
Manuscript accepted on :12-Jan-2019
Published online on: 22-01-2019
Plagiarism Check: Yes
Reviewed by: Utkarsh Mangal
Second Review by: Aysegul Kovan
Final Approval by: Dr. Ayush Dogra
Nidhin Philip Jose1, Arjun Sehgal2, Siddarth Shetty1 , Lida Mary3 and Ashith M. V1
, Lida Mary3 and Ashith M. V1
1Department of Orthodontics, Manipal College of Dental Sciences, Mangalore, A Constituent College of Manipal Academy of Higher Education, Manipal.
2Orthodontist, Private practice, Mumbai, India.
3Department of Oral and Maxillofacial Surgery, A.J Institute of Dental Sciences, Mangalore, Rajiv Gandhi University of Health Sciences.
Corresponding Author E-mail: philipnidhin@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1647
Abstract
The hyoid and the tongue are intimately associated structures. The hyoid bone forms the anterior limit of the pharyngeal airway space. Thus, the position of hyoid bone and position of tongue can be considered determinants of pharyngeal airway space. Sixty samples, divided in three groups based on their growth pattern were studied and McNamara’s airway analysis and hyoid triangle analysis were used to evaluate the pharyngeal airway space and hyoid bone position respectively. A negative correlation was found in hyperdivergent group between the upper and lower airway space and the FMA. A positive correlation was seen in hyperdivergent group between the upper and lower airway space and the anteroposterior position of the hyoid bone.
Keywords
Hyoid Bone; Pharyngeal Airway Space; Vertical Skeletal Dysplasia
Download this article as:| Copy the following to cite this article: Jose N. P, Sehgal A, Shetty S, Mary L, Ashith M. V. Correlation Between Hyoid Bone and Pharyngeal Airway Space in Differing Vertical Skeletal Dysplasia. Biomed Pharmacol J 2019;12(1). |
| Copy the following to cite this URL: Jose N. P, Sehgal A, Shetty S, Mary L, Ashith M. V. Correlation Between Hyoid Bone and Pharyngeal Airway Space in Differing Vertical Skeletal Dysplasia. Biomed Pharmacol J 2019;12(1). Available from: http://biomedpharmajournal.org/?p=25736 |
Introduction
The hyoid bone is the only bone in the head and neck region which does not have any bony articulations. The hyoid bone along with the supra and infra hyoid group of muscles plays a crucial role in maintenance of head posture. The tongue influences the position of the hyoid bone.1 The hyoid and the tongue are intimately associated structures and both are positioned in space by a 3 point muscular suspension.2 The anterior limit of the pharyngeal airway space is formed by the hyoid. The pharyngeal airway space thus is affected by the position of the hyoid bone.1 Obstructive sleep apnea patients have been associated with a possibility of narrowing of pharyngeal airway space.3 Thus the position of hyoid bone and position of tongue can be considered to be determinants of pharyngeal airway space. Few studies have evaluated the position of hyoid bone in patients with different vertical skeletal dysplasia having a Class I skeletal base. The present study aims to determine the relationship between the position of the hyoid bone and pharyngeal airway space in patients with differing vertical dysplasia.
Materials and Methods
This was a retrospective study and a total of 60 samples with age between 17 to 25 years were selected for the study. The 60 samples were divided into 3 groups of 20 each based on their growth pattern. Frankfort Mandibular Plane Angle was used to categorize the three groups into Normodivergent growth pattern (FMA – 24±4), Hyperdivergent growth pattern (FMA> 29) and Hypodivergent growth pattern (FMA < 19). All samples had class I skeletal base with an ANB > 0 and < 3.5. Standardized Lateral cephalograms were selected from the departmental archives. Patients with gross dental abnormalities, oral habits, previous orthodontic treatment history or history of any diseases affecting the pharyngeal structures were excluded. All cephalograms were traced by the same operator. A few weeks later, 20 cephalograms were selected and retraced. The method error was evaluated and was found to be within acceptable limits.
Upper and lower airway widths were evaluated using McNamara‘s airway analysis4 (Figure 1). The upper pharyngeal width is the smallest distance from the posterior pharyngeal wall to anterior half of the soft palate outline. The normal value for an adult is 17 +/- 4 mm. A decreased measurement is used as an indicator for possible upper airway impairment.
The lower pharyngeal width is measured on the mandibular plane from the posterior tongue to posterior pharyngeal wall. The norm for an adult women is 11.3 +/- 4, while the norm for an adult male is 13.5 +/- 4. Values that are less than 15 millimeters suggest that the anterior positioning of the tongue is either postural or there’s an enlargement of the tonsils.
The hyoid bone position was determined using Hyoid triangle analysis5 (Figure 1.). The triangle is formed by joining the cephalometric points retrognathion (the most inferior, posterior point on the mandibular symphysis), hyoidale (the most superior, anterior point on the body of the hyoid bone) and C3 (the most anteroinferior point on the third cervical vertebra). The hyoid triangle relates the hyoid bone to the vertebrae and to the mandible.
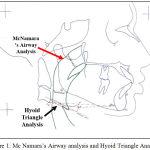 |
Figure 1: Mc Namara’s Airway analysis and Hyoid Triangle Analysis.
|
Statistical Analysis
The comparison of three groups was done using one-way ANOVA with post hoc tukey test. Pearson correlation coefficient was used to find out the correlation of the hyoid bone position with the pharyngeal airway space. Level of significance is set at P < 0.05. All statistical analysis was carried out with SPSS software. (SPSS Inc, Chicago, version 13).
Results
The groups were divided on the basis of FMA into hypodivergent , normodivergent and hyperdivergent growth pattern. This was verified by the fact that FMA were significantly different in the three groups. The sample was selected such that all the patients were Class I skeletal base and this was evident by the ANB value not showing any significant difference in between the three groups. The results of the ANOVA test done to compare the upper and the lower airway space and the horizontal position of the hyoid bone between the three groups concluded that the horizontal position of the hyoid was very stable and the difference between the groups is not statistically significant. Pearson’s correlation coefficient (Table 1) showed a negative correlation between FMA and upper and lower airway space in hyperdivergent group indicating that as FMA increased upper and lower airway space decreased. Also, a positive correlation was seen in hyperdivergent group between the upper and lower airway space and the anteroposterior position of the hyoid bone.
| Group | N | Pearsons Correlation (R) | ||
| Normodivergent | Pair 1 | Upper Airway & Hyoid Angle | 20 | .012 |
| Pair 2 | Upper Airway & Vertical | 20 | -.308 | |
| Pair 3 | Upper Airway & Hrgn | 20 | .271 | |
| Pair 4 | Upper Airway & C3h | 20 | .064 | |
| Pair 5 | Lower Airway & Hyoid Angle | 20 | -.230 | |
| Pair 6 | Lower Airway & Vertical | 20 | -.302 | |
| Pair 7 | Lower Airway & C3h | 20 | .066 | |
| Pair 8 | Lower Airway & Hrgn | 20 | .128 | |
| Hyperdivergent | Pair 1 | Upper Airway & Hyoid Angle | 20 | -.334 |
| Pair 2 | Upper Airway & Vertical | 20 | -.646 | |
| Pair 3 | Upper Airway & Hrgn | 20 | .086 | |
| Pair 4 | Upper Airway & C3h | 20 | .489 | |
| Pair 5 | Lower Airway & Hyoid Angle | 20 | -.274 | |
| Pair 6 | Lower Airway & Vertical | 20 | -.509 | |
| Pair 7 | Lower Airway & C3h | 20 | .689 | |
| Pair 8 | Lower Airway & Hrgn | 20 | .191 | |
| Hypodivergent | Pair 1 | Upper Airway & Hyoid Angle | 20 | -.059 |
| Pair 2 | Upper Airway & Vertical | 20 | -.179 | |
| Pair 3 | Upper Airway & Hrgn | 20 | .194 | |
| Pair 4 | Upper Airway & C3h | 20 | .111 | |
| Pair 5 | Lower Airway & Hyoid Angle | 20 | -.194 | |
| Pair 6 | Lower Airway & Vertical | 20 | -.263 | |
| Pair 7 | Lower Airway & C3h | 20 | -.057 | |
| Pair 8 | Lower Airway & Hrgn | 20 | .230 | |
Discussion
The assessment of the horizontal position of the hyoid bone as evident from the ANOVA test results revealed that the hyoid bone is relatively constant. This is in accordance with the findings reported by Bibby and Preston5 and Kumar.6 The hyoid also maintains a very constant relationship to the cervical vertebrae as shown by the C3‑H values in the three groups. This finding is in agreement with previously published results by Bibby and Preston,4 Tourné7 and Haralabakis.8 Duggal,9 in contrast showed that the position of the hyoid bone in subjects with short face syndrome was more anterior than in subjects with long face syndrome. This could be attributed to the severity of the short face and long face patients since the cases selected in their study were not restricted to only class I skeletal base.
In this study, the upper and lower airway showed a negative correlation with FMA in hyperdivergent group, i.e. increase in FMA reduced the upper and lower airway spaces. The vertical position of the hyoid bone was comparable among subjects with different vertical jaw dysplasia which was similar to study done by Duggal.9
Grant10 did a study on hyoid bone positions in Class I, Class II and Class III malocclusions and reported that the hyoid position is constant in the three types of malocclusions. He also said that the musculature and not the occlusion of the teeth determine the position of the hyoid. A similar study was done by Jose et al11 on hyoid bone position in class I, Class II, and Class III malocclusions and reported that the hyoid bone maintained a relatively constant position in patients with all three malocclusions in average growers.
The highlight of this study lies in the fact that all the samples had a class I skeletal base unlike in the previous studies. Only class I skeletal base cases were selected in order to evaluate whether class I skeletal patients with different growth patterns also show any variation in hyoid bone position and to minimize any role played by the sagittal position of the mandible.
Conclusion
A negative correlation was found in hyperdivergent group between the upper and lower airway space and the FMA.
A positive correlation was seen in hyperdivergent group between the upper and lower airway space and the anteroposterior position of the hyoid bone.
Acknowledgments
The author(s) received no specific funding for this work.
References
- King E. W. A roentgenographic study of pharyngeal growth. Angle Orthod. 1952;22:23–25.
- A. G. Consideration of musculature in diagnosis, treatment and retention. Am. J. Orthod. Dentofac. Orthop. 1952;38:823.
CrossRef - Hoekema A., Hovinga B., Stegenga B., De Bont L. G. Craniofacial morphology and obstructive sleep apnea a cephalometric analysis. J Oral Rehabil. 2003;30:690–696.
CrossRef - McNamara Jr J. A. A method of cephalometric evaluation. Am J Orthod 1984; 86:269-300.
CrossRef - Bibby RE, Preston CB. The hyoid triangle. Am J Orthod. 1981;80:92‑7.
CrossRef - Kumar K. J. A study of hyoid bone position and its relation to the oral and pharyngeal spaces in normal and malocclusion subjects. Master’s Thesis. University of Kerala. 1983.
- Tourné L. P. Growth of the pharynx and its physiologic implications.Am J Orthod Dentofacial Orthop. 1991;99:29.
CrossRef - Haralabakis N. B., Toutountzakis N. M., Yiagtzis S. C. The hyoid bone position in adult individuals with open bite and normal occlusion. Eur J Orthod. 1993;15:265‑71.
CrossRef - KumarA.,Duggal R. Hyoid bone position in subjects with different vertical jaw dysplasias. AO. 2011;81:81-85.
- Grant L. E. A radiographic study of the hyoid bone position in Angle’s class I, II and III malocclusions. – Unpublished Masters Thesis, University of Kansas City 1959, Cited in Stepovich M. L Am. J Orthod. Dentofac. Orthop. 1965;51(12):882-900.
- Jose P. N. Evaluation of hyoid bone position and its correlation with pharyngeal airway space in different types of skeletal malocclusion. Contemporary Clinical Dentistry Apr-Jun. 2014;5:2.
CrossRef

