
Nawal Mustafa Abdullah1*, Mazin Abed Hazza2 and Abdul Kareem Qasim Mohamed3
1Department of Human Anatomy, Basrah Medical College, University of Basrah , Iraq
2Department medicine /cardiology, Basrah Medical College, University of Basrah, Iraq
3Department Pathology and Forensic medicine / Basrah Medical College, University of Basrah, Iraq
Corresponding Author E-mail: nawal.abdullah@uobasrah.edu.iq
DOI : https://dx.doi.org/10.13005/bpj/1848
Abstract
The left ventricular false tendons (LVFTs ) are fibrous or fibromuscular bands crossing the left ventricle in human hearts ,they arise mainly from the ventricular septum to the free wall or to a papillary muscle .They are considered as normal anatomical variant with different numbers, location and type. LVFTs had been associated with many clinical studies and discussions regarding their function . Literatures were reviewed and their incidence ,morphology , histology and clinical correlation were discussed .This study was intended to evaluate the existence LVFTs in Basrah city , and to compare the findings with other data verified in literatures. A prospective autopsy study of the prevalence and morphology of LVFTs in 215 cadaveric human hearts was performed to estimate the number ,types and location .of these bands .10 out of 215 samples were undergo routine histopathological processing to obtain 4 micrometer thickness slides stained with hematoxylin and eosin and examined for histological characteristics . LVFTs of varying number, types and different attachment were recorded in 62 ( 28.8% ) of 215 adult human cadaveric hearts studied. A complete morphologic assessments were done. No significant differences was found regarding age or gender. , Majority of LVFTs are single , commonly between the ventricular septum and papillary muscle .Fibrous and fibro muscular type is predominant . In our community false tendons are frequent anatomic variants of normal human LV which may be identified at routine examination and should not be mistaken as pathologic structures such as flail chordae tendineae or thrombi, further radiological and clinical studies are suggested to ensure their role and function .
Keywords
ventricular false tendons; incidence; morphology
Download this article as:| Copy the following to cite this article: Abdullah N. M, Hazza M. A, Mohamed A. K. Q. Ventricular False Tendons in Human Hearts ,An Autopsy Study of the Incidence ,Morphology ,Histology and Distribution in Basrah City;12(4). |
| Copy the following to cite this URL: Abdullah N. M, Hazza M. A, Mohamed A. K. Q. Ventricular False Tendons in Human Hearts ,An Autopsy Study of the Incidence ,Morphology ,Histology and Distribution in Basrah City;12(4). Available from: https://bit.ly/37dHkns |
Left ventricular false tendons (LVFTs) are isolated cordlike filaments of tissue that traverse the cavity of the left ventricle , they are attached to the ventricular septum , extending from the septum to the free wall ,or from the septum to the papillary muscle , from a papillary muscle to the free wall ,or between papillary muscles 1,2 . These bands are not found at all human hearts and considered within normal anatomical variations . Many identify them as intra cavity radiations of bundle of His 3,4. They are first reported by Turner at 1893 who incidentally found these fascinating structures at autopsy 5, Later, a series of morphological studies have widely explored the anatomic criteria of them in several mammalian species 6-9
LVFTs have various numbers, length and thickness, they could be single , multiple or branched , small multiple filaments at the junction of the septum with the free wall were considered an apical network 10,11. Most of these tendons were fibrous, or fibro muscular and sometimes they contain conducting fibers 12,13 The incidence of FTs in human has been rising with technical improvements,. The LVFTs nowadays become a common finding especially with the submission of ultrasound diagnostic instruments primarily with the use of routine 2-dimensional echocardiography recommended in human patients for different cardiac conditions. Nishimura supplied the first paper using echocardiography to demonstrate LVFTs in 1981 14.
Prior to the introduction of cardiac ultrasound, FTs in humans were identified at autopsy The earliest morphological studies recorded rates of 0.5% whereas recent investigations have achieved up to 78% in human and 95% of animal hearts .Other articles describe a range in 40-60% of examined hearts 15 .In a pathology study by Grzybiak et al , the prevalence was about 40% and it was similar across all age groups.16 Loukas et al reported the prevalence in a series of 200 gross pathology specimens to 62%… The results reported in literatures varied widely mainly because of the different methodologies and study designs ,age , race varieties, additional heart abnormalities and new equipment’s used .The embryogenetic origin of FTs was not fully elucidated , the most probable mechanism believed to involve displacement of conducting fibers into the LV lumen. In microscopic studies, the false bands consist of fibrous tissue, cardiomyocytes, blood vessels; they may also contain conducting fibers pertaining to the left branch of the His bundle 17,18
LVFTs are considered by many as benign anatomical variants . Recent morphologic studies have focused on the clinical importance of these bands ,several studies have indicated that they might have a pathophysiologic role in ventricular geometric anomalies. Increased prevalence of innocent precordial murmur and ventricular arrhythmias in humans, giant inverse T waves and left ventricular hypertrophy evident on resting electrocardiograms and pre-excitation mitral regurgitation considered to have possible relationship with these bands 19-26. No previous studies on LVFTs in local participant of Basrah city was done before .
Aim
The present study directed to describe the prevalence and characteristics of LVFs as normal anatomical variant and to estimate a prognostic significance of these structures and their role in clinical cardiac manifestations .
Materials and Methods
Anatomical study
The present work was enrolled during the period extended from March 2018 – December 2018 at forensic medicine department in Basrah with full ethical approval obtained . Two hundred fifteen human hearts were examined from cadavers for actual prevalence of LVFTs . The age ranged from 18-71yrs, gender distribution were 151 men (70.2%) / 64 women (29.8%) . Children , individuals below 18 years and those with obvious heart problems were excluded .
The normal hearts were cleaned of surrounding tissue and left ventricular chamber was opened. A scalpel incision on the lateral wall of left ventricle was made to visualize the interior and FTs. The number and location of these tendons were examined and identified as isolated fibrous or fibromuscular bands crossing the left ventricular cavity with no attachment to the atrioventricular valve ,they extend from a papillary muscle to the septum, or from a papillary muscle to the free wall, between papillary muscles, or from the septum to the free wall. The location of each band was described according to their points of attachment . The number was recorded as single ,multiple or branched and the type of the band like fibrous , fibromuscular or muscular is described .
Histological study
Visible false tendons from 10 of total 215 dissected hearts were examined for histopathological examination , 2-3 mm thickness tissue samples were preserved in 10% NBF and embedded in paraffin blocks .Sections of 4 micrometer thickness were stained with hematoxylin-eosin stain and examined under light microscope. A microphotographs at 10, 20, and 40 by using Elica camera were obtained .Data were collected, tabulated and statistically analyzed by a quantitative morphological assessment using ( version 21 ,SPSS,INC., Chicago ,Illinois ,USA ) and Pearson Chi-square test for qualitative data verification . P≤ 0.05 was considered statistically significant at all tests
Results
Morphological study
Data collected for 10 months with total 215 human hearts. Age ranged from 18-71yrs with mean age 36 years ± 14.9 . Male to female ratio was 2.4 : 1 . LVFTs found in 62 ( 28.8%) out of 215 hearts . ( Table 1 and Diagram 1) .
Table 1 : LVFTs percentage according to total number
| LVFTs | ||
| Percentage % |
No. |
|
| Negative | 71.2% | 153 |
| Positive | 28.8% | 62 |
| Total | 215 | |
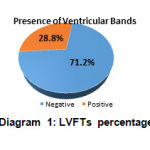 |
Diagram 1: LVFTs percentage
|
Regarding gender ,no of positive cases in male was 39 ( 25.8%) out of 151 male and in female was 23 ( 35.9%) out of 64 female , Male to female ratio was 2.4 / 1 . No significant difference was detected between M\F.(P value n.s (Table 2 and Diagram 2 ).
Table 2 : Male to Female ratio and % of positive LVFTs
| Count | Percent% | P value | |||
| Males | 151 | 70.2% | |||
| Females | 64 | 29.8% | |||
| % of positive | Count | LVFTs % according to gender | % Total (215) | ||
| Males | Positive | 39 | 25.8% | 18.1% | 0.135 |
| Negative | 112 | 74.2% | 52.1% | ||
| Females | Positive | 23 | 35.9% | 10.7% | |
| Negative | 41 | 64.1% | 19.1% |
P value = n.s.
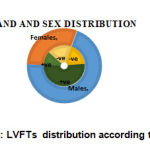 |
Diagram 2 : LVFTs distribution according to gender
|
Regarding number of bands ; the majority were single ( 53.2% ) followed by multiple bands ( 29.% ) . Multiple branching bands are less common with only 17.7% . A significant difference found between number of bands with significant p v( 0.000 ) (Table 3 ,Diagram 3 and Figure 1a, b, & c )
Results showed that false tendons were located frequently between papillary muscle and the ventricular septum ,P-S (41.9%) ,followed by FTs between ventricular septum and the free wall S-F type ( 24.2%) . Many attachments are combined and connect more than one point like papillary muscle to a papillary muscle to the septum PP-PS (8.1%) ,or false tendons from papillary muscle to ventricular septum , to the free wall or to a papillary muscle PS-,P-F,P-P, ( 6.5%) .few no include false tendons between papillary muscle to the septum to the free wall P-S,P-F( 1.6%) .Significant p-value (0.000) was detected(Table3,Diagram 4&Fig 2 a &b) .
This study found that the commonest type was the fibrous ( 66.1%) , followed by fibro muscular type ( 33.9%) while muscular type was uncommon . Significant P value was detected (0.000 ) (Table 3 ,Diagram 5 & Figure 3 a , b) .
Table 3: % of LVFTs regarding No of bands ,site and type
| Characteristics | Frequency % | Count | P-value | |
| Number of bands | Single | 53.2%** | 33 | 0.000 |
| Multiple | 29% | 18 | ||
| Multiple Branched | 17.7% | 11 | ||
| Band site | PS | 41.9%** | 26 | 0.000 |
| SF | 24.2% | 15 | ||
| PS,SF | 8.1% | 5 | ||
| PP,PF | 6.5% | 4 | ||
| PS,PF,PP | 4.8% | 3 | ||
| PS, SF | 3.2% | 2 | ||
| PP | 3.2% | 2 | ||
| PF,PP,SF | 3.2% | 2 | ||
| PF,PP | 3.2% | 2 | ||
| PS,PF | 1.6% | 1 | ||
| Band type | Fibrous | 66.1%** | 41 | 0.000 |
| Fibromuscular | 33.9% | 21 | ||
| Muscular | 0% | 0 | ||
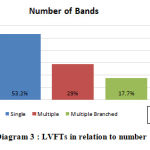 |
Diagram 3: LVFTs in relation to number .
|
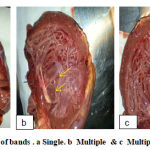 |
Figure 1: Number of bands . a Single. b Multiple & c Multiple-branched .
|
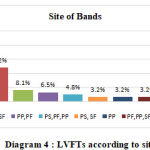 |
Diagram 4: LVFTs according to site.
|
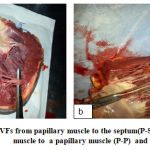 |
Figure 2: A, LVFs from papillary muscle to the septum(P-S) .B from papillary muscle to a papillary muscle (P-P) and P value ˂ 0.05
|
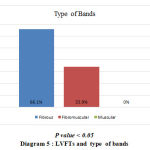 |
Diagram 5: LVFTs and type of bands
|
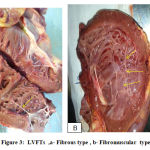 |
Figure 3: LVFTs ,a- Fibrous type, b- Fibromuscular type.
|
Histopathological study
The histological examination showed cardiac muscle tissue in different proportions ,cardiomyeocytes, ,conductive and connective tissue fibers , and abundant blood vessels . The fibromuscular type showed muscular and fibrous tissue crossed by small branches of coronary arteries. ( Fig 4 , a, b, c , & d)
 |
Figure 4: (a) and (b) Cardiac muscle fibers (10x & 40x) . (c) and (d) Blood vessels with connective &conductive tissue (40x).
|
Discussion
Various different terms have been used to describe left ventricular bands, these include; aberrant left ventricular chordae or anomalous, left ventricular chordate tendinae or tendinal cords, false chordae, false tendons, muscular strands, anomalous left ventricular bands, moderator bands and septomarginal trabeculae 2, 15, 26-29.
The high incidence of LVFTs have raised questions about their possible role in the malfunctioning of the heart. Many morphologic studies indicate that there could be a relationship between their existence and physiologic heart problems such as heart murmurs, arrhythmias or premature ventricular complexes. False tendons can be associated also with ventricular septal defects, a bicuspid aortic valve and coarctation of the aorta 30,31 , their functional significance remain largely unexplored till the establishment of the echocardiography which focus on these structures. From embryological point of view these ventricular bands have no obvious embryology ,it may be considered as an extension of the cardiac conduction system into the left ventricular cavity, It was found that many of these bands bear some similarity to chordae tendinae of mitral valve with similar mode of embryological origin ,the difference is they are not connected to the papillary muscles 32 . From developmental point of view these tendons were thought to have been derived from the inner muscle layer of the primitive heart 33 ;such a relation usually need more detailed morphological and clinical studies with more attention for these normal variants recently. In some of these tendons , few conductive tissue components found to be connected to the branch of bundle of His ,which support the idea of their role in the heart arrhythmias 17,26.
Previous studies found that both pathological and echocardiographic studies have controversy about their prevalence, morphology and clinical significance . The current study is the first to be done in Basrah city and demonstrates a lower incidence of LVFTs ( 28.8%) and this differ s from what Luetmer et al reported,he found that FTs exist in 55% of normal humans, while Gerlis et al. found them in 46%. These investigators also reported that most of the bands extended between the papillary muscles and the interventricular septum., another study found left ventricular bands in 47% of the 28 human hearts examined, located primarily between the interventricular septum and free wall 34 . In the present study the results demonstrate no significant difference between male and female while there is a significant difference found regarding the number of these bands ; majority are single, located mainly between the septum to the papillary muscle or between the septum to the free wall and usually composed of fibrous bands , this agrees with most studies done on LVFTs which emphasize on their anatomical bases . the differences detected in morphologic studies in humans could be due to differences in the thickness criteria of these bands or may could be due to race or methodology used 35, 36 , the most probable mechanism is believed to involve displacement of conducting fibers into the LV lumen ,they are considered to be a part of the conduction system that causes excess tension in the Purkinje fibers in the septum, thus irritating arrhythmia 37,38
Histopathological examination showed that FTs are mainly formed of cardiac muscle fibers , connective and conducting tissues, thick bands are composed of thickened endocardium with myocardial tissues that have all the features attributable to myogenic conducting tissues identical to that seen in the bundle of His . It is not clearly known whether these bands are functionally different although some studies correlate their presence with implication in cardiac arrhythmias, Because of the presence of muscular and conductive tissues ,it can be assumed that their contraction may effect electrophysiologic changes , this may explain their usual existence in subjects with innocent cardiac murmurs compared with normal subjects, However, such causation need further expanded clinical studies to achieve a clear understanding of a relationship between the morphology of left ventricular bands and the clinical presentation.
Conclusion
This study provided suggestions that:
LVFTs In Basrah population can be identified at all age groups and both genders . Majority were found between interventricular septum and papillary muscles with single appearance mostly and frequently as fibrous type .
LVFTs are common anatomical variants ,their prevalence is evaluated and compared with that reported in many published data of different populations .
Knowledge of the morphology and existence of these bands may be helpful to link them with cardiac murmurs and arrhythmias , beside it may minimize difficulties and critical points which are faced while introducing devices in the left ventricular catheterization.
Acknowledgements
Authors are grateful to forensic medicine department staff for their help
References
- Philip S, CherianKM, WuMH, LueHC. Left ventricular false tendons: Echocardiographic, morphologic, and histopathologic studies and review of the literature. Pediatr Neonatol 2011;52:279-86
- Turner W. Another heart with moderator band in the left ventricle. J Anat Physiol, 1896 ;30:568e9.
- Elizari MV1. The normal variants in the left bundle branch system; J Electrocardiol., 2017;50(4):389-399. doi: 10.1016/j.jelectrocard.2017.03.004
- Kosiński A, Grzybiak M, Dubaniewicz A, et al.(2012 ).False chordae tendineae in right ventricle of adult human hearts – morphological aspects .Arch Med Sci.2012;8(5):834-840,doi:10.5114\aoms.pubmed;23185192.
- Turner W.A heart with moderator band in left ventricle J Anat Physiol .1893;27:19 [Abstract
- Satish Kenchaiah, MD, MPH, Emelia J. Benjamin, MD, ScM, Jane C. Evans, DSc, Jayashri Aragam, MD, and Ramachandran S. Vasan, MD .Epidemiology of Left Ventricular False Tendons: Clinical Correlates in the Framingham Heart Study 3. J Am Soc Echocardiogr.; 22(6): 739–745. doi:10.1016/j.echo.2009.03.008
- Kervancioğlu M, Ozbağ D, Kervancioğlu P, et al. Echocardiographic and morphologic examination of left ventricular false tendons in human and animal hearts. Clin Anat..2003; 16(5): 389–395, doi: 10.1002/ca.10152, indexed in Pubmed: 12903060.
- Kimura Y1, Karakama S1, Kobayashi M1, Machida N2 Incidence, Distribution and Morphology of Left Ventricular False Tendons in Cat Hearts. Anat Histol Embryol.2016;45(6):490-493. doi: 10.1111/ahe.12216. Epub 2015 Oct 26.
- Heshmat SW Haroun. Comparative Anatomy of the Cardiac Septomarginal Trabecula (Moderator Band) , Anatomy Physiol Biochem Int J .2017 ;2(4): APBIJ.MS.ID.55595
- Luetmer PH, Edwards WD, Seward JB, Tajik . Incidence and distribution of left ventricular false tendons: an autopsy study of 483 normal human hearts. J Am Coll Cardiol .1986;8: 179–183
- Gerlis LM, Wright HM, Wilson N, Erzengin F, Dickinson DF . Left ventricular bands: a normal anatomical feature. Br Heart J .1984;52: 641–647
- .Deniz M, Kilinç M, Hatipoglu ES. Morphologic study of left ventricular bands. Surg Radiol Anat. 2004; 26(3): 230–234, doi: 10.1007/s00276-003-0212-0, indexed in Pubmed: 14648038
- Loukas M, Louis RG, Black B, et al .False tendons: an endoscopic cadaveric approach. Clin Anat..2007; 20(2): 163–169, doi: 10.1002/ca.20347, Pubmed: 16944521. 40.
- Nishimura T, Kondo M, Umadome H, Shimono Y. Echocardiographic features of the false tendons in the left ventricle. Am J Cardiol . 1981;48:177e83
- Loukas M, Wartmann CT, Tubbs RS, et al .Right ventricular false tendons, a cadaveric approach. Surg Radiol Anat. 2008; 30(4): 317–322, doi: 10.1007/s00276-008-0326-5, indexed in Pubmed: 18283389
- Grzybiak M, Lotkowski D, Kozlowski D .False tendons in the left ventricle of the heart in humans during pre- and postnatal periods. Folia Morphol. 1996; 55: 89–99.
- Francisco Sa´nchez Ferrer,a, * Marı´a Luisa Sa´nchez Ferrer,b Marı´a Dolores Grima Murcia,c Marina Sa´nchez Ferrer,a and Francisco Sa´nchez. . Basic Study and Clinical Implications of Left Ventricular False Tendon. Is it Associated With Innocent Murmur in Children or Heart Disease Rev Esp Cardiol.2015;68(8):700–705
- Saji Philip a,b,c , Kottureth Mammen Cherian a , Mei-Hwan Wu c , Hung-Chi Lue c,d,. Left Ventricular False Tendons:, Echocardiographic Morphologic, and Histopathologic Studies and Review of the Literature Pediatrics and Neonatology (2011) 52, 279e286
- Abdulla AK, Frustaci A, Martinez JE, Florio RA, Somerville J, Olsen EGJ Echocardiography and pathology of left ventricular ‘‘false tendons.’’ Chest: 1990;98: 129–132
- Malouf J, Gharzuddine W, Kutayli F..A reappraisal of the prevalence and clinical importance of left ventricular false tendons in children and adults. Br Heart J. 1986 ;55:587e91
- Bhatt MR, Alfonso CE, Bhatt AM, et al. Effects and mechanisms of left ventricular false tendons on functional mitral regurgitation in patients with severe cardiomyopathy. J Thorac Cardiovasc Surg .2009;138:1123e8.
- Kareem H, et al. Case Rep .A dancing ball in the heart’: false tendon of the left ventricle simulating a mass lesion BMJ .2013;doi:10.1136/bcr-2013-201115
- Mehul R. Bhatt, MD, Carlos E. Alfonso, MD, Amar M. Bhatt, BS, Sangmin Lee, MD, Alexandre C. Ferreira, MD, Tomas A. Salerno, MD, and Eduardo de Marchena, MD .Effects and mechanisms of left ventricular false tendons on functional mitral regurgitation in patients with severe cardiomyopathy .The Journal of Thoracic and Cardiovascular Surgery .2015; Volume 138, Number 5 1123
- Yuan Liu1, Ning Mi2, Yiming Zhou3, Peng An4 , Yongyi Bai1 , Yifang Guo5 , Changming Hong1 , Zhixin Ji6 , Ping Ye1 , Caie Wu1. Transverse False Tendons in the Left Ventricular Cavity are associated with Early Repolarization * PLOS ONE | .2015; DOI:10.1371/journal.pone.0125173
- Suwa M, Hirota Y, Kaku K, Yoneda Y, Nakayama A, Kawamura K, Dio K Prevalence of the coexistence of left ventricular false tendons and premature ventricular complexes in apparently healthy subjects a prospective study in the general population. J Am Coll Cardiol .1988;12: 910–914 17.
- Suwa M, Hirato Y, Nagao H, Kino M, Kawamura K .Incidence of the coexistence of left ventricular false tendons and premature ventricular contractions in apparently healthy subjects. Circulation.1984; 70: 793–798
- Boyd MB, Seward JB, Tajik AJ, Edwards WD. Frequency and location of prominent left ventricular trabeculations at autopsy in 474 normal human hearts: implications for evaluation of mural thrombi by two dimensional echocardiography. J Am Coll Cardiol 1987;9:323e6.
- Martins L, Van Zeller P, Rocha-Goncalves F, Ramalhao C, Cerqueira-Gomes M. Morphology, prevalence and clinical significance of left ventricular false tendons in adults. Acta Cardiol 1988;43:245e9.
- Choo MH, Chia BL, Wu DC, Tan AT, Ee BK. Anomalous chordae tendinae. A source of echocardiographic confusion. Angiology 1982;33:756e67.
- Kudoh Y, Hiraga Y, Imura O. Benign ventricular tachycardia in systemic sarcoidosis- a case of the false tendon. Jpn Circ J 1988;52:385e9
- Ker J. Subaortic tendon induced ST-segment elevationda new echo-electrocardiographic phenomenon? Cardiovasc Ultrasound 2009;24:7e13.-32
- Elizari MV1 The normal variants in the left bundle branch system.J Electrocardiol. 2017 Jul – Aug;50(4):389-399. doi: 10.1016/j.jelectrocard.2017.03.004. Epub 2017 Mar 14.
- Perry LW, Ruckman RN, Shapiro SR, Kuehl KS, Galioto Jr FM, Scott LP. Left ventricular false tendons in children: prevalence as detected by 2-dimensional echocardiography and clinical significance. Am J Cardiol 1983;52:1264e6
- Deniz M. Kilinc¸ E.M , Hatipoglu E. S. .Morphologic study of left ventricular bands .Surg Radiol Anat (2004) 26: 230–234
- Chaudhary S, Bharti RK, Deshpande H. A large morphological variant trifurcated septal band in right ventricle in middle east population: a case report. J. Evolution Med. Dent. Sci. 2016;5(58):4042-4043,
- Pisiak, K. Dorniak, M. Hellmann, D. Rawicz-Zegrzda, M. Węsierska, M. Dudziak .. Left ventricular false tendons: echocardiographic characteristics in the Polish population .Department of Noninvasive Cardiac Diagnostics, Medical University of Gdansk, Poland .2015
- Tamborini G, Pepi M, Celeste F, Muratori M, Susini F, Maltagliati A, Veglia F Incidence and characteristics of left ventricular false tendons and trabeculations in the normal and pathologic heart by second harmonic echocardiography. J Am Soc Echocardiogr, 2004;17: 367–374.
- Weir RA, Dargie HJ, Findlay IN .Arrhythmogenic left ventricular false tendon. Med J Aust,.2007; 187: 591.

