
Manuscript accepted on :15-Nov-2018
Published online on: 20-11-2018
Plagiarism Check: Yes
Reviewed by: Vinisha Pandey
Second Review by: Vyoma Shah
Jyothsna Pinni1 , J. S. Sankar Avula2, Sridhar Mukthineni2, Sujatha Bandi3 and Thulasi Gokul4
, J. S. Sankar Avula2, Sridhar Mukthineni2, Sujatha Bandi3 and Thulasi Gokul4
1Department of Pedodontics and Preventive Dentistry, Thai Moogambigai Dental College and Hospital, Chennai, Tamil Nadu, India.
2Department of Pedodontics and Preventive Dentistry, Sibar Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
3Department of Pedodontics and Preventive Dentistry, Narayana Dental College and Hospital, Nellore, Andhra Pradesh, India.
4Department of Pharmacology, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
Corresponding Author E-mail: pinnijyothsna@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1578
Abstract
Plant materials were known as source of new antimicrobial agents. Many efforts have been made to develop alternative mouth rinses from natural products which are safe, easily available and substitute the standard pharmaceutical remedies. Thus, considering the therapeutic value of pomegranate fruit, the present study was designed to compare the antimicrobial efficacy of aqueous extract of Pomegranate pericarp and commercially available Chlorhexidine mouth wash against caries causative microorganisms both in vitro and in vivo. To evaluate the antimicrobial efficacy of pomegranate pericarp extract (PPE) against Streptococcus mutans (S.mutans) and to determine its usefulness as anti caries mouth rinse. In vitro antimicrobial efficacy was evaluated by disc inhibition zone method and broth dilution assay considering minimum inhibitory concentration of PPE. In vivo evaluation was done as a randomised controlled trial which included thirty children aged between 6-12 years. They were divided randomly into 3 groups of ten each and subjected to different mouth rinses - Group I: PPE mouth rinse, Group II: 0.2% Chlorhexidine mouth rinse and Group III: Distilled water (control). The salivary samples which were collected before and after (5 minutes) mouth rinsing were inoculated on Mutans Sanguis agar and the bacterial count was calculated.Statistically significant decrease in salivary S.mutans count was observed in group I and II compared to group III after mouth rinsing. However, there was no statistically significant difference between groups I and II. PPE mouthwash was effective in reducing the salivary S.mutans count and was comparable to chlorhexidine mouth rinse. Hence PPE mouth rinse may be considered as a potential anti caries mouth rinse.
Keywords
Chlorhexidine; Minimum Inhibitory Concentration; Mouthwash; Pomegranate Pericarp Extract; Streptococcus Mutans
Download this article as:| Copy the following to cite this article: Pinni J, Avula J. S. S, Mukthineni S, Bandi S, Gokul T. Evaluation of Anticariogenic Efficacy of Pomegranate (Punica Granatum) Pericarp Extract as Natural Mouth Rinse: An In Vitro and In Vivo Study. Biomed Pharmacol J 2018;11(4). |
| Copy the following to cite this URL: Pinni J, Avula J. S. S, Mukthineni S, Bandi S, Gokul T. Evaluation of Anticariogenic Efficacy of Pomegranate (Punica Granatum) Pericarp Extract as Natural Mouth Rinse: An In Vitro and In Vivo Study. Biomed Pharmacol J 2018;11(4). Available from: http://biomedpharmajournal.org/?p=24086 |
Introduction
Dental caries is one of the most common chronic infectious diseases in the world which is influenced by multiple factors such as diet, host characteristics and cariogenic microorganisms, of which Streptococcus mutans (S.mutans) is a significant contributor to tooth decay.1
The prime mode of preventing the development and progression of dental caries is through mechanical plaque control (regular tooth brushing). Mouth rinses are medicated solutions which are recommended as an antimicrobial, topical anti-inflammatory solutions so as to decrease halitosis and deliver fluoride for caries prevention in general. They are beneficial especially to mentally and physically challenged patients who lack manual dexterity. A multitude of products have arisen, during the past few decades which contain different active chemical ingredients like chlorhexidine, triclosan, fluoride mouth rinses etc.2
Chlorhexidine is considered as a gold standard anti-plaque agent because of its broad spectrum antimicrobial activity.3 However, its long term usage can cause tooth staining, unpleasant taste, increased calculus formation and mucosal erosion at higher concentrations.4 These short comings have led to the need for further research and introduction of new antibacterial agents which are derived from natural resources with minimal / no side effects on the oral tissues especially in children.
Nature has enormous plant sources which have good medicinal value and work against pathogenic microorganisms. Pomegranate (Punica granatum) is one such natural source that is currently finding important applications in the field of dental health.5 The healing property of pomegranate was discussed in one of the oldest medical texts, the Eber’s Papyrus from ancient Egypt (1500 BC).3 In Ayurvedic medicine, pomegranate is considered “a pharmacy unto itself” and as a remedy for diabetes in Unani medicine. Various components of this plant such as the leaves, flowers, roots, bark and fruit extracts have been used for a variety of ailments.6
Even though there is ample evidence regarding the antimicrobial efficacy of PPE in various in vitro studies, its clinical evidence is very minimal. Considering this fact, the present study is an attempt to evaluate the clinical applicability of naturally available PPE as mouth rinse in children.
Materials and Methods
Following the approval from the institutional ethical committee, the present microbiological study was conducted in the department of Pedodontics and Preventive dentistry in collaboration with department of Microbiology and Pharmacology.
Fresh ripen pomegranate fruits were procured from local market and the pericarps were separated manually, shade dried for 7 days, powdered and stored under freezing condition until its use [Figure I]. This powder was mixed in different concentrations (250, 500, 750 and 1000 mg) with 10 ml of distilled water in Jiffy’s centrifuge tubes. These four concentrations of extracts were immersed in thermostatic water bath at a temperature of 60o C for 20 minutes following which they were left to cool and subjected to centrifugation at 2500 rpm for 10 minutes and the resultant supernatants were used to analyse the antimicrobial efficacy.7
 |
Figure 1a: Dried pomegranate pericarp;b: Pomegranate pericarp powder. |
The antimicrobial activity of PPE was assessed using disc inhibition zone method. S.mutans was first isolated from saliva by inoculation on Mitis Salivarius Bacitracin agar and PPE was loaded on the sterile filter paper discs at a concentration of 25, 50, 75 and 100mg/ml, respectively. Filter paper disc dipped in 0.2% chlorhexidine was taken as positive control and distilled water as negative control. S.mutans streaked agar plates impregnated with discs were incubated in anaerobic jar at 37°C for about 24 hrs. The zone of inhibition was assessed by measuring the diameter of inhibited growth [Figure II]. Broth dilution method was adopted to determine minimum inhibitory concentration (MIC) of the active extract. The lowest concentration of extract resulting in bacterial density lower than 300 colonies per plate was determined as MIC. As there was no bacterial colony growth at all the three concentrations (50, 75, 100 mg/ml) of PPE mouthwash, the lowest concentration i.e., 50mg/ml was taken as MIC and was used to prepare the mouth rinse without adding any sweeteners.
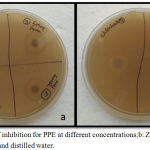 |
Figure 2a: Zone of inhibition for PPE at different concentrations;b: Zone of inhibition for chlorhexidine and distilled water. |
A total of two hundred children between the age group of 6-12 years who were following a routine oral hygiene practice with DMFT score ≥ 4 were screened without sex predilection. Subjects with draining abscess, sinus, cellulitis or any other conditions that require emergency dental treatment and patients with history of recent antibiotic usage (atleast for past 1 month) were excluded from the study. After explaining the test procedure for the forty two children who have fulfilled the inclusion criteria, only thirty parents have gave their consent to participate in the study voluntarily. Further these children were randomly divided into three groups depending upon the mouth rinse used – group I: PPE mouth rinse (experimental); group II: 0.2% chlorhexidine mouth rinse (positive control) and group III: Distilled water (negative control) with ten subjects in each group.
Salivary samples were collected in the morning in order to eliminate any bias in the concentration of saliva due to circadian rhythm. Following an initial swallow, about 1 ml of unstimulated saliva was collected in a sterile vial by instructing the children to drool for 2 minutes. Each child in their respective group was given 5ml of mouth rinse and asked to squish for about one minute. The same procedure was followed for salivary sample collection after 5 minutes following mouth rinsing. The collected samples were transported in an icebox within 2 hours to maintain the viability of microorganisms.
The collected saliva was inoculated on Mutans Sanguis agar and the plates were incubated in an anaerobic jar for 48 hours followed by bacterial count using conventional plate count method [Figure III].
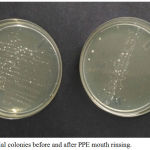 |
Figure 3: Bacterial colonies before and after PPE mouth rinsing. |
The whole procedure was conducted by a single investigator and the scores were recorded. To avoid bias in the results, a second investigator who was unaware of the prior results randomly evaluated the agar plates. As the inter examiner variability was not significant (P value < 0.5), the scores given by the first investigator were only considered. The values thus obtained were tabulated and subjected to statistical analysis using Wilcoxon signed rank test and Mann-Whitney U test.
Results
Intra group comparison in S.mutans count before and after mouth rinsing revealed significant decrease in number of S.mutans colony count in groups I and II (P=0.001). Nevertheless, this reduction was not statistically significant in group III (P=1) [Table I].
Table 1: Intragroup comparison of salivary S.mutans count before and after mouth rinsing (in 103 CFU/ml).
| Group | Before IQR
(in 103CFU/ml) |
After IQR
(in 103CFU/ml) |
P-value |
| I | 383 | 218 | 0.005* |
| II | 350 | 203 | 0.005* |
| III | 350 | 375 | 1 |
Wilcoxon signed rank test
*Statistically highly significant if P≤0.01, IQR: Interquartile range
Intergroup comparison of salivary S.mutans count showed significant decrease in colony count between groups I and III; II and III (P=0.001). However, no statistical significant difference was observed when groups I and II were compared (P=0.48) [Table II].
Table 2: Intergroup comparison of difference in salivary S.mutans count before and after mouth rinsing (in 103 CFU/ml).
| Inter group comparison of difference (after – before count) in IQR | P-value |
| I(285) Vs II(308) | 0.48 |
| I(285) Vs III(105) | 0.001* |
| II(308) Vs III(105) | 0.001* |
Mann-Whitney U test
*Statistically highly significant if P≤0.01, IQR: Interquartile range
Discussion
Epidemiological studies showed that the prevention of dental caries was done by inhibiting plaque biofilm formation or removing plaque from the teeth that enhances oral hygiene. Common preventive strategies of dental caries are mechanical cleansing techniques such as regular brushing and flossing; use of systemic and topical fluorides; dietary modifications include altering frequency of sugar intake, use of sugar substitutes, fissure sealants, antimicrobial agents in mouth washes and probiotics.8Among these, use of topical antimicrobial agents such as mouth rinses minimize caries risk by reducing the number of S.mutans in the mouth there by altering the oral environment.9
A variety of synthetic mouth washes containing Chlorhexidine, Triclosan and Cetylpyridinium chloride are available in the market. Over a period of last 40 years, chlorhexidine has been thoroughly investigated and successfully used as antiplaque agent in dental practice. [10] It is a synthetic bisbiguanide which is positively charged showing high affinity for negative ions found in the cell membrane of the microorganisms. It indirectly affects the enzymatic function of dehydrogenase and adenosine triphosphatase present in the cell wall of bacteria resulting in disruption of cell membrane leading to cell death. Proposed mechanism of caries inhibition is by interfering with the metabolic activity of S.mutans, particularly inhibition of phosphonyl pyruvate enzyme.11
Chlorhexidine has high substantivity of 12 hours which is attributed to its controlled release system regulated by beta cyclodextrine. Greater the amount of beta cyclodextrine, the more progressive release of chlorhexidine.4 In the present study chlorhexidine was taken as positive control as it was considered to be gold standard anti plaque mouth ri
Epidemiological studies showed that the prevention of dental caries was done by inhibiting plaque biofilm formation or removing plaque from the teeth that enhances oral hygiene. Common preventive strategies of dental caries are mechanical cleansing techniques such as regular brushing and flossing; use of systemic and topical fluorides; dietary modifications include altering frequency of sugar intake, use of sugar substitutes, fissure sealants, antimicrobial agents in mouth washes and probiotics.8Among these, use of topical antimicrobial agents such as mouth rinses minimize caries risk by reducing the number of S.mutans in the mouth there by altering the oral environment.9
A variety of synthetic mouthwashes containing Chlorhexidine, Triclosan and Cetylpyridinium chloride are available in the market. Over a period of last 40 years, chlorhexidine has been thoroughly investigated and successfully used as antiplaque agent in dental practice.10 It is a synthetic bisbiguanide which is positively charged showing high affinity for negative ions found in the cell membrane of the microorganisms. It indirectly affects the enzymatic function of dehydrogenase and adenosine triphosphatase present in the cell wall of bacteria resulting in disruption of cell membrane leading to cell death. Proposed mechanism of caries inhibition is by interfering with the metabolic activity of S.mutans, particularly inhibition of phosphonyl pyruvate enzyme.11
Chlorhexidine has high substantivity of 12 hours which is attributed to its controlled release system regulated by beta cyclodextrine. Greater the amount of beta cyclodextrine, the more progressive release of chlorhexidine.4 In the present study chlorhexidine was taken as positive control as it was considered to be gold standard anti plaque mouth rinse due to its prolonged broad spectrum antimicrobial activity. However certain local side effects were reported with its long term usage. 12
To overcome these side effects, researchers are shifting their attention to herbal remedies to fight against microbial infections. Since plant extracts were known to be a good source of new antimicrobial agents, efforts have been made for development of alternate mouth wash from natural products which were anticipated to be safer, easily available and substitute standard pharmaceutical remedies.
Pomegranate fruit is currently finding important applications in the field of dental health due to its consumption in ancient cultures for its medicinal purposes without adverse effects or toxicity. There are several in vitro studies determining the antimicrobial activity of Pomegranate extract against S.mutans but very few clinical studies were conducted to prove its efficacy against dental caries. Thus PPE was selected in the present study to determine its clinical usefulness as anti caries mouth rinse.
Pomegranate pericarp contains different bioactive compounds like phenolics, flavonoids, proanthocyanidine compounds, minerals such as potassium, nitrogen, sodium and complex polysaccharides. Consuming pomegranate pericarp was considered beneficial for treatment of colic, colitis, menorrhagia, oxyuriasis, headache, diuretic, acne, piles, allergic dermatitis and treatment of oral diseases.2
Pomegranate fruit has many properties which include antimicrobial, anti-oxidant, anti-inflammatory, anti-mutagenic, anti-carcinogenic and inhibitory effect on invasion/motility, cell cycle arrest and apoptosis.13
The main compounds responsible for most of the beneficial properties of Pomegranate pericarp are phenolic compounds like ellagitannins and flavonoids. Chemically phenolic acids are defined as substances that possess an aromatic ring bound to one or more hydrogenated substituent.
Eating Pomegranate as a food could place antibacterial and antioxidant agents into the mouth and gum areas. On the other hand, better oral exposure to these agents could come from more direct and chronic exposure with active agents, such as mouth rinses. This is thought to occur due to the fact that the oral tissue would directly be exposed to polyphenols, which would subsequently get activated by enzymes, thereby destroying pathogenic bacteria.2 Hence an approach has been tried out in the present study to use PPE as mouth rinse.
In the current study S.mutans was isolated using Mitis Salivarius Bacitracin (MSB) agar as suggested by Gold et al. (1973)14 who stated that MSB agar can be used as selective medium for isolating S.mutans from saliva.
Broth dilution assay, Agar dilution method, Disc diffusion method, Cup plate method and Ditch plate method are used to assess the antimicrobial activity of any natural or synthetic agent. In the present study, disc diffusion method and broth dilution assay were followed as these methods were considered as standard and reliable.15 Furthermore these methods involves direct contact of the tested substances with the microbial cultures, which is important for the evaluation of mouth rinses.
In a study conducted by Aldhaher et al (2015)1 the MIC of PPE was 15mg/ml. However, in this study it was 50mg/ml. This difference in the results may be attributed to the difference in the type of extract used and method of extract preparation. In the current study, aqueous extract was prepared rather than alcoholic extracts because of its easy availability and highest extraction capacity with water followed by methanol and ethanol. This is due to the relative polar nature of polyphenols in pomegranate and they are strongly soluble in polar solvents like water rather than non-polar solvents such as alcohol.16
The aqueous extract used in this contemporary study was prepared at 60oc temperature for 20 minutes. This procedure was followed according to the findings by Wissam et al (2012)17 who stated that, there is effective extraction of polyphenols and PA at 60oc temperature using water as a solvent; however temperature above 70o c and time longer than 30 minutes may lead to possible polymerization of flavonoids leading to loss of phenolic compounds.
Results of the present study showed significant reduction in salivary S.mutans count with PPE compared to distilled water, whereas no significant difference was noticed with chlorhexidine group. This implies that pomegranate mouth rinse is equally efficacious with chlorhexidine mouth rinse. The possible reason for this is due to the presence of tannins, which crosses bacterial cell wall and precipitate proteins through complex formation, increase bacterial lysis and impede bacterial adhesion by suppression of enzymes like glucosyl transferase which plays an important role in adhesion of S.mutans to tooth surface. [6] According to Machado et al. (2002) 18 ellagitannin-punicalgin is thought to be the primary constituent involved in the antimicrobial effect of pomegranate pericarp.
Similar results were noted by Smruti et al. (2011)19 who compared antiplaque efficacy of pomegranate mouth rinse against chlorhexidine. This study also concluded that pomegranate mouth rinse could be explored as a long-term anti-plaque rinse with prophylactic benefits.
The data obtained with the mouthwash of Punica granatum on S.mutans are consistent with the results shown in a clinical study conducted by Umar et al.(2016)20 who stated that pomegranate mouth rinse may be used as an adjunct to prevent dental caries and maintain good oral hygiene.
There are certain limitations in the use of plant extracts as mouth rinse when compared to synthetic mouth rinses as its preparation is time consuming, need of elaborate apparatus to isolate and characterise active molecules and limited shelf life. The isolation of active components faces many other challenges like inconsistency of source material, obscurity in isolating active components and cost of extraction.
However to consider the clinical applicability of this study certain issues have to be addressed, which include – appropriate concentration of mouth wash to be used, cost effectiveness, addition of preservatives for better shelf life, addition of colouring agents to improve acceptability by children, addition of flavouring agents for better palatability and its long term effectiveness as anti caries mouth rinse on large sample group.
Conclusion
The results of this study gives an inference that both PPE and chlorhexidine mouth rinse possess remarkable antimicrobial activity against S.mutans. Hence PPE mouth rinse may be used as an alternative to chlorhexidine and also as an adjunct to conventional tooth brushing for prevention of dental caries and maintenance of oral hygiene in children.
Acknowledgement
I take this opportunity to whole heartedly thank and express my sincere gratitude to Dr. Padmaja, Dr. Madhav, Assistant Professors, Department of Microbiology and Dr.Charan Das, Professor & Head, Department of Pharmacology for their continuous support and permission to use the facilities of the NRI medical college for the study. I would like to sincerely thank Hanumanth, Biostatistician for his help in statistics.
I would like to sincerely thank Karuna, Lab assistant, Department of microbiology for her indispensable and timely help.
References
- Leite S. J. O., Oliveira F. M., Almeida L. M. S., Gusmao M. A. N., Chedier L. M., Vasconcelos E. G et al. In Vitro assessment of the antimicrobial effects of pomegranate (Punica granatum ) pericarp decoction on saliva samples. Rev. Cienc. Farm. Basica. Apl. 2014;35(1):25-28.
- Narayan T., Deshpande S., Jha A., Ramprasad V. P. Punica granatum (Pomegranate) fruit and its relevance in oral hygiene. IOSR Journal Of Dental and Medical Sciences. 2014;13(8):29-34.
CrossRef - Bhat S. S., Hegde K. S., Farha M. Effect of pomegranate extract mouth rinse on salivary pH and streptococcus mutans counts in children: An In Vivo Study. International Journal of Research in Dentistry. 2014;4(1):12-19.
- Sajjan P., Laxminarayan N., Kar P. P., Sajjanar M. Chlorhexidine as an antimicrobial agent in dentistry – A review. Journal of Oral Health and Dental Management. 2016;15(2):93-100.
- Mehta V. V., Rajesh G., Rao A., Shenoy R., Pai M. B. H. Antimicrobial efficacy of punica granatum mesocarp, nelumbo nucifera leaf, psidium guajava leaf and coffea canephora extract on common oral pathogens. An In Vitro J. Clin. Diagn. Res. 2014;8(7):65-68.
- Subramaniam P., Dwivedi S., Uma E., Girishbabu K. L. Effect of pomegranate and aloe vera extract on streptococcus mutans. An In Vitro Dent.Hypotheses. 2012;3(3):99-105.
CrossRef - Wissam Z., Ghada B., Wassim A., Warid K. Effective extraction of polyphenols and proanthocyanidins from pomegranate’s pericarp. I J. Pharm. Pharm. Sci. 2012;4(3):675-682.
- Daboor S. M., Masood F. S. S., Al-Azab M. S., Nori E. E. A review on streptococcus mutans with its diseases dental caries, dental plaque and endocarditis. Indian. J. Microbiol. Res. 2015;2(2):76-82.
- Bhardwaj P., Krishnappa S. Various approaches for prevention of dental caries with emphasis on probiotics: A review. IOSR Journal of Dental and Medical Sciences. 2014;13(2):62-67.
CrossRef - Emilson C. G. Potential efficacy of chlorhexidine against mutans streptococci and human dental caries. Dent. Res. 1994;73(3):682-689.
CrossRef - Balagopal S., Arjunkumar R. Chlorhexidine: The gold standard antiplaque agent. J. Pharm. Sci & Res. 2013;5(12):270-274.
- Flotra L., Gjermo P., Rölla G., Waerhaug J. Side effects of chlorhexidine mouth washes. J. Dent. Res. 1971;79(2):119-125.
- Rahimi H. R., Arastoob M., Ostada S. N. A comprehensive review of punica granatum (pomegranate) properties in toxicological, pharmacological, cellular and molecular biology researches. Iranian Journal of Pharmaceutical Research. 2012;11(2):385-400.
- Gold G., Jordan H. V., Houte J. V. A selective medium for streptococcus mutans. Arch. Oral. Bid. 1973;18(11):1357-1364.
- Parkar S. M., Thakkar P., Shah K. Antimicrobial activity of four commercially available mouthwashes against Streptococcus mutans. An In Vitro Univ. Res. J. Dent. 2013;3(3):108-112.
- Al-Rawahi A. S., Rahman S., Guizani N., Essa M. M. Chemical composition, water sorption isotherm and phenolic contents in fresh and dried pomegranate pericarps. Drying. Technol. 2013;31(3):257-263.
CrossRef - Wissam Z., Ghada B., Wassim A., Warid K. Effective extraction of polyphenols and proanthocyanidins from pomegranate’s pericarp. I J. Pharm. Pharm. Sci. 2012;4(3):675-682.
- Machado T. B., Leal I. C. R., Amaral A. C. F., Santos K. R. N., Silva M. G., Kuster R. M. Antimicrobial ellagitannin of punica granatum J. Braz. Chem. Soc. 2002;13(5):606-610.
CrossRef - Smruti J. B., Anirudh B. A., Silvia V. R., Srinath L. T. The antiplaque efficacy of pomegranate mouthrinse. Int. 2011;42(1):29-36.
- Umar D., Dilshad B., Farhan M., Ali A., Baroudi K. The effect of pomegranate mouth rinse on Streptococcus mutans count and salivary pH: An In Vivo study. J. Adv. Pharm. Technol. Res. 2016;7(1):13-16.
CrossRef

