
Skanda Ragi* and Pramod Shah
Department of Radiology, Krishna Institute of Medical Sciences, Karad, Maharashtra-415117.
Corresponding Author E-mail: skandaprasad9999@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2021
Abstract
In the past few years, advancements in computed tomography (CT) technology have changed the trend of imaging techniques used in the evaluation of the urinary system. However, the accuracy is main concern for detecting urinary calculi. To compare unenhanced multi-detector computed tomography (MDCT) with ultrasonography (USG) for accurate diagnosis of urinary calculi. This cross-sectional study was conducted from June 2018 to May 2019 by involving 80 non-consecutive patients, who underwent unenhanced MDCT and USG for the diagnosis of urinary calculi. Diagnostic accuracy of MDCT and USG were measured by calculating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). SPSS software Ver. 21.0 was used to perform statistical analysis. In the present study male to female ratio was 3.2:1 and the mean age was 37.1±16.01 years and 41.2±14.16 years, respectively. Flank pain was the commonest complaint recorded in 81.25% of patients. In both modalities, renal calculi were detected in 90% of the patients and in majority of patients (21.25%), stones were found in vesicoureteric junction and in 16.25 % it was found upper junction of the ureter. Further, in most of the patient’s calculi were detected bilaterally (41.25%), while in 31.25% and 27.5% patients, calculi were detected in left and right ureter, respectively. The sensitivity and specificity of MDCT in diagnosing ureteric calculi was 100% and 57.14%, respectively. The sensitivity of USG was 8.33% with 100% specificity. Hence, MDCT showed more sensitivity than USG in diagnosing urinary calculi. MDCT helps in accurate diagnosis of urinary calculi compared to USG.
Keywords
Flank pain; Urinary Calculi; Ureteral Calculi; Tomography; Ultrasonography
Download this article as:| Copy the following to cite this article: Ragi S, Shah P. Role of Unenhanced Multi-Detector Computed Tomography in Detection of Urinary Calculi in Comparison with Ultrasonography. Biomed Pharmacol J 2020;13(3). |
| Copy the following to cite this URL: Ragi S, Shah P. Role of Unenhanced Multi-Detector Computed Tomography in Detection of Urinary Calculi in Comparison with Ultrasonography. Biomed Pharmacol J 2020;13(3). Available from: https://bit.ly/36ya11o |
Introduction
Urinary calculi are solid deposits found in the urinary tract from minerals dissolved in the urine.1 Calculi located in the kidneys, ureters, urinary bladder or urethra and are one of the major diseases that have affected people since ancient times.2 The prevalence of urinary tract calculi is found to be greater in males (15%) than in females (8%) with a global annual incidence of 131 per 100,000.3,4 Longstanding kidney stones may cause obstruction and infection, which can ultimately lead to renal failure.5 Hence, early accurate diagnosis of urolithiasis with appropriate treatment is pivotal for preventing complications and renal failure.6
In the last few years, several imaging techniques, particularly, X-Rays, USG, Intravenous Pyelography (IVP), Computed Tomography (CT), and Magnetic Resonance Imaging (MRI) were used to diagnose urinary calculi in the renal tract. The most recent breakthrough in renal calculi imaging is an emergence of unenhanced multi-detector computed tomography (MDCT) and its use in ureteral and renal stone detection.7 MDCT is the method of choice in assessment of urinary calculi due to its shorter examination time, safety and accuracy.8 Patients with acute flank pain are typically diagnosed using intravenous urography (IVU) as the standard screening tool for identifying urinary calculi. However, intravenous contrast medium is required in IVU which is associated with potential risks.9 Such concerns have led to the use of other methods such as the combination of plain abdominal X-ray and Ultrasonography (USG) and more recently MDCT.
MDCT produces thin collimated data of the urinary tract in a single breath hold and generates higher spatial resolution compared to single detector CT.10 The capacity to provide reconstructions in the coronal, sagittal and oblique planes make it accurate in localization of calculi and different pathologies of the urinary tract. It provides accurate anatomical details of vital structures, providing valuable data for management decisions.11
From past three decades, USG is widely used for detecting urinary calculi, as it is non-invasive, and cheap method and it is the modality of choice for calculi detection under circumstances such as pregnancy and paediatric age group patients and it can detect stones located in pyeloureteric and vesicoureteric junctions (VUJ); however, it has limited diagnostic value in assessing urinary calculi, as it does not detect stones that are <5 mm in diameter, which may remain unrecognised due to a partial volume effect or the absence of posterior shadowing.12 The detection of ureteral stones in mid ureter is not easily identified by USG, particularly in bowel interposition or in obese patients. Hence, the present study was undertaken to assess the accuracy of MDCT in comparison with USG for accurate diagnosis of urinary calculi.
Methodology
Study design
This cross-sectional study was conducted in the Department of Radiodiagnosis in a private hospital from June 2018 to May 2019 at Karad, Maharashtra. Ethical approval from the institutional ethical committee and the informed consent from all patients was obtained prior to the initiation of the study. At 95% confidence interval and 80% statistical power, the sample size required was found to be minimum of 21 patients, to fulfil the primary objective. During the study period, 80 cases were diagnosed in the Radiology department and were included in the study to improve statistical reliability.
Selection criteria
A total of 80 non-consecutive patients belonging to all ages and both sexes admitted into the various clinical departments who had presented with suspected urolithiasis by clinical signs and symptoms (flank pain and hematuria), who underwent unenhanced MDCT and USG for the diagnosis of urinary calculi. were considered for the study. Post-operative cases, extra renal masses invading the kidney and pregnant woman were excluded from this study.
Data collection
A structured proforma was used to collect the demographic data such as age, gender, past history and complaints on admission. The findings of MDCT and USG such as location, site and other findings were also recorded.
Procedure
In this study, the unenhanced MDCT imaging was performed using CT machine Siemens Emotion system 16 slice MDCT and the ultrasonogram was performed with Ultrasonography Siemens Acuson x 300.3.5 Mhz frequency Transducer.
During, scanning procedure, patients were asked to drink one to one and half litres of water one hour prior to the scan so that their urinary bladder would be full at the time of the scan. The topogram or scout radiograph was obtained at 120kv and 40mAs with a collimation of 1 mm. The field of view of unenhanced computerized tomography was then plotted from the level of diaphragm to the base of the urinary bladder i.e., at the level of the pubic symphysis. The scan was carried out at 120kv and 130mAs with a slice thickness of 5.0 mm at the collimation of 2.5 mm. No oral or intravenous contrast was administered during the study. The entire scan took a total of 10 to 15 seconds and was carried out in a single breath hold. The images are later reformatted at the thickness of 1.5 mm, to facilitate detection of small calculi, which were invariably undetected by another imaging modality. Further these patients were subjected to USG abdomen examination.
For MDCT procedure, patients were placed in a supine position and in a single breath hold, scanning from the level of suprarenal glands to the infravesical level was performed. All patients were nil by mouth to avoid bowel gas artifacts.
Statistical analysis
Data were coded and tabulated on Microsoft Office Excel Spreadsheet and analysis were done using SPSS version 21. Diagnostic accuracy of USG was measured by calculating sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV). The correlation of the MDCT and USG diagnosis was identified using Cohen’s kappa coefficient (κ). A p-value of <0.05 was considered statistically significant.
Results
Among the 80 patients enrolled in the study, 76.25% were males and 23.75% were females with mean age of 37.1±16.01 years and 41.2±14.16 years respectively. The patients presented with clinical signs and symptoms are given in the Table 1. The most common symptoms were observed to be flank pain (81.25%) and backache (51.25%) in most patients.
Table 1: Clinical signs and symptoms
| Complaints | Number | Percentage |
| Flank pain | 65 | 81.25 |
| Backache | 41 | 51.25 |
| Burning micturation | 31 | 38.75 |
| Headache | 26 | 32.50 |
| Hematuria | 23 | 28.75 |
| Fever | 8 | 10.00 |
Both MDCT and USG scans identified renal stones in most patients (90%). With respect to the location of the calculus in ureter, in both modalities in majority of patient’s (21.5%) calculi were found in VUJ followed by calculi in upper, mid and lower ureter. Further, in most of the patients, stones were detected bilaterally (41.25%), while in 31.25% calculus were detected in left side and in 27.5% of the patients calculus were detected in right side ureter. In MDCT scanning, presence of hydronephrosis was noted in 67.5% of patients and hydroureter in 65% of the patients. However, there was one case of perinephric fat stranding found in the MDCT scan (Table 2).
Further, the ultrasound findings revealed hydronephrosis in 72.5% of patients and hydroureter in 72.5% of patients. However, 11 (13.75%) cases of renal mid ureteric calculus with hydronephrosis and hydroureter, 13 (16.25%) cases of renal, upper ureteric calculus with hydronephrosis and hydroureter and 12 (15%) cases of renal and lower ureteric calculus with hydronephrosis and hydroureter could not be diagnosed on ultrasound and only renal calculus was seen on USG (Table 2).
Table 2: MDCT and USG scan findings-Location
| Location | MDCT (n=80) (%) | USG (n=80) (%) |
| Renal | 72 (90) | 72 (90) |
| Pelviureteric junction | 9 (11.25) | 10 (12.5) |
| Upper ureter | 13 (16.25) | 3 (3.75) |
| Mid ureter | 11 (13.75) | 0 |
| Lower ureter | 12 (15) | 0 |
| VUJ | 17 (21.25) | 17 (21.25) |
| Vesical | 5 (6.25) | 5 (6.25) |
VUJ: Vesicoureteric Junction; MDCT: Multi-detector Computed Tomography; USG: Ultrasonography
There are eight diagnosis that are mentioned below. The numbers in the bold are the diagnoses identified and confirmed by the MDCT and USG scan. USG was unable to identify the calculi in upper, mid and lower ureter with hydronephrosis and hydroureter (diagnosis “f”, “g”, “h”) and detected only renal calculi (diagnosis “c”). Whereas, MDCT could accurately locate the calculi in ureter. The correlation of the MDCT and USG diagnosis was using Cohen’s kappa coefficient (κ). The degree of agreement between MDCT and USG was determined using Cohen’s kappa coefficient test. The kappa value was 0.52 (95 % CI) which indicates that there was good agreement between MDCT and USG findings; values between 0.40 and 0.75 indicate fair to good agreement. MDCT findings were found to be reliable in detecting urinary calculi and well matched with the USG.
Table 3: Distribution of diagnosis based on MDCT and USG findings
| MDCT Findingsa | USG Findings | Total | |||||||
| a | b | c | d | e | f | g | h | ||
| a | 5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 |
| b | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| c | 0 | 0 | 13 | 0 | 0 | 0 | 0 | 0 | 13 |
| d | 0 | 0 | 0 | 14 | 0 | 0 | 0 | 0 | 14 |
| e | 0 | 0 | 0 | 0 | 9 | 0 | 0 | 0 | 9 |
| f | 0 | 0 | 11 | 0 | 0 | 0 | 0 | 0 | 11 |
| g | 0 | 0 | 10 | 0 | 0 | 0 | 3 | 0 | 13 |
| h | 0 | 0 | 12 | 0 | 0 | 0 | 0 | 0 | 12 |
| Total | 7 | 1 | 46 | 14 | 9 | 0 | 3 | 0 | 80 |
MDCT: Multi-detector Computed Tomography; USG: Ultrasonography; a: Vesical calculus; b:
There were 45 cases of same disease identified by both MDCT and USG scans and 35 cases of different diseases detected by the two scans. However, there was no statistical significance between the detection of disease and the findings of MDCT and USG scans (P=0.2684).
By taking the diagnosis of ureteric calculi, the sensitivity and specificity of USG in comparison to MDCT was found to be low (Table 4).
Table 4: Accuracy of USG in comparison to MDCT for the diagnosis of ureteric calculi
|
Variables |
MDCT | Sensitivity
(%) |
Specificity
(%) |
PPV
(%) |
NPV
(%) |
||
| Positive | Negative | ||||||
|
USG |
Positive | 3 | 0 | 8.33 | 100 | 100 | 57.14 |
| Negative | 33 | 44 | |||||
MDCT: Multi-detector Computed Tomography; USG: Ultrasonography; PPV: Positive predictive value; NPV: Negative predictive value
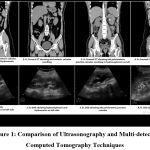 |
Figure 1: Comparison of Ultrasonography and multi-detector computed tomography techniques |
Discussion
Radiological diagnostic tools play an important role in the differential diagnosis of flank pain and renal calcifications. There is a need for a highly sensitive and non-nephrotoxic means of instantly identifying calculi. USG is inexpensive, does not expose patients to ionizing radiation and can be performed at patient’s bedside. However, it has highly variable sensitivity for detecting urinary calculi as reported by previous literature.13-15 Hence, the present study was undertaken to assess the accuracy of MDCT in comparison with USG for accurate diagnosis of urinary calculi.
In the present study most patients were in their 30s and 40s, this supports the observations reported in previous reports that urinary calculi are most common in middle-aged people with a peak onset in the fourth decade of life.16 On analysing the distribution of gender of the patients, it was observed that there was male predominance over female. This is consistent with previous literature reporting urinary calculi are more common in men.3,4,17 In this study, flank pain was the most common complaint from majority of the patients, as flank pain is the primary sign of ureteric stone.18
In the current study, USG was not sensitive in detecting ureteric calculi compared to MDCT. Of the 36 cases with ureteric calculi, 3 cases were seen on USG. Unlike MDCT, USG could not detect the calculi in upper, mid and lower ureter with hydronephrosis and hydroureter and could identify only renal calculi. The sensitivity of USG found in this study was substantially low compared to other studies such as Ather et al. reported 81% and Passerotti et al. reported 76%.19,20 The poor sensitivity and inaccuracy of USG could be due to lack of acoustic shadowing of ureteric calculi, which could have missed the detection of calculi in ureters. Other factors like selection of the focal length or transducer power could influence the accuracy of USG.21 The sensitivity value of USG reported in the previous studies show a varying range of 12% to 93% sensitivity of detecting ureteric calculi.13-15 Fowler et al. revealed that USG is a poor diagnostic tool for identifying stones smaller than 4.0mm.22
Using the Cohen’s kappa coefficient test, we found good agreement between the findings of MDCT and USG. This is in agreement with Ulusan et al who reported a kappa value of 0.590.23 The diagnostic accuracy of MDCT is said to be 99% of stones, including the radiolucent stones on plain film radiography can be detected.24 The detection of urinary calculi by MDCT was found to be more effective than USG. Although, USG is not accurate compared to MDCT, it is readily available, non-invasive, safe and effective when MDCT scan is not available or cannot be performed. Overall, the present study showed that MDCT is more accurate in comparison with ultrasonography for the diagnosis of urinary calculi.
The limitation in the study was that time interval between USG and MDCT scans were not specified. This could affect the accuracy of the scan as the calculi might have moved or changed in size during the time interval. The chemical composition of the calculi was not considered in the study.
Conclusion
The efficiency of MDCT for the detection of urinary calculi is greater than USG. Further studies are needed for comparison of the diagnostic accuracy of MDCT in cases of urinary calculi”.
Acknowledgment
None
Funding source
The authors declare there is no funding source.
Conflict of interest
There is no conflict of interest.
References
- Rule AD, Lieske JC, Pais VM. Management of Kidney Stones in 2020. JAMA. 2020;323(19):1961–2.
- Leonardo FF, Thiago DS. Kidney Stones: Treatment and Prevention. Am Fam Physician. 2019;99(8):490-6.
- Lee M-C, Bariol SV. Epidemiology of stone disease in Australia. In: Talati JJ, Tiselius HG, Albala DM, YE Z, editors. Urolithiasis: Basic science and clinical practice. London: Springer London, 2012; p. 73-6
- Romero V, Akpinar H, Assimos DG. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev Urol. 2010;12(2-3):e86-96.
- Gambaro G, Favaro S, D’Angelo A. Risk for renal failure in nephrolithiasis. Am. J. Kidney Dis. 2001; 37: 233-43
- Soomro HU, Hammad Ather M, Salam B. Comparison of ureteric stone size, on bone window versus standard soft-tissue window settings, on multi-detector non-contrast computed tomography. Arab J Urol. 2016;14(3):198-202.
- Older AR, Jenkins AD: Stone disease. Urol Clin North Am 2000;27(2):215-29.
- Fielding JR, Silverman SG, Rubin GD: Helical CT of urinary tract: Am J Roentgenol 1999;172:1199-1206.
- Gavant ML. Low-osmolar contrast media in the 1990s. Guidelines for urography in a cost-sensitive environment. Invest Radiol 1993;28(Suppl. 5):S13-9.
- Dawson P, Lees WR. Multislice technology in computed tomography. Clin Radiol 2001;56:302-9.
- Eshed I, Witzling M. The role of unenhanced helical CT in the evaluation of suspected renal colic and atypical abdominal pain in children. Pediatric Radiology. 2002;32(3):205-8.
- McLaughlin PD, Murphy KP, Hayes SA, Carey K, Sammon J, Crush L, et al. Non-contrast CT at a comparable dose to an abdominal radiograph in patients with acute renal colic; the impact of iterative reconstruction on image quality and diagnostic performance. Insights into imaging. 2014;5(2):217-30.
- Patlas M, Farkas A, Fisher D, Zaghal I, Hadas-Halpern I. Ultrasound vs CT for the detection of ureteric stones in patients with renal colic. Br J Radiol 2001;74:901-4.
- Sommer FG, Jeffrey RB Jr, Rubin GD, et al. Detection of ureteral calculi in patients with suspected renal colic: value of reformatted noncontrast helical CT. AJR Am J Roentgenol 1995;165:509–13.
- Catalano O, Nunziata A, Altei F, Siani A. Suspected ureteral colic: primary helical CT versus selective helical CT after unenhanced radiography and sonography. AJR Am J Roentgenol 2002;178:379–87.
- Romans L. Urinary tract calculi. Available from: URL: http://www.cewebsource.com/coursePDFs/CTurinaryTract.pdf [Access Date: 28.01.2020]
- Portis AJ, Sundaram CP. Diagnosis and initial management of kidney stones. Am Fam Physician. 2001;63:1329-38.
- Smith RC, Rosenfield AT, Choe KA, Essenmacher KR, Verga M, Glickman MG, et al. Acute flank pain: comparison of non-contrast-enhanced CT and intravenous urography. Radiology. 1995;194(3):789-94.
- Ather MH, Jafri AH, Sulaiman MN. Diagnostic accuracy of ultrasonography compared to unenhanced CT for stone and obstruction in patients with renal failure. BMC Med Imaging. 2004; 4(1): 2.
- Passerotti C, Chow JS, Silva A, et al. Ultrasound versus computerized tomography for evaluating urolithiasis. J Urol. 2009; 182(4 Suppl): 182934.
- King W, 3rd, Kimme-Smith C, Winter J. Renal stone shadowing: an investigation of contributing factors. Radiology. 1985; 154(1): 191-6.
- Fowler KA, Locken JA, Duchesne JH, Williamson MR. US for detecting renal calculi with nonenhanced CT as a reference standard. Radiology. 2002;222(1):109-13.
- Ulusan S, Koc Z, Tokmak N. Accuracy of sonography for detecting renal stone: comparison with CT. J Clin Ultrasound. 2007 Jun;35(5):256-61.
- Romans L. Abdomen and pelvis imaging procedures. In: Pete Sabatini, eds. Computed Tomography for Technologists: Exam Review. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2018. p.127

