
Manuscript accepted on :13- 11-2019
Published online on: 21-11-2019
Plagiarism Check: Yes
Reviewed by: Ammar B
Second Review by: Hussein Adel
Final Approval by: Ayush Dogra
Mirfat Mohamed Labib El-Kashif 1,2
1Applied medical science collage, Wadi Addwaser, Prince Sattam Bin Abdulaziz Universivty, Saudi Arabia
2Maternity, obstetrics, and gynecology. nursing department - faculty of nursing- Port Said University, Egypt
Corresponding Author E-mail: drmirfat_k@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1832
Abstract
Urinary tract infection is widespread among pregnant women and is accompanying adverse maternal, fetal, and neonatal outcomes. Even so, no data exist regarding this problem in Wadi Addawser to guide specific management and thus to avert the adverse consequences. The study aimed to assess the urinary tract infection among pregnant women and its associated risk factors and to investigate the most common antibacterial agent used by infected pregnant women. A total of 303 pregnant women who attend the obstetrics and gynecology clinic with the inclusion criteria were included. The sample was collected using a structured interview. The study results showed, 53.5 % of the studied women had positive pathogens in the urine culture. E. coli (37%) followed by Klebsiella pneumonia (27%) had the highest percentage of the isolated pathogens. Amoxicillin and cefoxitin (40.1% &21.6%, respectively) are the most antibiotics used by infected women, while the lowest used antibiotics are fusidic acid (5.6%). The clinical symptoms such as frequency of micturition, dysuria, lower abdominal pain, urine color change, painful burning sensation, incomplete bladder evacuation were e most common among infected women. Since the symptoms are a good predictor for urinary tract infection during pregnancy, so early screening for pathogens and proper treatment for infected cases should be applied.
Keywords
An antibacterial agent; Pregnant women; Urinary tract infection
Download this article as:| Copy the following to cite this article: El-Kashif M. M. L. Urinary Tract Infection among Pregnant Women and its Associated Risk Factors: A Cross-Sectional Study. Biomed Pharmacol J 2019;12(4). |
| Copy the following to cite this URL: El-Kashif M. M. L. Urinary Tract Infection among Pregnant Women and its Associated Risk Factors: A Cross-Sectional Study. Biomed Pharmacol J 2019;12(4). Available from: https://bit.ly/2qogSYH |
Introduction
Pregnancy is associated with, structural, physiological and functional changes in the urinary tract which most often Resulting in ascending of pathogens into the urinary bladder, causing urinary tract infections (UTIs).1 In the general population, The extent of UTIs among pregnant women is higher than other healthy women.2 Both symptomatic and asymptomatic UTIs are prevalent among pregnant women and are linked with adverse effects to the mother, the fetus, and newborn. 1,3
The changes in the urinary tract during pregnancy and immune system increase the prevalence of bacteriuria, causing serious risks for both mother and fetus. Parity, Increasing age, sickle cell anemia, diabetes, urinary tract disorders and history of UTI, may increase the risk of urinary tract infection in pregnant women . 4,5
In pregnancy, urinary tract infection without antibiotic treatment may be result in serious complications such as low birth weight , preterm labor, hypertension , pre-eclampsia, anemia, pyelonephritis, amnionitis, stillbirths, neonatal deaths , bacteremia and toxic septicaemia.6,7 Treatment of urinary tract infection may reduce the risk of pregnancy complications. So, screening for early diagnosis and treatment of urinary tract infection in pregnant women is essential to avoid its complications. 8
Among pregnant women in Saudi Arabia, the prevalence of UTI was reported to be 20% (12% with symptomatic urinary trcat infection and 8% were asymptomatic.9 In general, the cases of UTIs are caused by bacteria bathogenes, especially gastrointestinal bathogens, that infects the urethral meatus through contaminating the area that surrounds the rectum and spreading to the bladder. 10
Approximately the common pathogenic causes of urinary tract infection are “Escherichia coli, Staphylococcus spp., Streptococcus spp., Proteus spp., Klebsiella spp. Corynebacterium, Neisseria, and Pseudomonas spp “. The severity of a urinary tract infection is influenced by the malevolence of the bacteria and the susceptibility of the host.11 Penicillin, Amoxicillin, celtaxidime, norfloxacin, and cefoxitin are the most competent antibiotics for the treatment of the majority of the urinary tract pathogens. 9
The significance of the present study is that urinary tract infection can be a danger for pregnant women between whom it has been revealed that up to 50% of those with asymptomatic Bacteriuria (ABU) go on to get pyelonephritis. Therefore, women during pregnancy should be assessed for predisposing factor and the causative organism of UTI during their antenatal follow-up. The urine examination for the presence of pathogens and the suitable antibiotic regimen should be specified for maternal and fetal health safety. The sensitivity for the antibiotics and their adverse reaction related to pregnancy should be considered 12
The aim of the study
This study aimed to assess the urinary tract infection among pregnant women and its associated risk factors, and to investigate the most common antibacterial used by infected pregnant women.
Material and Methods
Study design
A cross-sectional descriptive design
Study population and samples
The total subjects of the study sample consisted of 303 pregnant women who attend the antenatal clinic at Wadi Addwaser General Hospital, KSA with the inclusion criteria. The inclusion criteria are pregnant women at the second trimester of pregnancy with suspected clinical symptoms of urinary tract infection. The suspected clinical symptoms of urinary tract infection such as; the frequency of urination, fever, dysuria, painful burning sensation, strangury, incomplete bladder voiding, lower abdominal pain, flank pain, changed urine color and shaking chills. Exclusion criteria; sickle cell disease (renal damage), anatomic or functional congenital urinary abnormalities, the pregnant women under antibiotic regimen within 72 hours to the study data collection were excluded because the antibiotic must have inhibited or destroyed the pathogens.
Sampling
The data were collected through face to face interview from first October 2018 to end of March 2019 by using structured questionnaire that inclue; the socio-demographic characteristics as (age, level of education, occupation, and family income).
Obstetrical history( number of pregnancies, number of deliveries, abortion, number of children and Previous treatment for UTI during current pregnancy. Medical history and health habits ( regular voiding, drinking enough water, intake of vitamin C, frequent tea intake , soft drinks and coffee ingestion; . Medical history as
previous genital tract infection, hypertension, anemia , kideney calculi, and Diabetes Mellitus and clincal symptoms faced by pregnant women. The vaginal swab was taken from the study sample and analyzed to exclude vaginal infection according to the hospital rules.
Urine sample technique
enough clean-catch midstream urine specimen was collected by the pregnant women after given adequate and careful instructions for urine sample collection technique.
The urine sample was inoculated on blood agar- plates- (MacConkey agar). The urine sample plates were put in the incubator under perfectly aerobic conditions at 37°C for 24 hrs. After 24 hours of inculation, The urine culture plates were examend macroscopically to identify the color, appearance, morphology, and the colonies size. The isolated bacteria were diagnosed by using Gram stain and biochemical test and using microscopic examination. Antimicrobial susceptibility of isolated bacteria was examined to determine the proper antibiotic use. The presence of leukocyte (LE) and nitrate in urine were secreened by using the biochemical reagent strip test (dipstick test). The microscope was used to test red blood cells (RBCs) and pus cell (pyuria) in urine 13
Statistical analysis
The original data were coded and inserted into SPSS system files (SPSS package version 19, Chicago, USA). The data were analyzed and interpreted. Smirnov test was used to test the distribution of data. Univariate analyses including ( Mann Whitney test and t-test) were used to test the significance of the quantitative variables results. Monte Carlo test, Chi-Square test, and Fisher’s Exact test were used to testing the significance of the qualitative variables results.
Results
Out of 303 pregnant women, 162 women (53.5 % ) were positive for urinary tract pathogens. E. coli were the most frequent organism (37%) isolated from a positive pregnant women urine culture, followed by Klebsiella pneumonia (27%) while the lowest was staphylococcus saprophytic (3.7%). The study presented that amoxicillin and cefoxitin (40.1% &21.6%, respectively) are the most used antibiotics by infected women for the treatment of UTI, while the lowest used is the fusidic acid (5.6%) figure 1,2). Table (1): shows that there are statistically significant differences among negative and positive culture women concerning the age, occupation, family income, and previous treatment for UTI during current pregnancy at P≤0.05. And there were no differences with the number of pregnancies, number of deliveries, abortion and the number of living children.
Table (2) Reveals that there is a statistically significant difference between the presence of pathogens in urine culture in relation to regular bladder voiding, diabetes mellitus, previous urinary tract infection and regarding clinical manifestation among the pregnant women
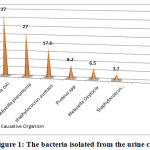 |
Figure 1: The bacteria isolated from the urine culture. |
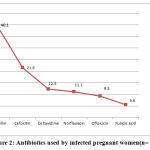 |
Figure 2: Antibiotics used by infected pregnant women(n= 162) |
Table 1: The Socio-demographic characteristics and the obstetric history of the studied pregnant women (n=303)
| Socio-demographic characteristics | Women with a negative culture
(n=141) |
Women with a positive culture
(n=162) |
Significance | |||
| No. | % | No. | % | |||
| Age (years) | ||||||
| Less than 25 | 30 | 21.3 | 33 | 20.4 | ||
| 25-<35 | 81 | 57.4 | 63 | 38.9 | ||
| 35-≤45 | 30 | 21.3 | 66 | 40.7 | ||
| Min-Max | 18.0-42.0 | 20.0-45.0 | t=2.082 | |||
| Mean±SD | 29.3±5.9 | 32.0±6.7 | P=0.040* | |||
| Level of education | ||||||
| Illiterate | 9 | 6.4 | 15 | 9.3 | ||
| Read and write | 18 | 12.8 | 30 | 18.5 | X2=5.145 | |
| Secondary school | 54 | 38.3 | 39 | 24.1 | MCP=0.280 | |
| University | 48 | 34.0 | 45 | 27.8 | ||
| Postgraduate studies | 12 | 8.5 | 33 | 20.3 | ||
| Occupation | ||||||
| Work | 42 | 29.8 | 93 | 57.4 | X2=7.760 | |
| Housewife | 99 | 70.2 | 69 | 42.6 | P=0.005* com | |
| Family income | ||||||
| Insufficient | 21 | 14.9 | 30 | 55.6 | X2=18.314 | |
| Moderate | 111 | 78.7 | 63 | 38.8 | MCP<0.0001* | |
| Enough | 9 | 5.6 | ||||
| NO of pregnancies | ||||||
| 1-2 | 51 | 36.2 | 51 | 31.5 | ||
| 3-4 | 48 | 34.0 | 48 | 44.4 | ||
| 5 or more | 42 | 29.8 | 39 | 24.1 | ||
| Min-Max | 1-9 | 1-12 | Z=0.618 | |||
| Median (Q1-Q3) | 3 (2-5) | 4 (2-4) | P=0.537 | |||
| Number of deliveries. | ||||||
| None | 39 | 27.7 | 24 | 14.8 | ||
| 1-2 | 66 | 46.8 | 75 | 46.3 | ||
| 3-4 | 24 | 17.0 | 39 | 24.1 | ||
| 5 or more | 12 | 8.5 | 24 | 14.8 | ||
| Min-Max | 0-8 | 0-8 | Z=1.431 | |||
| Median (Q1-Q3) | 2 (0-3) | 2 (1-3) | P=0.152 | |||
| Abortions | ||||||
| None | 87 | 61.7 | 123 | 75.9 | ||
| 1-2 | 48 | 34.0 | 30 | 18.5 | ||
| 3-4 | 6 | 4.3 | 9 | 5.6 | ||
| Min-Max | 0-3 | 0-4 | Z=1.462 | |||
| Median (Q1-Q3) | 0 (0-1) | 0 (0-0.5) | P=0.144 | |||
| Previous treatment for UTI during current pregnancy | ||||||
| Yes | 39 | 27.7 | 108 | 66.7 | X2=15.310 | |
| No | 102 | 72.3 | 54 | 33.3 | P<0.0001* | |
Q1-Q3: Interquartile range, Z: Mann Whitney test, X2: Chi-Square test, *significant at P≤0.05, t: Student t-test, MCP: Monte Carlo corrected, P-value, *significant at P≤0.05
Table 2: the predisposing factors and clinical manifestations of the studied pregnant women (n =303)
| Predisposing factors | Women with
NEGATIVE culture (n=141) |
Women with POSITIVE culture
(n=162) |
Significance | |||||||
| No. | % | No. | % | |||||||
| Health-related Habits during pregnancy | ||||||||||
| Vitamin C intake | 84 | 59.6 | 75 | 46.3 | X2=1.777 P=0.183 | |||||
| Regular bladder voiding | 123 | 87.2 | 99 | 61.1 | X2=8.755 P=0.003* | |||||
| Frequent soft drinks consumption | 69 | 48.9 | 99 | 61.1 | X2=1.508 P=0.219 | |||||
| Frequent tea consumption | 57 | 40.4 | 93 | 57.4 | X2=2.899 P=0.089 | |||||
| Frequent coffee consumption | 57 | 40.4 | 93 | 57.4 | X2=2.899 P=0.089 | |||||
| Drinking enough water | 111 | 78.7 | 102 | 63.0 | X2=2.989 P=0.084 | |||||
| Medical history | ||||||||||
| Genital tract infection | 45 | 31.9 | 54 | 33.3 | X2=0.023 P=0.880 | |||||
| Hypertension | 36 | 25.5 | 57 | 35.2 | X2=1.101 P=0.294 | |||||
| Kidney stones | 15 | 10.6 | 24 | 14.8 | X2=0.391 P=0.532 | |||||
| Diabetes Mellitus | 12 | 8.5 | 57 | 35.2 | X2=10.147 P=0.001* | |||||
| Previous urinary tract infection | 33 | 23.4 | 108 | 66.7 | X2=18.904 P<0.0001* | |||||
| Anemia | 66 | 46.8 | 57 | 35.2 | X2=1.408 P=0.235 | |||||
| Clinical manifestation | ||||||||||
| Painful burning sensation | 54 | 38.3 | 117 | 72.2 | X2=11.763 P=0.001* | |||||
| Incomplete bladder voiding | 39 | 27.7 | 105 | 64.8 | X2=13.910 P<0.0001* | |||||
| Frequency of urination | 66 | 46.8 | 147 | 90.7 | X2=23.227 P<0.0001* | |||||
| Fever | 27 | 19.1 | 66 | 40.7 | X2=5.507 P=0.019* | |||||
| Strangury | 30 | 21.3 | 90 | 55.6 | X2=12.345 P<0.0001* | |||||
| Dysuria | 33 | 23.4 | 129 | 79.6 | X2=31.292 P<0.0001* | |||||
| Shaking chills | 21 | 14.9 | 57 | 35.2 | X2=5.413 P=0.02* | |||||
| Flank pain | 48 | 34.0 | 96 | 59.3 | X2=6.407 P=0.011* | |||||
| Change urine color | 36 | 25.5 | 120 | 74.1 | X2=23.706 P<0.0001* | |||||
| Lower abdominal pain | 69 | 48.9 | 120 | 74.1 | X2=6.766 P=0.009* | |||||
| Laboratory results | ||||||||||
| Hematuria | 3 | 2.1 | 48 | 29.6 | X2=13.577 P<0.0001* | |||||
| Pyuria | 18 | 12.8 | 123 | 75.9 | X2=40.291 P<0.0001* | |||||
X2: Chi-Square test, *significant at P≤0.05
Discussion
The result of the present study revealed the overall prevalence of urinary trcat infection among pregnant women was (53.5%), which is abviousely higher than what was documented earlier in Saudi Arabia (20%). 9
In spite of the advances in medical and health care nowadys . This contrast in prevalence may be due to change in the studied sample and place of data collection. This result is nearly similar with the result of Worie & Eze., 2010 14 but it was lower than the result from Niger (75%) 15
Regarding bacteria isolated from the urine culture among pregnant women, the present results showed that the highest isolated organisms were E. coli (37%) and Klebsiella pneumonia (27%) while the lowest was staphylococcus saprophytic (3.7%). The previously mentioned result can be explained by the fact that the acidity of urine during pregnancy reaches the percentage that helps E. coli to grow.16. This finding is most consistent with many of the previous studies which determined that E. coli are the most common urinary tract associated bacteria.9,15,17-21. In another study, Staphylococcus aureus is the most prevalent pathogens among asymptomatic pregnant women. 22
In the current study, amoxicillin and cefoxitin (40.1% &21.6%, respectively) are the most used antibiotics by infected women for the treatment of UTI, while the lowest used is the fusidic acid (5.6%). In this respect, Faidah et al., 2013 9 reported that amoxicillin, cefoxitin, celtaxidime, norfloxacin, penicillin, and fusidic acid are the highest beneficial antibiotics for treatment of UTI during pregnancy. The effect of these antibiotics lies in these highly expensive drugs and had controlled their attaining and indiscriminate use, therefore facilitating the pathogens susceptible to them.
In this study, there is a statistically significant differences among negative and positive culture women concerning the age, occupation, family income and previous treatment for UTI during current pregnancy at P≤0.05. In this context, Eriksson, 201123 and Rahiman et al., 201516 reported that Urinary tract infection (UTI) is a common in women of all ages but the incidence and prevalence increase with age. Kolawole et al., 2009 14stated that socioeconomic rank is a predictor for the presence of bathogens in urine and this result from shortage in housing and drainage system, improper environmental and personal hygiene. From the researcher’s point of view, this could be attribute to the association of low socioeconomic status with Improper nutrition and low immunity especially during pregnancy. This study result is in line with the outcome of Tamalli et al., 2013 17 study which revealed that prevalence of bacteriuria in healthy women is found to be 9% and 21% in case of poor pregnant women. It is noticeable that the infection of the urinary system is widespread among working women, and this can be explained that working women do not drink enough water during working hours. Moreover, 66.7% of positive culture women have previous UTI during current pregnancy with P≤0.05. Kearney, 2011 25 mentioned that during pregnancy, there is a modification in the immune system of the pregnant woman to help implant the egg and the development of the fetus. So, the response of the immune system is modified from a cell-intermediated to a humoral reaction which results in fewer responses to bacterial cell surface proteins and probably facilitate pathogenicity. These modifications allow bacteria to penetrate, multiply and Settles in the urinary system
The current study results showed that the difference between the presence of bacteria in urine culture in relation to regular bladder voiding, diabetes mellitus, previous urinary tract infection was statistically significant. Rahiman et al., 2015 16 stated that emptying of the bladder is the dominant defense against urinary tract infection so, complete emptying the bladder during urinating and not ignoring the desire to urinate can help women to be away from urinary tract infections in most cases. Also, urinary tract infection was significantly associated with pregnant women who have diabetes mellitus and previous UTI. This is maybe attributable to elevate the glucosuria and decrease the immune system host factors prejudice to infection during pregnancy. Increase blood glucose during pregnancy causes a neutrophil disturbance by excessing calcium inside the levels of the cell and restrict with actin, also diapedesis and phagocytosis. The vaginal candidiasis and vascular disease also have a role in recurrent of infections. Also, this is due to the stoppage of the urine during pregnancy caused by physiological and anatomical changes in the urinary system, such as uterus compression on the ureters and the effect of the relaxation of progesterone on the urinary tract muscle.26 Moreover, Emiru et al.., 2013 27 proved that recurrent urinary tract infection and diabetes mellitus are risk factors for UTI, so the frequency and the severity of UTI rise in pregnancy.
The current study results revealed that, a statistically significant difference between presences of bacteria in urine culture in relation to clinical symptoms related to urination. The clinical symptoms such as frequency of micturition, dysuria, lower abdominal pain, urine color change, painful burning sensation, incomplete bladder evacuation. This result consistent with the results of Almushait et al., 2013 28 study which found nearly the same results. There is a statistically significant difference between the presence of pathogens in urine in relation to laboratory findings such as pyuria and hematuria P≤0.05 in the present findings. This result is in line with Michelim et al.., 2016 29, who stated that Pyuria is found in a majority of women with pyelonephritis.
Conclusion
Out of 303 pregnant women, 162 women were positive for utinary tract pathogens. E. coli were the most frequent organism isolated from a positive pregnant women urine culture, followed by Klebsiella pneumonia while the lowest was staphylococcus saprophytic. Amoxicillin and cefoxitin are the most used antibiotics by infected women for the treatment of UTI, while the lowest used is fusidic acid. There was a statistically significant difference between the presence of pathogens in urine culture in relation to regular bladder voiding, diabetes mellitus, previous urinary tract infection, and regarding clinical manifestation among pregnant women. Since the symptoms are a good predictor for urinary tract infection during pregnancy, so early screening for pathogens and proper treatment for infected cases should be applied.
References
- Matuszkiewicz-Rowi´nska J, Małyszko J, and Wieliczko M. Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems, Archives of Medical Science, vol. 11, no. 1, pp. 67–77, 2015.
- Ipe D.S, Sundac L, Benjamin Jr. L.W. H, Moore K. H, and Ulett G. C. Asymptomatic bacteriuria: prevalence rates of causal microorganisms, etiology of infection in different patient populations, and recent advances in molecular detection. FEMS Microbiology Letters, vol. 346, no. 1, pp. 1–10, 2013.
- Masinde A, Gumodoka B, Kilonzo A, & Mshana S.E. Prevalence of urinary tract infection among pregnant women at Bugando Medical Centre, Mwanza, Tanzania. Tanzania Journal of Health Research, vol. 11, no. 3, pp. 154–159, 2009.
- Giraldo P.C, Araújo E.D, Junior JE, Amaral R.L.G.D, Passos M.R.L, Gonçalves A.K. The prevalence of urogenital infections in pregnant women experiencing preterm and full-term labor. Infect Dis Obstetrics Gynecol. 2012;2012:1–4.
- Raza S., Pandey S., Bhatt C.P. Microbiological analysis of isolates in Kathmandu medical college teaching hospital, Kathmandu, Nepal. Kathmandu Univ Med J (KUMJ). 2011;9(36):295–7.
- Glaser A.P, Schaeffer A.J. Urinary Tract Infection and Bacteriuria in Pregnancy. Urol Clin North Am. 2015;42(4):547–60. https://doi.org/10.1016/j.ucl.2015.05. 004. Epub 2015 Aug 1.
- Izadi B, Rostami-Far Z, Jalilian N, Khazaei S, Amiri A, Madani S.H, Rostami-Far M. Urinary Tract Infection (UTI) as a risk factor of severe preeclampsia. Glob J Health Sci. 2016;8(11):54364.
- Smaill F, & Vazquez J.C. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev. 2015;8:CD000490.
- Faidah H, Ashshi A, Hada A, Al-ghamdi G, & Amr M. Urinary Tract Infections among pregnant women in Makkah, Saudi Arabia Biomedical & Pharmacology Journal. .(2013): Vol. 6(1), 01-07.
- Anuli S, Clement I, Basseye A. Review on the prevalence and predisposing factors responsible for urinary tract infection among adults. Eur J Exp Biol 2016; 6(4): 7-11.
- Hannan T.J, Totsika M, Mansfield K.J, Moore K.H, Schembri M.A, Hultgren S.J. Host-pathogen Checkpoints and Population Bottlenecks in persistent and intracellular uropathogenic Escherichia coli bladder infection. FEMS Microbiol Rev 2012; 36(3): 616-48.
- Prakash P, Krishan V, Hlufong L, AgrimaS, and Mahendra. Predisposing factors and etiology of urinary tract infections in pregnant women . DOAJ.Volume 3, Number 45. 2016: pp. 2244-2248(5)
- Cheesbrough M. Microbiological Tests. District Laboratory Practice in Tropical Countries, Part 2, 2nd ed., (Cambridge, Cambridge University Press,). 2006: 105 114,157159,156, 178179, 187189, 194195.
- Worie N, & Eze, U. A. Prevalence and Aetiologic Agents of Urinary Tract Infection in Pregnancy in Abakaliki Metropolis. Continental J. Medical Research. 2010: 4, 18 -23.
- Ebido L, Toluope A, and Deborah O. Urinary tract infection amongst pregnant in Amassoma, southern Nigeria. AJMR. 2015: Vol .9 (6), PP ,355-359.
- Rahiman F. O. M, Balasubramanian T, Shejina M, and Musambil M. A Review on Urinary Tract Infection in Pregnancy. International Journal of Pharma Research & Review, Feb; 2015: 4(2):26-33.
- Tamalli M, Sangar B, & Alghaza M. A. Urinary tract infection in pregnancy at Al-khoms, Libya. International Journal of Medicine and Medical Sciences. 2013: 3 (5), 455-459.
- Sharifa A.A. Asymptomatic Bacteriuria in Pregnant Women in Jeddah, Western Region of Saudi Arabia: Call for Assessment. JKAU: Med. Sci., 2010: 17 (1): 29-42.
- El-Sokkary M. Prevalence of Asymptomatic Bacteriuria in Antenatal Women with Preterm Labor at an Egyptian Tertiary Center. J. Am. Sci. 2011: 7(4): 605-610
- Alemu A, Moges F, Shiferaw Y, et al. Bacterial profile and drug susceptibility pattern of urinary tract infection in pregnant women at University of Gondar teaching hospital, in Northwest Ethiopia. BMC Res Notes. 2012: 5:197.
- Onuoha S.C, & Fatokun K. Prevalence and antimicrobial susceptibility pattern of urinary tract infection (UTI) among pregnant women in Afikpo, Ebonyi State, Nigeria. Am J Life Sci. 2014: 2(2):46–52.
- Jalali M, Shamsi M, Roozbehani N, and Kabir K. Prevalence of Urinary Tract Infection and Some Factors Affected in Pregnant Women in Iran Karaj City, 2013. Middle-East Journal of Scientific Research. ( 2014): 20 (7): 781-785, ISSN 1990-9233.
- Eriksson I. Urinary Tract Infection ‐ a serious health problem in old women: Electronic version available at http://umu.diva‐portal.org/ Printed by Print & Media, Umeå University, Umeå, Sweden 2011.
- Kolawole A.S, rowade K.A. C.F. Prevalence of urinary tract infection (UTI) among patients attending Dalhatu Arf specialist Hospital, Aafia, Nasarawa state, Nigeria IN?t. J . Med. Med. Sci. 2009: 1(5) ” 163-167.
- Kearney P. Urinary tract infection in pregnancy. ARTICLE in THE OBSTETRICIAN & GYNAECOLOGIST · JANUARY 2011: https://www.researchgate.net/publication/229442600, Retrieved on 21 March 2016.
- Chandel L.R, Kanga A, Thakur K, Mokta K. K, Sood A, Chauhan S. Prevalence of Pregnancy-associated Asymptomatic bacteriuria: A study was done in a tertiary care hospital. J Obstet Gynecol India. 2012: 62:511-4.
- Emiru T. G, Beyene W, Tsegaye and Melaku, S. Associated Risk Factors of Urinary Tract Infection among Pregnant Women at Felege Hiwot Referral Hospital, Bahir Dar, North West Ethiopia. 2013: BMC Res Notes, 25(6): 292.
- Almushait M, Mohammed H, Al-Harthy D, Abdullah A. Prevalence and Predisposing Factors of Urinary Tract Infections among Pregnant Women in Abha General Hospital International Journal of Sciences: Basic and Applied Research (IJSBARV. 2013:volume 11, No 1, pp 18-29 ISSN 2307-4531.
- Michelim L, Bosi G.R, & Comparsi E. Urinary Tract Infection in Pregnancy: Review of Clinical Management. 2016: J Clin Nephrol Res 3(1): 1030.

