
Smita A. Surale-Patil1 , Tatyasaheb Patil2 and Ravindra Kulkarni3
, Tatyasaheb Patil2 and Ravindra Kulkarni3
1Department of pharmacology, Krishna Institute of Medical Sciences Deemed To be University, Karad, Maharashtra, India, Pincode- 415110
2Pharmacologist Consultant Physician, Gurukripa, Station Road, Miraj, Maharashtra, India
3Bharati Vidyapeeth Deemed University Medical College and Hospital, Sangli
Corresponding Author E-mail: smitaasp73@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1806
Abstract
Wound healing is a complex, delicate process which consists of series of cellular and biochemical events leading to re-establishment of anatomical continuity. Anal fissure is a painful, chronic, non-healing wound. Its chronicity is due to spasm of anal sphincter and local ischemia. It is treated surgically by sphincterotomy to eliminate sphincter spasm. Therefore, Glyceryl trinitrate(GTN) has been used as a non-surgical alternative treatment due to its spasmolytic activity. The present study was undertaken to determine wound healing potential of GTN in wistar rats. 18 male wistar rats were divided in three groups, 6 rats per group Control (Normal saline), GTN, GTN Ointment base. A 500 mm2 excisional wound , circular in shape was created . The drugs were applied topically over the wound, one day after the wounding. Two parameters were studied viz; wound contraction and period of epithelization. Glyceryl trinitrate has shown statistically signfiicant difference in wound contraction compared to control on 10th day. Period of epithelization was not reduced significantly by Glyceryl trinitrate when compared to Control. Glyceryl trinitrate has wound healing potential apart from its spasmolytic action.
Keywords
Glyceryl trinitrate; excisional wound; wound contraction; epithelization
Download this article as:| Copy the following to cite this article: Surale-Patil S. A, Patil T, Kulkarni K. A Probe into Prohealing Potential of Glyceryl Trinitrate. Biomed Pharmacol J 2019;12(4). |
| Copy the following to cite this URL: Surale-Patil S. A, Patil T, Kulkarni K. A Probe into Prohealing Potential of Glyceryl Trinitrate. Biomed Pharmacol J 2019;12(4). Available from: https://bit.ly/2OkWek0 |
Introduction
Wound healing is a complex, delicate process which consists of series of cellular and biochemical events leading to re-establishment of anatomical continuity. Generally wounds heals without complications. There are many factors which affect wound healing. These factors may interfere with one of the phases of wound healing. There may be impaired wound healing, which leads to chronicity of wound eg. Chronic anal fissure, diabetic foot wound, venous ulcers. Chronic wound requires several days of treatment to achieve satisfactory healing without complications. The need for improving impaired wound healing has resulted in continued research on wound healing in human as well as animals.
Anal fissure is a painful, chronic, non-healing wound. It’s chronicity is due to spasm of anal sphincter and local ischemia.1,2 Commonly, anal fissure is treated surgically by sphincterotomy to eliminate sphincter spasm. Glyceryl trinitrate(GTN) is a non-surgical alternative treatment due to its spasmolytic action.3,4
GTN is also used to promote wound healing.5,6. GTN has been used in chronic anal fissure and compared with calcium channel blockers for its therapeutic effect.7.
The prohealing effect of GTN is believed to be due to smooth muscle relaxation resulting in mitigation of sphincter spasm and local ischemia.8,9 Since wound healing is a complex phenomenon, there is a possibility that wound healing potential of GTN may not be solely due to smooth muscle relaxant action. Therefore, the present study was undertaken to investigate, whether GTN has any wound healing property apart from its spasmolytic action. We have also studied the effect of GTN ointment base, to see if wound healing is due to the drug itself or is potentiated by the base.
Aim and Objectives
To determine wound healing potential of GTN.
Materials and methods
Study was carried out in 3 groups of rats ( 6 rats per group) for wound healing potential of Glyceryl trinitrate at Dept of Pharmacology and Central Animal House, Bharati Vidyapeeth Deemed University, Medical College & Hospital Sangli.
Synopsis was discussed in IAEC (Institutional Animal Ethical Committee). IAEC approved the project, IAEC approval registration no.- BVDUMC&H, Sangli CAH/ 2015/11
Total 18 male Wistar rats weighing 150-250 gm were taken. These were divided into three groups, 6 rats per group.
Chemicals / Drugs: surgical material used
Glyceryl trinitrate ointment- 0.2% (GTN) –Troikaa Pharmaceuticals Ltd.
Ointment base (OB) – Troikaa Pharmaceuticals Ltd.
Thiopental sodium, Spirit and Normal Saline, scissor, scalpel blade, artery forcep
Table 1: Group of animals and Drug Treatment Schedule for excisional wound model
| Group No. | No. of Animals | Drugs |
| 1 | 6 | Control (Normal Saline) |
| 2 | 6 | 0.2% Glyceryl trinitrate ointment |
| 3 | 6 | GTN Ointment Base |
Methodology
It was a double blinded study. Randomization was done by simple random method.
The animals bearing experimental wounds were treated with Normal Saline, GTN, GTN Ointment Base.
Wounding Procedure
The nape of neck of rat was shaved. All the rats were starved overnight with water ad libitum and the next day, surgical intervention under general anaesthesia was done to create excisional wound.
About 500 mm2 full thickness skin was excised, circular in shape with scalpel blade on the nape of the neck by using method of Morton and Malone10.
Drug Schedule
18 rats were wounded. 6 rats in each group received Normal Saline, GTN and GTN Ointment Base. Drug application was done locally once daily from the next day of wounding. The drug application was continued till the wound healed completely, as shown by total epithelization of the wound.
Monitoring of healing
Excisional wounds
Two parameters viz; contraction of wound and epithelization period were monitored. The wound contraction was accomplished by periodical (every 4th day post wounding) recording of wound size by planimetry or by tracing the wound area on polythene paper first and subsequently on mm2 paper every 4th day. The degree of wound healing was calculated as percentage closure of the original wound area using the following formula-
Percentage closure =A0 -Ad/ A0 х 100
Where A0 = wound area on zero day and
Ad= wound area on corresponding day.
The mean percentage of wound contraction and standard error of mean were calculated in control ( Normal Saline), GTN and GTN Ointment Base treated groups. The time required for epithelization was assessed in terms of days required for total fall of eschar with no trace of wound and full covering by glistening young epithelium.
Statistical Analysis
The level of significance between individual group was analysed using one way ANOVA. Data was expressed as mean ± SEM with a probability of p < 0.05 considered to be significant.
After completion of epithelization, animals were followed up by standard procedures as outlined by CPCSEA guidelines and rehabilitated.
Observations and Results
Table 2: Percentage of wound contraction.
| Group
|
No of Animals | .Drugs | Mean Percentage Wound Contraction ± .S.E.M. | ||
| 6th day. | 10th day | 14th day | |||
| 1 | 6 | Control(Normal Saline) | 55.33±6.04 | 74.00±1.63 | 90.33±1.82 |
| 2 | 6 | GTN | 70.67± 2.04 * | 81.00±1.98 * | 90.33± 1.50 |
| 3 | 6 | Ointment Base | 67.33±8.04 | 72.33±7.42 | 94.6±1.34 |
Data is expressed as Mean ± S.E.M. p < 0.05 is significant *= p < 0.05 When compared with Control
There was statistically significant difference in mean percentage of wound contraction of drug teated groups – GTN, when compared with Control indicating GTN, has enhanced wound contraction than Control on 10th day.
There was no statistically significant difference in mean percentage of wound contraction of drug treated groups – GTN, when compared with Control indicating GTN, has not enhanced wound contraction than Control on 6th day and 14th day.
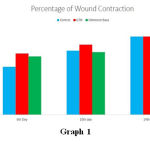 |
Graph 1 |
Period of Epithelization in Days
| Group no. | No of Animals | Drugs | Mean Period Of Epithelization |
| 1. | 6 | Control | 19.00±0.45 |
| 2. | 6 | GTN
|
17.83± 0.31 |
| 3. | 6 | Ointment Base | 19.00±0.45 |
Data is expressed as Mean ± S.E.M. p < 0.05 is significant * = p < 0.05 compared with Control
There was no statistically significant difference in means of period of epithelization with drug treated groups – GTN, GTN Ointment base, when compared to control indicating similar effect.
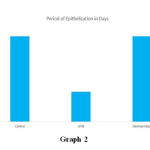 |
Graph 2 |
Discussion
GTN is used to treat chronic anal fissure. It acts by release of nitric oxide (NO), which increases concentration of Guanylyl cyclase. It increases cyclic GMP and brings out vasodilatation. GTN promotes wound healing by increasing blood supply and there by nourishment to the wound area. In addition, GTN activates cGMP, an intracellular intermediate, that inhibits the calcium activity. Calcium modulates cellular proliferation, modification, maturation of keratinocytes and fibriblasts.11
GTN increases angiogenesis which is more vital. Wound contraction mediated by myofibroblasts is a secondary effect to angiogenesis. GTN application stimulates the production of organized collagen fibres and dampens inflammatory response by reducing number of polymorphonuclear cells. An NO inhibitor or NO synthase inhibitor can retard wound healing and NO donors have beneficial effects on wound healing, which confirms the role of NO in wound healing.11
GTN acts as an NO donor. NO plays an important role in modulating cytokines that initiate the process of inflammation after formation of wound. NO modulates inflammation induced oedema formation and it inhibits inflammatory cell infiltration into granulomas. It is vital for the activity of pro-angiogenic cytokines. It also important in the Vascular Endothelial Growth Factor (VEGF) dependent and independent angiogenesis. Angiogenesis in wound bed is important to maintain newly formed granulation tissue. Keratinocyte proliferation and wound re-epithelization is NO dependent, which is mediated by VEGF. It plays important role in collagen synthesis which is important in the proliferative phase of wound healing, as collagen gives strength to wound.12,13. In a previous study it has been observed that NO has promoted re- epithelization in healing of wounds.6,14. An NO inhibitors or iNOS inhibitor can retard wound healing by decreasing proliferation of keratinocytes and delays healing.15,16
The present study was undertaken to determine if GTN possesses wound healing potential. The property of GTN regarding wound healing was compared with control group. GTN has shown increase in mean percentage of wound contraction on 10th day after wounding. Percentage of wound contraction of Control group (74.00±1.63) and that of GTN group is (81.00±1.98). There was statistically significant difference in mean percentage of wound contraction and GTN was better than control group. There was no statistically significant difference in period of epithelization when compared with control.
Thus from present study it seems that apart from spasmolytic activity Glyceryl trinitrate has wound healing property as it has enhanced mean percentage of wound contraction.
Conclusion
Apart from the spasmolytic activity of Glyceryl trinitrate, wound healing property has been demonstrated in our study, as it has enhanced mean percentage of wound contraction.
Acknowledgement
Authors acknowledge to Mrs Gore, Associate Professor, Department of Preventive and Social Medicine, Bharati Medical college and Hospital, Sangli for her valuable support in statistical analysis.
Conflict of Interest
No conflict of Interest
Funding Source
No funding was required
References
- Maria G. Etal. A Comparison of botulinum toxin and saline for the treatment of chronic anal fissure. N Eng J Med.1998; 338; 217-20.
- Schouten WR, Briel JW, Auwerda JJA, De Graaf E JR. Ischaemic nature of anal fissure. Br J Surg . 1996; 83:63-65.
- Lund JN, Scholefield JH.Randomized prospective, double-blind, placebo-controlled trial of Glyceryl trinitrate ointment in the treatment of anal fissure. Lancet. 1997; 349:11-14.
- Banerjee AR. Treating anal fissure. GTN ointment may remove the need for surgery. Br Med J. 1997; 314:1638-39.
- Effect of 0.2% GTN oint. On wound healing in streptozocin induced diabetes rats an expt’ study. Asian J Med Cli Sci. 2012; 1(2) : 86-88.
- Ghori V, Mandavia DR, Patel Tk, Tripathi CB. et al. Effect of topical nitric oxide donor (0.2% GTN) on wound healing in diabetic wistar rats. Int. J Diabetes Dev Countries. 2014; 34: 45-49.
- Franceschilli L ,Luca E, Milito G,Gaspari AL.Role of 0.4% glyceryl trinitrate ointment after haemorrhoidectomy. Int J Colorectal Dis.2012 Aug; 1544-51.
- Simon AJ, Breat RW Jr. GTN for anal fissure. Lancet. 1996;348: 491-92.
- Lund JN, Scholefield JM. Follow-up of patient with chronic anal fissure treated with topical GTN. Lancet 1998; 352: 491-92.
- Wild T,Rabarnia A, Kellner M, Sobotka L,Eberlein T. Basics in nutrition and wound healing.Nutrition.2010; 26: 862-66.
- Tripathi KD. Antianginal & other Antieschemic Drugs.In: Tripathi KD, editor.Essentials of Medical Pharmacology. New Delhi: Jaypee Brothers Medical Publishers(p) Ltd; 2013. p.539-57.
- Chong DY, Michel T. Pharmacology of vascular tone. In: Golan DE, Tashjian AH, Armastrong EJ, Armstrong AW, editor.Principles of pharmacology. Phildelphia: Lippincott Williams & Wilkins publisher; 2008. P. 367- 81.
- Katzung BG, Vasodilators & The Treatment of Angina Pectoris. In: Katzung BG, Trevor AJ, editor. Basic & Clinical Pharmacology. New Delhi : McGraw Hill Education(India). Publisher; 2015. P.191- 207.
- Stallmeyer B,Anhold M,Wetzler C,Kahlina K,Pfelschifter J, Frank S.Regulation of Enos in normal and diabetis- impaired skin repair: implications for tissue regeneration. Nitric Oxide. 2002; 6: 168-77.
- Opal SM,DePalo VA. Anti- inflammatory cytokines.Chest 2000; 117: 1162-72.
- Zuh H, Ka B,Murad F. Nitric Oxide accelerates the recovery from burn wounds. World J Surg .2007;31: 624-31.

