
Nicolas Padilla-Raygoza1* , Cuauhtémoc Sandoval-Salazar2, Luis Antonio Diaz-Becerril1, Daniel Alberto Díaz-Martínez3, Efrain Navarro-Olivas3, Maria de Jesús Gallardo –Luna3and Francisco J. Magos-Vazquez3
, Cuauhtémoc Sandoval-Salazar2, Luis Antonio Diaz-Becerril1, Daniel Alberto Díaz-Martínez3, Efrain Navarro-Olivas3, Maria de Jesús Gallardo –Luna3and Francisco J. Magos-Vazquez3
1School of Medicine, University of Celaya, Mexico 38080
2Department of Nursing and Obstetrics, Division of Health Sciences and Engineering, Campus Celaya-Salvatierra, University of Guanajuato, México Orcid ID: 0000-0001-9918-405
3Secretary of Health form Guanajuato State, Mexico 36000
Corresponding Author E-mail : npadilla@udec.edu.mx
DOI : https://dx.doi.org/10.13005/bpj/2004
Abstract
The aim was to describe the number of confirmed cases of COVID-19 in Mexico until April 16, 2020. The study design was an ecological descriptive study. The place and duration of study were registries of confirmed cases for COVID-19 in Mexican population during February and until April 16, 2020, 13:00 PM, from National System of Epidemiological Surveillance/ General Direction of Epidemiology/ Secretary of Health, Mexico. Material and methods: Accord to database of confirmed cases of COVID-19 by Secretary of Health in Mexico, it was collected data on age, gender, it was included 6,297 registries. Results: The first confirmed case in Mexico was February 20, 2020 and the frequency are arising at the end of February and throughout March. The early confirmed cases were imported cases for travel to USA, Italy, Germany, Spain, France and Singapore. No one travelled to China. Now, there are a lot of confirmed cases infected for contact with a case. Conclusion: The frequency of confirmed cases of COVID-19 are higher and the health authorities in Mexico are waiting that the peak of the epidemiological curve is in early May.
Keywords
COVID-19; Infection; Population; SARS-CoV-2
Download this article as:| Copy the following to cite this article: Raygoza N. P, Salazar C. S, Becerril L. A. D, Martínez D. A. D, Olivas E. N, Luna M. de J G, Vazquez F. J. M. Evolution of COVID-19 Infection in Mexico until April 16, 2020: A Descriptive Ecological Study. Biomed Pharmacol J 2020;13(3). |
| Copy the following to cite this URL: Raygoza N. P, Salazar C. S, Becerril L. A. D, Martínez D. A. D, Olivas E. N, Luna M. de J G, Vazquez F. J. M. Evolution of COVID-19 Infection in Mexico until April 16, 2020: A Descriptive Ecological Study. Biomed Pharmacol J 2020;13(3). Available from: https://bit.ly/3adSZW5 |
Introduction
On December 31, 2019, a case of pneumonia occurred in Wuhan, China, and it was reported at the office of the World Health Organization (WHO) in China; due to the increase in cases, in one month, the WHO declared a Public Health emergency of international interest on January 30, 2020.1
SARS-CoV-2 is a new coronavirus that has not been identified in humans and the infection can be asymptomatic or manifest as a disease with a clinical data, 2 to 14 days after exposure, manifests with fever, dry cough, respiratory distress, and some cases diarrhoea and vomiting.2
Coronaviruses belong to the Coronaviridae family in the Nidovirales order. Corona represents crown-like spikes on the outer surface of the virus; thus, it was named as a coronavirus. Coronaviruses are minute in size (65–125 nm in diameter) and contain a single-stranded RNA as a nucleic material, size ranging from 26 to 32kbs in length.3
The zoonotic origin of SARS-CoV-2 has not been confirmed, however sequential analysis suggests bats as their reservoir; DNA recombination was found to be involved in the spine glycoprotein which classifies SARS-CoV, thus being the reason for cross-transmission between species and rapid infection. According to phylogenetic branches, SAR.CoV is close to SARS.CoV of bats.3
The virus was identified and characterized by Zhu et al., and also, confirmed that SARS-CoV-2, uses the same cell entry receptor, angiotensin-converting enzyme 2, as SARS-CoV, which is highly expressed in airway epithelial cells.4
Severe cases can manifest with pneumonia, severe acute respiratory syndrome, kidney failure2. As the infection spreads to other countries, infected persons, infect their contacts and health services must discriminate, based on clinical data and epidemiological history, the performance of the diagnostic test.
It is a pandemic with 1,991,562 confirmed cases and 130, 885 deaths until April 16, 2020 and cases have been reported in 212 countries, with death rate of 6.6%.5,6
In Mexico, the first confirmed cases were people who had traveled to the United States of North America or Europe; none travelled to China.7
The objective was to describe the evolution of the number of cases in Mexico per day and by source of contagion, until 28 March 2020.
Material and Methods
An ecological study was designed with data published by the National Epidemiological Surveillance System (SINAVE) of the General Directorate of Epidemiology of the Ministry of Health in Mexico until April 16, 20207.
The variables collected were: age, gender, trip to a country with high risk, date of beginning of clinical data and the state of residence of the patient. All cases were confirmed with the real-time RT-PCR test.
Each state is responsible for monitoring cases and reporting to the Federal Secretary of Health, if each patient was suspected, they were confirmed (positive RT-PCR test, they were ruled out, they had died.
The federal and state health systems centralized all the information on the cases and only the information compiled by the General Directorate of Epidemiology of the Federal Ministry of Health was included.
For statistical analysis, descriptive statistics were used, using the program STATA 13.0 ® (Stata Corp., College Station, TX, USA).
Results
According to what SINAVE reported, until April 16, 2020, there were 12,340 suspected cases of which COVID-19 was confirmed in 6,297, of which 486 deaths have been reported, mainly in Mexico City, State of Mexico and Sinaloa.6
Of the 6,297 confirmed cases, the age range was from 0 to 97 years, with a mean of 46.10 ± 15.74 years. This was calculated based on all confirmed cases.
Table 1 shows the distribution by gender and status of confirmed cases. The States with higher frequency of confirmed cases were Ciudad de México, Nuevo León, Jalisco, Yucatán, Estado de México, Quintana Roo and Puebla.
Table 1: Distribution by gender and Mexican States, confirmed cases of COVID-19 (n=6297)7
| n (%) | |
| Gender
Male Female |
3641 (57.82) 2656 (42.18) |
| States
Aguascalientes Baja California Baja California Sur Campeche Ciudad de México Chiapas Chihuahua Coahuila Colima Durango Estado de México Guerrero Guanajuato Hidalgo Jalisco Michoacán Morelos Nayarit Nuevo León Oaxaca Puebla Querétaro Quintana Roo Sinaloa San Luis Potosí Sonora Tabasco Tamaulipas Tlaxcala Veracruz Yucatán Zacatecas Total |
71 (1.13) 505 (8.02) 166 (2.64) 45 (0.71) 1828 (29.03) 54 (0.86) 108 (0.71) 214 (3.40) 7 (0.11) 17 (0.27) 695 (11.04) 100 (1.59) 96 (1.52) 67 (1.06) 178 (2.83) 84 (1.33) 48 (0.92) 29 (0.46) 159 (2.53) 53 (0.84) 305 (4.84) 76 (1.21) 276 (3.38) 327 (5.19) 56 (0.89) 89 (1.41) 233 (3.70) 78 (1,24) 62 (0.98) 112 (1.78) 131 (2.08) 18 (0.29) 6297 (100.00) |
Source: SINAVE/DGE
 |
Figure 1: Map of Mexico with states. |
The source of most cases was traveling to the USA and Spain, but there are already cases due to contact with a sick patient, which increases the possibility of the infection spreading.
The first confirmed case in Mexico was on February 20, 2020 and thereafter the largest number of confirmed cases were from March 19 to April 10, 2020 (Figure 1). The first cases were imported, but now community cases are increasing. The decrease in confirmed cases on 8 to 14 April 2020 may be artefacts due to delayed delivery of diagnostic test results. To this date, in the world, there were 1,991,562 confirmed cases.8
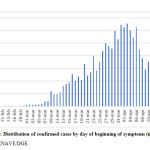 |
Figure 2: Distribution of confirmed cases by day of beginning of symptoms (n=6,297)7 |
Discussion
The sample of 6,297 confirmed cases predominated the males. At the beginning, the source of COVID-19, were travel to Europe or USA.
As reported by He et al.,9 the early cases were imported and the increase the local transmission of confirmed case. Similar to cases data from Mexico.
In Mexico from to 28 March to 16 April, 2020, the increase of confirmed cases was of 848 to 6,297, represented 742.57% and by day 39.08% , more than Italia with 25% increase of confirmed cases each day or Spain with 20%.10
Bulut et al.11, report that accord to early models total 10-12 weeks is required to control an outbreak in the community, but in all countries affected by COVID-19 is needed more than 12 week to flatted the epi.curve of new cases.
March 20, 2020, many governments of the Mexican states ordered the closure of schools at all levels and by March 25, 2020, public parks, mass shows, and gatherings of more than 10 people had already been closed. Any activity that gathered more than 10 people was cancelled. People do not go to restaurants, parks, gym, and another places.
Sanche et al.12, assumed a serial interval of 6-9 days, and they calculated a median R0 value of 5.7 (95% CI 3.8-8.9). They recommend that active surveillance, contact tracing, quarantine, and early strong social distancing efforts are needed to stop transmission of the virus.
Matrajt et al.13, reported that after social distancing interventions, 20% of new cases and most hospitalizations were averted, but to the end of intervention, the epidemic rebounded. Similar conclusion reported by Li et al.14, imposing social controls impact the number of new cases.
In countries from America until April 16, 2020, the worst situation is in USA with 632,781 confirmed cases and 28,221 deaths and Specific-Cause Mortality Rate (SCMR) of 4.46%, Canada with 28,884 cases and 1,048 deaths and SCMP=3.63%, Brazil 28,320 cases and 1,736 deaths SCMR=6.13%, Chile with 8,807 cases and 105 deaths and SCMR=1.19%. In LatinAmerican countries, Ecuador with 8,225 cases and 403 deaths SCMPR=4.90%, Peru, with 11,475 cases and 254 deaths with a SCMR=2.21%. In countries from Central America, the number of cases are less than Mexico8. In Mexico the SCMR = 7.71% with 6,297 confirmed cases and 456 deaths.15
Initial cases of COVID_19 in Mexico were for traveled to USA, Spain or Italy, none traveled to China. Now, the spread of the infection is for contact with cases (community spread).
Handwashing campaigns have been launched with soap and water and / or disinfectant gel, do not wave, cover nose and mouth with the elbow when coughing or sneezing. Isolation at home with practically no social activity has been recommended. All with the aim of reducing the transmission of the COVID-19.
The spread of COVID-19 infection is just over a month after it started in Mexico. Measures taken by governments and residents are expected to prevent the further spread of COVID-19 infection, but the health authorities declared that peak of epi-curve will be in May 2020.
Conclusion
The dissemination of COVID-19 is higher than March but the Ministry of Health from Mexico, are waiting that the last week of May will be the peak of cases in epidemiological curve.
The spread of COVID-19 in Mexico is more slow than another countries as USA, Italy or Spain.
Competing Interests Disclaimer
Authors have declared that no competing interests exist. The products used for this research are commonly and predominantly use products in our area of research and country. There is absolutely no conflict of interest between the authors and producers of the products because we do not intend to use these products as an avenue for any litigation but for the advancement of knowledge. Also, the research was not funded by the producing company rather it was funded by personal efforts of the authors.
References
- World Health Organization. Rolling updates on coronavirus disease (COVID-19). Updated 27 March 2020. 2020. Cited: 29 March 2020. Available in: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen
- Chotani RA. 2019-novel Coronavirus (COVID-19) Facts &Misconceptions. Just in Time lectures. Supercourse on Epidemiology, Internet and Global Health. 2020. Available in: http://www.pitt.edu/~super1/lecture/lec56501/001.htm
- Shereen MA, Khan S, Kazmi A, Bashir N, Siddiquea R. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses J Adv Res. 2020; 24: 91–98. Doi: https://doi.org/10.1016/j.jare.2020.03.005
- Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019 [published online ahead of print January 24, 2020]. N Engl J Med. https://doi.org/10.1056/NEJMoa2001017
- World Health Organization. Coronavirus disease 2019 (COVID-19). Situation Report – 87. 2020. Available in: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200416-sitrep-87-covid-19.pdf?sfvrsn=9523115a_2
- Unidad de Inteligencia Epidemiológica y Sanitaria. Secretaría de Salud. Comunicado técnico diario nuevo Coronavirus en el Mundo (COVID-19). Available in: https://www.gob.mx/cms/uploads/attachment/file/546980/Comunicado_Tecnico_Diario_COVID-19_2020.04.16.pdf
- Sistema Nacional de Vigilancia Epidemiológica. Dirección General de Epidemiología, Secretaría de Salud. Casos confirmados a enfermedad por COVID-19. 2020. Tabla_casos_positivos_COVID-19_resultado_InDRE_2020.04.16
- Pan American Health Organization. Number of COVID-19 cases in the region of the Americas as of 16 April 2020 at 02:00 pm. Available in: https://www.paho.org/en/documents/cumulative-suspected-and-confirmed-covid-19-cases-reported-countries-and-territories-21
- He GH, Rong ZH, Hu JX, Liu T, Xiao JP, Guo LC, et al. Comparison of two epidemic patterns of COVID-19 and evaluation of prevention and control effectiveness: an analysis based on Guangzhou and Wenzhou. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(0):E035. Doi: http://doi.org/10.3760/cma.j.cn112338-20200303-00242
- Cordova-Lepe F, Gutiérrez-Aguilar R, Gutiérrez-Jara JP. Number of COVID-19 cases in Italia at 120 days with data at 21/03/2020 and threshold of daily effort to flatten the epi-curve. Medwave 2020;20(2):e7861 Doi: http://doi.org/10.5867/medwave.2020.02.7861
- Bulut C, Kato Y. Epidemiology of COVID-19 Turk J Med Sci. 2020;50(S1-1): 563-570. Doi: http://doi.org/10.3906/sag-2003-172
- Sanche S, Lin YT, Romero-Severson E, Hengartner N, Ke R. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg Infect Dis. 2020; 26(7). Doi: https://doi.org/10.3201/eid2607.200282
- Matrajt L, Leung T. Evaluating the effectiveness of social distancing interventions to delay or flatten the epidemic curve of Coronavirus disease. Emerg. Infect. Dis. 2020; 26(8). Doi: http://doi.org/10.3201/eid2608.201093
- Li L, Yang Z, Dang Z, Meng C, Huang J, Meng H, et al. Propagation analysis and prediction of the COVID-19. Infectious Disease Modelling. 2020; 3: 282-292. Doi: http://doi.org/10.1016/j.idm.2020.03.002
- Pan American Health Organization. Number of COVID-19 cases in the region of the Americas as of 17 April 2020 at 02:00 pm. Available in: https://www.paho.org/en/documents/cumulative-suspected-and-confirmed-covid-19-cases-reported-countries-and-territories-22

