy SM, Shannon BC, Reisner AT, Wilcox SR. Is novel coronavirus 2019 reinfection possible? Interpreting dynamic SARS-CoV-2 test results through a case report. Am J EmergMed. 2021; 39: 256.e1–256.e3.Doi_ https://dx.doi.org/ 10.1016/ j.ajem.2020.06.079
CrossRef - Morales- OlveraM. ¿Cómo descarto el diagnostico de COVID-19 en un paciente que se someterá a cirugía electiva? Recomendaciones de seguridad en cirugías que se realicen durante la pandemia de COVID-19. Medicina basada en evidencia. Cirugía plástica 2020; 30 (1): 22-32.Available in: https://www.medigraphic.com/pdfs/cplast/cp-2020/cp201c.pdf
CrossRef - To KKW, Tsang OTY, Leung WS, Tam AR, Wu TC,Lung DC et al. Temporal profiles of viral load inposterior oropharyngeal saliva samples and serum2antibody responses during infection by SARS-CoV-2:an observational cohort study. The Lancet InfectiousDiseases. 2020; 20:565-574. Doi: https://dx.doi.org/10.1016/S1473-3099(20)30196-1
CrossRef - Zhang K., Johnson Yiu-Nam Lau JYN, Yang L,Ma ZG. SARS-CoV-2 reinfection in two patients who have recovered from COVID-19. PrecisionClinical Medicine. 2020; 3(4): 292-293. Doi: https://doi.org/10.1093/pcmedi/pbaa031
CrossRef

