
Manuscript accepted on :14-04-2020
Published online on: 29-06-2020
Plagiarism Check: Yes
Reviewed by: Prasanna Tadi
Second Review by: Tahmineh Mokhtari
Final Approval by: Dr. Javad Sharifi-Rad
Ismail Setyopranoto* and Nurul Rakhmawati
and Nurul Rakhmawati
Department of Neurology Faculty of Medicine, Public Health, and Nursing Universitas Gadjah Mada Yogyakarta Indonesia and Dr Sardjito General Hospital, Yogyakarta, Indonesia
Corresponding Author E-mail: ismail.setyopranoto@ugm.ac.id
DOI : https://dx.doi.org/10.13005/bpj/1955
Abstract
Background: Stroke is a disease that causes high mortality and disability. The aortic diameter and carotid intima media thickness contribute to the functional outcome of ischemic stroke patients. Narrowing of the aortic diameter, carotid intima media thickness and ischemic stroke generally occurs because of the process of atherosclerosis. Objective: Proving the influence of aortic diameter with functional outcome in acute ischemic stroke patients. Material and Methods: The study design used a cross-sectional method with the first ischemic stroke subject treated at Dr. Sardjito General Hospital. Patients underwent echocardiographic examinations to assess aortic diameter and Carotid Intima Media Thickness (CIMT), whereas to assess functional outcomes of ischemic stroke, patients were examined by The National Institute of Health Stroke Scale (NIHSS). Results: Mean CIMT 0.8cm, with a range of 0.4-3.6, while the aortic diameter averages 29.2 ± 2.67 (22-35) mm. The functional stroke in this study used the NIHSS score, which obtained the average NIHSS score in this study was 6.13 ± 5.6 (1-25). This study showed no significant relationship between CIMT and ischemic functional stroke (p> 0.05), while a significant relationship was found between aortic diameter and functional stroke (p = 0.013; r = -0.332), ie diameter the aorta has a weak correlation strength to NIHSS, the lower the diameter, the greater the value of NIHSS, and vice versa. Conclusion: The aortic diameter is related to functional outcome but not to CIMT.
Keywords
Acute Ischemic Stroke; Aortic Diameter; Carotid Intima Media Thickness; Functional Outcome
Download this article as:| Copy the following to cite this article: Setyopranoto I, Rakhmawati N. Correlation Between Aortic Diameter and Carotid Intima Media Thickness (CIMT) With Functional Outcome in Acute Ischemic Stroke Patients. Biomed Pharmacol J 2020;13(2). |
| Copy the following to cite this URL: Setyopranoto I, Rakhmawati N. Correlation Between Aortic Diameter and Carotid Intima Media Thickness (CIMT) With Functional Outcome in Acute Ischemic Stroke Patients. Biomed Pharmacol J 2020;13(2). Available from: https://bit.ly/2ZdWkiY |
Introduction
Stroke is the second leading cause of death in the world and the third leading cause of death in the United States, after cardiovascular disease and cancer, and is a leading cause of functional disability for sufferers.1 Data of stroke in the world keep going up not only in elderly patient, but also in young patient.2 In Indonesia, based on the results of Riskesdas in 2013, the prevalence of stroke increases with age. The highest cases of stroke were over the age of 75 years (43.1%), and the lowest was in the age group of 15-24 years (0.2%).3
Atherosclerosis is a complex systemic chronic inflammatory process in the circulatory system, related to the elasticity of blood vessels, can affect all blood vessels and cause heart attacks and stroke (ischemia).4 The most commonly affected blood vessels are large blood vessels (aortic, carotid, and iliac arteries), as well as moderate blood vessels (coronary and popliteal arteries).4 One of the risk factors that take attention in ischemic stroke patients nowadays is a change in aortic diameter and carotid intima thickness, often called Carotid Intima Media Thickness (CIMT). Data showed that history of diabetes mellitus, level of LDL, HDL, and hypertension were all relevant to the increase development of the CIMT.5 The increase in CIMT values was related to the severity of ischemic stroke in patients with symptomatic extracranial carotid artery stenosis.6
Aortic stiffness is associated with ischemic stroke, also related to the aortic plaque thickness and other stroke risk factors.7 Research conducted in 2014 showed that aortic diameter could be a predictor of cerebrovascular disease severity.8
Atherosclerosis of the carotid arteries poses a great risk of cerebrovascular disease. In patients with asymptomatic to moderate stenosis, 0.35% to 1.3% will become an ischemic stroke.9 20% of ischemic strokes originate from carotid plaque. This study aims to prove the correlation between aortic diameter and CIMT with functional output in ischemic stroke patients.10
Material and Methods
This study used an analytic observational cross-sectional design. The descriptive study was used to determine the demographic characteristics and clinical characteristics of the subjects, while analytic studies were conducted to assess the correlation between aortic stiffness measured from aortic diameter and CIMT increase measured using TTE to the functional output of the stroke, measured using NIHSS. The study was conducted on ischemic stroke patients who were treated in the Stroke Unit of Dr. Sardjito General Hospital, Yogyakarta, Indonesia. Sampling was conducted using consecutive sampling techniques, from 1st January to 31st August 2018. Subjects were given inform consent and had been approved by ethics committee for human research Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada Yogyakarta, Indonesia.
Inclusion criteria in this study include; first-time acute ischemic stroke patients that have been confirmed by physical examination and Computed Tomography (CT) Scan; above 25 years old, willing to become a respondent and to sign the informed consent. Exclusion criteria in this study include loss of consciousness (GCS <9), intracranial infections, intracranial tumors, head trauma, systemic infections and/or sepsis, SIRS, coronary heart disease, aortic dissection, rheumatic heart disease and / or congenital heart disease, aortic stenosis, aortic regurgitation, myxoma, and the patients who use fibrinolytic drugs. First we obtain 60 subjects. 4 subjects are excluded in this study; 1 subject had myxoma in left atrium, 1 subject had pneumonia, and 2 subjects had passed acute phase (echocardiography was not done). The sample used in this study was 56 subjects.
Patients underwent echocardiographic examinations to assess aortic diameter and Carotid Intima Media Thickness (CIMT), whereas to assess functional outcomes of ischemic stroke, patients were examined by The National Institute of Health Stroke Scale (NIHSS).
The analysis in this study used descriptive and statistical analysis. For basic characteristics of subjects we use descriptive analysis, while statistical analysis includes bivariate and multivariate analysis. The data was expressed as number (percentage) for the categorical variables and mean± standard deviation (SD) for the continuous variables.To analyze the role of each variables in risk factors on NIHSS score, we use Pearson correlation test, while to analyze the effect and to predict those variables on NIHSS score, we use multiple linear regression test to obtain the coefficient determination (R2) and the constanta (b). All tests was considered as statistically significant with p value < 0.05.
Result
Basic Characteristics of Subjects and Role of Risk Factors on NIHSS
The number of subjects included in the inclusion and exclusion criteria was 56 people. The basic characteristics of the subjects can be seen in table 1. In the basic characteristics table, the average age of stroke patients is 63.33 years, the youngest age is 30 years and the oldest age is 94 years. The amount of male subjects were found to be more compared to female, 29 males (51.8%) and 27 females (48.2%). The level of education of the subject is based on the latest education; no education 10 subjects (17.9%), elementary school 9 subjects (16.1%), middle school 10 subjects (17.9%), high school 12 subjects (21, 4%), and university 15 people (26.8%), while the basic characteristics of the subject based on the type of occupation are 7 (12.5%) Civil Servants, 12 private employees (21.4%), 7 labor (12.5%), 6 farmers (10.7%), 6 pensioners (10.7%) and others 18 people (32.1%). The mean Body Mass Index (BMI) of the subjects was 23.31 kg / m2 (16.64-33.5). Based on the history, subjects who had a history of hypertension were 38 subjects (67.9%) and did not have a history of hypertension 18 subjects (32.1%), while only 15 subjects (26.8%) routinely took the anti-hypertensive medication. The mean systolic blood pressure was 158.76 ± 30.15, while the diastolic blood pressure was 86 (50-180) mmHg. Based on basic characteristics, subjects with a history of heart disease were 17 subjects (30.4%) and those without a history of heart disease were 39 subjects (69.6%). Subjects suffering from diabetes mellitus (DM) were 21 subjects (37.5%) and non-DM 35 subjects (62.5%), while the mean of random blood glucose levels was 122 mg/dl with a minimum value of 72 mg/dl and maximum 668 mg/dl, and the mean HbA1C is 6.5%, with a minimum value of 4.8% and a maximum of 16.8%. 17 subjects (30.4%) had a history of dyslipidemia, while non-dyslipidemia was 39 subjects (69.6%).
Table 1: Basic Characteristics of Subjects
| Variables | n (%) | Mean ± SD (*)
Median (Min-Max) (**) |
|
| NIHSS | 5.11 (1-23) ** | ||
| Aortic diameter | 29.37 ± 2.84* | ||
| Age | 63.3 ± 13.5 (30 – 94)* | ||
| Sex | Male | 29 (51.8%) | |
| Female | 27 (48.2%) | ||
| Level of education | No education | 10 (17.9%) | |
| Elementary School | 9 (16.1%) | ||
| Middle School | 10(17.9%) | ||
| High school | 12(21.4%) | ||
| University | 15 (26.8%) | ||
| Occupation | Civil servants | 7 (12.5%) | |
| Private employees | 12 (21.4%) | ||
| Labor | 7 (12.5%) | ||
| Farmer | 6 (10.7%) | ||
| Pension | 6 (10.7%) | ||
| Others | 18 (32.1%) | ||
| History of hypertension | Yes | 38 (67.9%) | |
| No | 18 (32.1%) | ||
| Consumption of anti-hypertensive drugs | Yes | 15 (26.8%) | |
| No | 41 (73.2%) | ||
| Systolic Blood Pressure | 158.76 ± 30.15* | ||
| Diastolic Blood Pressure | 86 (50-180)** | ||
| History of Heart Disease | Yes | 17 (30.4%) | |
| No | 39 (69.6%) | ||
| History of dyslipidemia | Yes | 17 (30.4%) | |
| No | 39 (69.6%) | ||
| Cholesterol Total | 193.15 ± 49.94* | ||
| Cholesterol LDL | 135.0 (32.0 – 226.0)** | ||
| Cholesterol HDL | 41.52 ± 13.81** | ||
| Triglycerides | 111.5 (38-314)** | ||
| History of Diabetes Mellitus | Yes | 21 (37.5%) | |
| No | 35 (62.5%) | ||
| Random Blood Glucose | 122.0 (72.0-668.0)** | ||
| HbA1C | 6.5 (4.8-16.8)** | ||
| Body Mass Index | 23.31 (16.40 – 33.58 )** | ||
| Onset | 12 (0.5-120)** | ||
| BUN | 13.95 (1.50-123.80)** | ||
| Creatinin | 1.1 (0.59-4.87)** | ||
| Leukocytes | 7.93 (3.24-20.17)** | ||
| Ao Asc Max | 126.13 ± 27.18* | ||
| Ejection Fraction | 70.50 (28.00-138.00)** | ||
| Carotid Intima Media Thickness (CIMT) | 8.0 (3.0-67.0)** | ||
Note: (*): normal distribution; (**): abnormal distribution
The values of lipid profiles in the study subjects are as follows; total cholesterol 193.15 ± 49.94 mg / dl; LDL 135.0 (32.0 – 226.0) mg / dl; HDL 41.52 ± 13.81 mg / dl; Triglycerides 111.5 (38-314) mg / dl. The mean value of Blood Urea Nitrogen (BUN) is 17.66 ± 17.57 mg / dl (1.5-123.8), and the mean value of Creatinine (Cr) is 1.1 mg / dl (0.59-4, 87). The mean leukocyte value is 7.93 (3.24-20.17) / mm3. The average AoAsc Max is 126.3 with a range of 61-168. The mean value of ejection fraction in this study was 70.50 (28-138)%. The mean NIHSS score in this study was 6.13 ± 5.6 (1-25). Furthermore, in this study, the average diameter of the aorta was 29.2 ± 2.67 (22-35) mm. Average CIMT of 8mm system with range 3-67.
Table 2: Role of Risk Factors on NIHSS
|
Variables |
NIHSS | r |
p |
||||||
| Median
(Min-Max) |
Mean ± SD | ||||||||
| Aortic diameter | -0.332 | 0.013* | |||||||
| Age | 0.056 | 0.682 | |||||||
| Sex | Male | 4 (1-25) | 5.07 ± 4.80 | 0.175 | |||||
| Female | 4 (1-23) | 7.26 ± 6.17 | |||||||
| History of hypertension | Yes | 4 (1-25) | 5.89 ± 5.85 | 0.501 | |||||
| No | 4.5(1-18) | 6.61 ± 5.03 | |||||||
| Consumption of anti-hypertensive drugs | Yes | 3 (1-12) | 4.20 ± 2.76 | 0.232 | |||||
| No | 4 (1-25) | 6.83 ± 6.16 | |||||||
| Systolic Blood Pressure | -0.047 | 0.737 | |||||||
| Diastolic Blood Pressure | 0.089 | 0.523 | |||||||
| History of Heart Disease | Yes | 4 (1-12) | 4.76 ± 3.05 | 0.653 | |||||
| No | 4 (1-25) | 6.72± 6.30 | |||||||
| History of dyslipidemia | Yes | 4 (1-23) | 5.59 ± 5.64 | 0.408 | |||||
| No | 4 (1-25) | 6.36 ± 5.59 | |||||||
| Cholesterol Total | 0.259 | 0.054 | |||||||
| Cholesterol LDL | -0.118 | 0.387 | |||||||
| Cholesterol HDL | 0.046 | 0.736 | |||||||
| Triglycerides | -0.224 | 0.097 | |||||||
| History of Diabetes Mellitus | Yes | 4 (1-25) | 9.33 ± 7.53 | 0.014* | |||||
| No | 4 (1-12) | 4.20 ± 2.55 | |||||||
| Random Blood Glucose | 0.239 | 0.079 | |||||||
| HbA1C | -0.087 | 0.527 | |||||||
| Body Mass Index | -0.022 | 0.872 | |||||||
| BUN | -0.023 | 0.864 | |||||||
| Creatinine | -0.150 | 0.269 | |||||||
| Leukocytes | 0.037 | 0.788 | |||||||
| Ejection Fraction | -0.270 | 0.044* | |||||||
| Carotid Intima Media Thickness (CIMT) | 0.098 | 0.473 | |||||||
In table 2 there was no significant difference between age and NIHSS score (p = 0.575). The average NIHSS for females was 7.26 higher than for males 5.07, in this study, no significant difference was found between gender and stroke output (p = 0.175). Based on the research of Wang et al. (2015), they found that overweight (25 <BMI <30 kg / m2) and age > 75 years were the independent risk factors for ischemic stroke (p <0.01), while this study found no significant differences between BMI and functional stroke output assessed based on NIHSS examination (p = 0.872). This study also did not find any significant differences in the history of hypertension with NIHSS (p = 0.501), taking anti-hypertensive drugs (p = 0.232), systolic (p = 0.737; r = -0.047), and diastolic (p = 0.523; r = 0.089). Subjects with a risk of heart disease in ischemic stroke patients were 65%. There were no significant differences between subjects suffering from heart disease with an NIHSS score (p = 0.653). These results are in accordance with the study done by Rasyid (2014). This study found a significant relationship between Diabetes Mellitus and NIHSS score (p = 0.014). DM subjects have a higher NIHSS score than those without DM. The level of random blood glucose did not have a significant correlation with the NIHSS score (p = 0.079; r = 0.239). The results of the study did not show a significant relationship between HbA1C and NIHSS scores (r = -0.087; p = 0.527). The results of the study did not show a significant relationship between the levels of lipid profile levels with NIHSS with total cholesterol (p = 0.054); LDL (p = 0.387); HDL (p = 0.736) and triglycerides (p = 0.097). This study also did not find any significant difference between BUN and NIHSS values (p = 0.864), as well as creatinine values (p = 0.269). This study did not find a significant correlation between leukocytes with NIHSS score (p = 0.788), but there was a tendency for higher leukocyte values to have a higher NIHSS score (r = 0.0375). The study showed a significant difference between the ejection fraction value and the NIHSS score, indicated by a positive correlation, meaning that the smaller the value of the ejection fraction, the greater the NIHSS score, and vice versa (Figure 1).
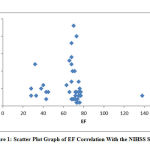 |
Figure 1: Scatter Plot Graph of EF Correlation With the NIHSS Scores |
The correlation test results showed no significant correlation between CIMT and NIHSS scores (p> 0.05). However, this study shows a significant correlation between aortic diameter with NIHSS score (p = 0.013). The smaller the aortic diameter, the greater the NIHSS value (r = -0.332). The correlation of aortic diameter to the NIHSS score is shown in the scatter plot graph below (Figure 2).
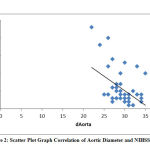 |
Figure 2: Scatter Plot Graph Correlation of Aortic Diameter and NIHSS Score |
Multivariate Analysis of the Role of Risk Factors and Aortic Diameter on the NIHSS Score
Variables that were continued to multivariate analysis were variables that had p <0.05 in the bivariate test, which were aortic diameter, ejection fraction, and history of DM. The analysis uses linear regression with the backward method as follows:
Table 3: Multivariate Regression Analysis
| Variables | Model 1
Coefficient p-value |
Model 2
Coefficient p-value |
Model 3
Coefficient p-value |
Model 4
Coefficient p-value |
| (Constant) | 44.256
0.000* |
45.014
0.000* |
44.499
0.000* |
40.536
0.000* |
| Aortic diameter | -0.886
0.001* |
-0.893
0.000* |
-0.968
0.000* |
-0.913
0.000* |
| History of Diabetes Mellitus | -4.560
0.001* |
-4.605
0.001* |
-4.914
0.000* |
-5.026
0.000* |
| Ejection Fraction | -0.045
0.211 |
-0.046
0.180 |
||
| R2 | 0.470 | 0.469 | 0.463 | 0.446 |
Multivariate analysis found 4 models in which the aortic diameter and history of DM had a significant effect on the NIHSS score (p <0.05). In the last model, the coefficient aortic diameter was -0.913, which means an increase in 1 mm aortic diameter would decrease the NIHSS score 0.913, and the coefficient of history of DM -4.56 which means patients with DM have an NIHSS score of 4.56 higher than non-DM. The coefficient determination (R2) of the aortic diameter and history of DM was 0.446, which means that the NIHSS score is influenced by both of these variables (44.6%), while the rest is influenced by other factors outside the study.
Discussion
Based on the results of the study, the variables associated with functional stroke output (NIHSS) are the history of diabetes mellitus, aortic stroke that is assessed from aortic diameter, and the ejection fraction. Patients with diabetes mellitus have an increased risk of atherosclerosis and an increased prevalence of atherogenic risk factors.11 Diabetes increases arterial stiffness through changes in vascular structure, such as decreased nitric oxide bioavailability, increased oxidative stress, low levels of chronic inflammation, increased sympathetic tone, and changes in elastin or collagen structure on arterial walls. Arterial stiffness is an important pathway that connects diabetes with an increased risk of cardiovascular disease.8,12 In the study of Shataratm et al. it was found that diabetic patients had transverse diameter, ascending aortic cutting area, descending aorta and pulmonary branches compared to patients without diabetes in both women and men (p <0.05).12 In study, higher CIMT values was found in ischemic stroke patients with diabetes mellitus.13
Patients with low ejection fraction are found to have impaired function of arterial wall distensibility due to complications from the ischemic heart. Decreased baroreceptor sensitivity will increase the incidence of arteriosclerosis and increase endothelial damage in blood vessel walls. Impaired cardiac baroreceptor sensitivity and decreased heart rate can be associated with poor clinical outcomes in ischemic stroke patients.14 Blood vessels in the brain are responsible for perfusion of the ischemic penumbra region, which loses autoregulation function during the acute phase of stroke, requiring greater blood supply from cardiac output to maintain cerebral blood flow. So that there is an association between low ejection fraction with poor clinical outcome in patients with acute ischemic stroke.15
Aortic stiffness is one of modifiable risk factors that can be modified to prevent stroke. Endothelial dysfunction plays a role in vascular disease through the release of vasoactive substances. Endothelial dysfunction causes structural stiffness, whereas structural stiffness worsens endothelial function. In several studies, this aortic stiffness can influence the functional outcome of stroke patient.17 Aortic stiffness seen from the aortic diameter is significantly related to the NIHSS score. The diameter of the aorta has a weak negative correlation to the NIHSS score. The smaller the diameter of the aorta, the worse the functional outcome. Aortic stiffness is an independent predictor of cardiovascular disease morbidity and mortality, including stroke. Aortic stiffness can provide prognostic information in ischemic stroke patients.7 The relationship between aortic stiffness with stroke is an increase in arterial stiffness that is responsible for an increase in systolic blood pressure and a decrease in diastolic blood pressure, thereby increasing pulse pressure (PP).17,18 Aortic stiffness can be measured by non-invasive methods through the assessment of Pulse Wave Velocity (PWV) on echocardiographic examination. Increased PWV is associated with fatal stroke. Other studies also report that low functional outcomes in acute ischemic stroke patients are associated with high PWV. Other study reported that aortic PWV >9 m / sec was significantly related to initial functional outcome of patient with stroke.17,19 In Dr Sadjito General Hospital, PWV, or cAIx examination is rarely performed, so aortic stiffness is measured based on aortic diameter using echocardiography. Changes in structure and qualitative proximal aorta will directly affect the aortic hemodynamics and afterload LV. The proximal diameter of the aorta is affected by age, an increase in aortic diameter is associated with tissue remodeling of the aortic wall, which affects the elastin tissue fragmentation, increased collagen and calcification which relate to the aortic wall stiffness.
In other study, there is an increased risk of stroke around 13%-18% with the absolute difference of CIMT around 0.1mm.5,20 However, the correlation test between CIMT and NIHSS scores in our study showed no significant correlation (p> 0.05).
The difference in results between this study and other studies might be due to the number of samples, differences in race, and methodology.
Conclusion
The conclusion obtained in this study is the aortic diameter has a significant correlation with the NIHSS score, but there is no correlation between CIMT and ischemic stroke functional outcome. Aortic stiffness is an independent predictor of cardiovascular disease morbidity and mortality, including stroke because it is responsible for an increase in systolic blood pressure and can worsen the functional outcome of patient with stroke. The smaller the aortic diameter, the worse the functional outcome, which is seen from the greater NIHSS score.
Acknowledgements
We would like to say thank you to Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada Yogyakarta, Indonesia that already help this research from the public funding in 2018. Beside that, we also would like to say thank you to I Putu Eka Widyadharma and Clarissa Tertia for the contribution in organizing and translating this paper.
Conflict of Interest
The authors declare that they have no conflict of interests.
References
- Arboix A. Cardiovascular risk factors for acute stroke: Risk profiles in the different subtypes of ischemic stroke. World Journal of Clinical Cases: 2015;3(5):418-429.
- Yueniwati Y, Darmiastini NK, Arisetijono E. Thicker carotid intima-media thickness and increased plasma VEGF levels suffered by post‑acute thrombotic stroke patients. Int J Gen Med. 2016;9:447–52.
- Riset Kesehatan Dasar (Riskesda). Badan Penelitian Dan Pengembangan Kesehatan Kementerian Kesehatan RI. 2013.
- Ammirati E, Moroni F, Norata GD, Magnoni M, Camici PG. Markers of inflammation associated with plaque progression and instability in patients with carotid atherosclerosis. Mediators Inflamm. 2015;2015.
- Bots ML, Evans GW, Tegeler CH, Meijer R. Carotid Intima-media Thickness Measurements: Relations with Atherosclerosis, Risk of Cardiovascular Disease and Application in Randomized Controlled Trials. Chin Med J (Engl). 2016;129(2):215–26.
- Heliopoulos I, Papaoiakim M, Tsivgoulis G, et al. Common carotid intima media thickness as a marker of clinical severity in patients with symptomatic extracranial carotid artery stenosis. Clinical Neurology and Neurosurgery., 2014;111:246–250.
- Cho EJ. Is Increased Aortic Stiffness Associated with Advanced Ischemic Stroke? Journal of Cardiovascular Ultrasound., 2013; 21(1): 10-11.
- Cuspidi C, Facchetti R, Bombelli M, Re A, Cairoa M, Sala C, Tadic M, Grassi G, Mancia G. Aortic root diameter and risk of cardiovascular events in a general population: data from the PAMELA study. Journal of Hypertension., 2014;32-9.
- Den Hartog A.G, Achterberg S, Moll F.L, et al., Asymptomatic carotid artery stenosis and the risk ishemic stroke according to subtype in patients with clinical manifest arterial disease. Stroke Journal., 2013;44(4): 1002-1007.
- Petty G.W, Brown Jr R.D, Whisnant J.P, Sicks J.D, O’Fallon W.M, Wiebers D.O. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke., 1999; 30:2513-6.
- Choudhury S.D, Das SK, Hazra A. Survey of knowledge-attitude-practice concerning insulin use in adult diabetic patients in eastern India. Indian Journal of Pharmacology., 2014;46(4): 425-429.
- Shatarat A.S, AL-Hadidi M.T, Badran D.H, Bustami F.F, AL-Hadidy A.M, Tarawneh E.S, Obeidat N.M, Abdul El Malek S.W. Sex-Specific Parameters of Ascending Aorta, Descending Aorta and Pulmonary Trunk by Computed Tomographic Angiography with Impact of Age, Hypertension, Smoking and Diabetes. J. Morphol., 2015;33(4):1411-1418.
- Das SK, Sarkar A, Pramanik S, Bandyopadhyay M, Mondal K, Singh SK. Carotid artery intima-media thickness in patients with acute ischemic stroke and its correlation with risk factors for atherosclerosis and/or stroke. Asian J Med Sci. 2014;6(1):22–7.
- Al-Qudah Z.A, Yacoub H.A, Souayah N. Disorders of the Autonomic Nervous System after Hemispheric Cerebrovascular Disorders: An Update. Journal of Vascular and Interventional Neurology., 2015;8(4): 43-52.
- Tiffany L, Mathias B.S, Karen C, Albright D.O, Amelia K.B, George B.S, et al.
- Chen Y, Shen F, Liu J, Yang GY. Arterial stiffness and stroke: De-stiffening strategy, a therapeutic target for stroke. Stroke Vasc Neurol. 2017;2(2):65–72.
- Gasecki D, Rojek A, Kwarciany M, Kowalczyk K, Boutouyrie P, Nyka W, Laurent S, Narkiewicz K. Pulse wave velocity is associated with early clinical outcome after ischemic stroke. Atherosclerosis., 2012; 225(2):348-52.
- Mitchell G.F, Lacourciere Cardiac Function and Short-Term Outcome in Patients with Acute Ischemic Stroke: A Cross-Sectional Study., 2008;15(10):1203-1214.
- Lee Y-B, Park J-H, Kim E, Kang C-K, Park H-M. Arterial Stiffness and Functional Outcome in Acute Ischemic Stroke. J Cerebrovasc Endovasc Neurosurg. 2014;16(1):11.
- Bian L, Xia L, Wang Y, Jiang J, Zhang Y, Li D, et al. Risk factors of subclinical atherosclerosis and plaque burden in high risk individuals: Results from a community-based study. Front Physiol. 2018;9(JUN):1–7.

