
Divya Rao1, M. R. Dhakshaini2, Ameet Kurthukoti3 and Vidya G. Doddawad4
1Department of Health System Management Studies, JSS University, Mysuru.
2Department of Prosthodontics, Vice Principal, JSS Dental College, JSS University, Mysuru.
3Dental Health Officer, Department of Health and Family Welfare, Government of Karnataka.
4Department of Oral Pathology and Microbiology, JSS Dental College, JSS University, Mysuru.
Corresponding Author E-mail: divyaraobj@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1543
Abstract
Biomedical waste (BMW) generated in our nation on a day to day basis is immense and contains infectious and hazardous materials. It is crucial on the part of the employees to know the hazards of the biomedical waste in the work environment and make its disposition effective and in a scientific manner. It is critical that the different professionals engaged in the healthcare sector have adequate Knowledge, Attitudes and Practices (KAP) with respect to biomedical waste management. Many studies across the country have shown that there are still deficiencies in the KAP of the employees in the organizations and hence it is necessary to make the appraisal of the same. To ascertain the levels of and the expanse of gaps in knowledge, attitudes and practices among doctors, post graduates, staff nurses, laboratory technicians and house-keeping staffs in a tertiary care teaching hospital in Mysuru, Karnataka. A cross sectional study was carried out using questionnaire as the study tool among the health care professionals in a tertiary care teaching hospital. The study demonstrated gaps in the knowledge amongst all the cadres of the study respondents. The knowledge in relation to BMW Management including the hospital BMW protocols was more desirable among doctors, but practical facets were better in nurses and the lab technicians. Knowledge, Attitude and Practice amongst the different cadres of staff members were found to be significant statistically.
Keywords
Attitude; Biomedical Waste; Healthcare personnel; Knowledge; Practice
Download this article as:| Copy the following to cite this article: Rao D, Dhakshaini M. R, Kurthukoti A, Doddawad V. G. Biomedical Waste Management: A Study on Assessment of Knowledge, Attitude and Practices Among Health Care Professionals in a Tertiary Care Teaching Hospital. Biomed Pharmacol J 2018;11(3). |
| Copy the following to cite this URL: Rao D, Dhakshaini M. R, Kurthukoti A, Doddawad V. G. Biomedical Waste Management: A Study on Assessment of Knowledge, Attitude and Practices Among Health Care Professionals in a Tertiary Care Teaching Hospital. Biomed Pharmacol J 2018;11(3). Available from: http://biomedpharmajournal.org/?p=22092 |
Introduction
Health care waste is a unique category of waste by the quality of its composition, source of generation, its hazardous nature and the need for appropriate protection during handling, treatment and disposal. Mismanagement of the waste affects not only the generators, operators but also the common people too.1
‘Bio-medical waste’ (BMW) means any solid and/or liquid waste including its container and any intermediate product, which is generated during the diagnosis, treatment or immunization of human beings or animals or in research pertaining thereto or in the production or testing thereof.2
Due to the increase in the procedures that are carried out at the various health care setups, excessive amounts of waste have been generated at the centers of care.
India approximately generates 2 kg/bed/ day 3 and this biomedical waste encompasses wastes like anatomical waste, cytotoxic wastes, sharps, which when inadequately segregated could cause different kinds of deadly infectious diseases like Human immunodeficiency virus(HIV) hepatitis C and B infections, etc,4 and also cause disruptions in the environment, and adverse impact on ecological balance.5,6
Adequate knowledge amongst the health care employees about the biomedical waste management rules and regulations, and their understanding of segregation, will help in the competent disposal of the waste in their respective organizations.7
Acceptable management of biomedical waste management begins from the initial stage of generation of waste, segregation at the source, storage at the site, disinfection, and transfer to the terminal disposal site plays a critical role in the disposal of waste. Hence adequate knowledge, attitudes and practices of the staff of the health care institutes play a very important role.8,4,9
Teaching institutes play a critical role in the health care setup as it is from these places that the future health care professionals and all those persons involved in the care giving to the community are trained.10
Studies documented from different parts of the country; still convey that there are gaps in the Knowledge, lacunae in the attitudinal component and inconsistency in the practice aspects which are matters of concern among the health care professionals.8,11-15 With this background, the study was carried out to assess the current knowledge, attitude and practices of the health care workers like doctors, post graduates, interns, staff nurses, laboratory technicians and house-keeping staff in a tertiary care teaching hospital with regard to the management of BMW.
Objectives
To assess the levels of knowledge, attitudes and practices among doctors, post graduates, interns, staff nurses, laboratory technicians and house-keeping staff in the different departments of a tertiary care teaching hospital.
To assess the gaps in knowledge, attitudes and practices among these health care workers in the different departments of a tertiary care teaching hospital.
Methodology
Study design
Cross-sectional study.
Study setting
Tertiary care teaching hospital
Study population
Staff working in the different departments of the hospital.
 |
Graph 1
|
Eligibility Criteria
All consenting individuals amongst the different cadres of staff were included into the study. There were 2056 eligible participants, which was taken as the sampling frame.
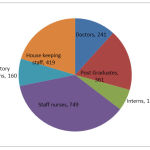 |
Graph 2
|
Sample Size
Expecting that 50% of the study population had precise knowledge (considering the outcome variable) about the rules and legislation of biomedical waste management,16 with an allowable error of 10%, at 95% confidence interval, and accounting for the finite population correction for 2,056 participants, a minimum sample size of 472 was calculated.
Sampling Strategy
The study population was classified according to the different strata based on their designation as doctors, postgraduates (junior residents), interns, staff nurses, laboratory technicians and house-keeping staff. Allocation of the population according to the strata.
| Strata | Participants |
| Doctors | 55 |
| Post Graduates | 83 |
| Interns | 29 |
| Staff Nurses | 172 |
| Laboratory Technicians | 37 |
| House Keeping Staff | 96 |
| Total | 472 |
Ethical Approval
The ethical clearance for the study was obtained from the Institutional Ethics Committee.
Materials and Methods
The tool used for the study was a pre-tested, semi-structured closed ended questionnaire which encompassed 42 questions on Knowledge, Attitudes and Practices.
The questions on knowledge appraised the participant’s knowledge on attributes related to the colour coding and their implications, identification of biomedical hazard symbol, waste categories, and hospital policies for biomedical waste management.
The questions on attitude were related to matters like, was biomedical waste hazardous, its management additional burden on their work or if their appropriate management burden on the finances of the hospital, and also on legislative measures for waste management.
The questions on practice appraised if the study respondents had received any training on biomedical waste management, if they were immunized against hepatitis B and if disinfection of sharps were carried out at the point of generation.
The literature review was done based on which the questionnaire was formulated according to the requirements of the study. The questionnaire was pretested and validated by a post-test and a pilot survey was conducted with a sample of 60 respondents, with representations from the various strata of the study respondents. The study tool consisted of 12 questions assessing the knowledge with yes/no/not sure responses, 10 questions assessing the attitude with agree/disagree/no comment as answers and 20 questions assessing the practices with yes/ no responses.
The participants filled up the self-administered questionnaires without scope for undue help.
The questionnaire was adapted from English to local language by an experienced professional who is involved in translating of health survey questionnaires to accommodate the housekeeping staff. The questionnaire was also back translated to English for checking of possible discrepancies and incorporating if any changes were required. The identity of the study respondents were maintained anonymous at various stages of the study.
Results
The results were evaluated across 3 domains for all the cadres of the study population.
The results are Displayed as Under
Statistical Methods
Data was analysed using MS-Excel and R version 3.4.3. Percentages (with 95% confidence intervals) were calculated and the same are presented graphically. Chi-square test was performed to test the association between the different cadres related to their knowledge, attitude and practices towards BMW
Knowledge Score
The knowledge regarding general information about HCW was assessed, the mean score was highest in doctors (10) followed by nursing staff (9.3) and least in housekeeping staff (7.5). This is found to be statistically significant.
Table 1: The participant’s knowledge on biomedical waste management.
| CADRE | Yes(%) (95% CI) | No(%) (95% CI) | Not sure(%) (95% CI) |
| Doctors | 82 (79,85) | 13 (11,16) | 5 (3,6) |
| Post Graduates | 69 (65,74) | 22 (18,26) | 9 (6,13) |
| Interns | 64(58,70) | 12 (8,16) | 24 (19,30) |
| Nursing | 74 (72,77) | 18 (16,21) | 8 (8,9) |
| Technicians | 71 (62,79) | 16 (11,25) | 13 (7,20) |
| House Keeping Class IV | 64 (59,69) | 25 (21,30) | 11 (8,14) |
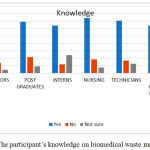 |
Figure 1: The participant’s knowledge on biomedical waste management.
|
Overall, the study respondents showed satisfactory knowledge regarding biomedical waste management. The knowledge about BMW among doctors was the distinctively better, followed by that of nurses, technicians, post graduates, interns and housekeeping staff (in order). The gaps in knowledge were in the areas regarding the fate of the waste after it was segregated, and as well as who was the regulator for the safe transportation of biomedical waste from the hospital.
Table 2: The participant’s attitudes towards biomedical waste management.
| CADRE | Yes(%) (95% CI) | No(%) (95% CI) | Not sure(%) (95% CI) |
| Doctors | 79 (75,82) | 17 (14,21) | 4 (2,6) |
| Post Graduates | 74 (69,78) | 18 (14,22) | 8 (0.5,11) |
| Interns | 79 (73,84) | 15 (10,21) | 6 (3,10) |
| Nursing | 82 (79,84) | 17 (15,19) | 1 (0.5,2) |
| Technicians | 71 (61,79) | 19 (12,28) | 10 (0.5,18) |
| House Keeping Class IV | 63 (57,68) | 32 (27,38) | 5 (3,8) |
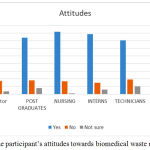 |
Figure 2: The participant’s attitudes towards biomedical waste management.
|
The mean attitude score was 9.20 for the nurses and 9.18 out of 10 for the doctors. Favourable attitude was shown by most of the study respondents towards biomedical waste management. The best attitudes were displayed by the nurses showed, subsequently by doctors, interns, postgraduates, the laboratory technicians, and house keeping staff (in order). It was concerning that the lacuna in this domain was that biomedical waste management was considered as additional burden on work.
Table 3: The participant’s practices regarding biomedical waste management.
| CADRE | Yes(%) (95% CI) | No(%) (95% CI) | Not sure(%) (95% CI) | Others |
| Doctors | 69 (64,72) | 10 (8,13) | 15 (13,17) | 6 (5,8) |
| Post Graduates | 52 (48,55) | 20 (18,24) | 24 (22,28) | 4 (2,5) |
| Interns | 54 (49,59) | 16 (13,21) | 23 (19,28) | 7 (4,9) |
| Nursing | 83 (79,85) | 11 (9,13) | 2 (1,3) | 4 (3,5) |
| Technicians | 66 (59,73) | 16 (20,32) | 15 (11,21) | 3 (1,6) |
| House Keeping Class IV | 72 (69,76) | 22 (19,25) | 4 (2,5) | 2 (1,4) |
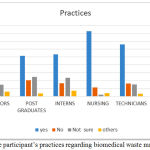 |
Figure 3: The participant’s practices regarding biomedical waste management.
|
The mean practice score was 17.30 for the nurses and 16.50 for the housekeeping staff and 15.27out of 20 for the doctors, in the study. Though greater number of the study respondents displayed favourable biomedical waste management practices, it was noted that the nurses had the best practices, followed house keeping staff, doctors, technicians, interns and junior residents (in order). It was noted that the staff ware following the preventive measures of immunisation against Hepatitis B, and also routine health check-ups were conducted for the staff. Explicit training on BMW management was desired by most of the staff.
Chi-Square Test
The null hypothesis which was to be tested here was “The two attributes were independent”. Here three hypotheses were there to be tested:
Cadre and knowledge are independent.
(Chi-square = 160.8, Degrees of freedom=10, p-value < 0.0001)
Cadre and attitudes are independent.
(Chi-square = 95.6, Degrees of freedom=10, p-value < 0.0001)
Cadre and practices are independent.
(Chi-square = 538.45, Degrees of freedom=15, p-value < 0.0001)
Discussion
The present cross-sectional study recognized certain inadequacies in the knowledge component amongst the different cadres of health care workers, though greater than 50% of the study respondents, across cadres, demonstrated satisfactory or good knowledge, attitudes and practices. The knowledge component of the doctors was more desirable compared to their practices whereas visa versa was true for nurses and lab technicians. The knowledge component was low amongst the housekeeping staff; which was identical to the results from other similar studies conducted previously.10,13,16
The attitude towards BMW management of housekeeping staff was low. Low level of knowledge was mainly attributed to new staff coming on rotation to the hospital and also to comparably low educational levels of the housekeeping staff. Training of all cadres of staff will help in the analytical evaluations for suitable and applicable management of biomedical waste.10,13,16
The practice of recapping the needles was very low across cadres. Recapping of needles is one of the important risk factor for needle stick injuries; the prevalence was very low in the organization. This may be associated to the awareness of the staff and also due to the adequate number of needle cutters in the various patient care areas of the hospital.
Higher practice scores found in the house keeping staff and nursing staff in the present study may be due to higher responsibilities assigned to them in handling of BMW which was similar to findings of previous studies.1,17 Overall 8.1 % of the study respondents attended the external training programmes on BMW management on their own accord, but others too (~ 59%) of them communicated their willingness to do the same if opportunities arose in the future.10,13,16
Conclusions
Overall, the knowledge, attitudes and practices towards biomedical waste management among the study respondents was satisfactory.
Knowledge, attitudes and practices toward biomedical waste management were better among the nurses and doctors than the other cadre of staff.
Knowledge, Attitudes and Practices of the study respondents are dependent on the cadre that they belong too.
Summary
This study was a modest attempt to evaluate the KAP of the health care workers towards BMW. We recommend further studies on a larger stratum across hospitals to evaluate the awareness of health care workers towards BMW.
Recommendations
Training programs need to focus on empowering the healthcare professionals on biomedical waste management with broad scope and practical knowledge in all aspects. The ethical requirements and the institutional level policies form the directional pathway for the practical components in the organization. The right practices and other activities of BMW management and its ramifications in the form of avoiding of injuries, importance of vaccinations and following of universal precautions can be achieved when adequately supported by IEC (information, education and communication) strategies like handouts, stickers, charts, celebrations of various days like hand hygiene day and other days etc can help in bettering the practices of the employees of the organizations. Training the staff with checklists and regular inspections can bring about accountability in the staff.
All health care professionals regardless of their designation, experience and qualification , designation must be included in these interventions, so that it can avoid cross infections among the professionals and patients in the health care sector.
Conflicts of Interest
There is no conflicts of interest.
References
- Kumar P.V.A.G, Kapate R et al, Knowledge, Attitude, and Practices of Health Care Waste Management amongst Staff of Nursing Homes of Gulbarga City. Journal of Pharmaceutical and Biomedical Sciences. 2012;19(19)1-3.
- Sharma A.K. Biomedical Waste (Management and Handling) Rules. First edition. Bhopal. Suvidha Law House. 12.
- Patil A.D, Shekdar A.V. Health-care waste management in India. J Environ Manage. 2001;63:211-20.
CrossRef - Nath P.A, Prashanthini V, Visvanathan C. Healthcare waste management in Asia. Waste Management. 2010;30:154-61.
CrossRef - Lakshmikantha H. Report on waste dump sites near Bangalore. Waste management. 2006;26(6):640-50.
CrossRef - Misra V, Pandey S.D. Hazardous waste, impact on health and environment for development of better waste management strategies in future in India. Environment International. 2005;31:417-31.
CrossRef - Kini B.S, Kumar , Kumar S, Reddy M, Nabar A.S, Kamath V.G, Kamath A, Eshwari K. Knowledge, Attitudes and Practices regarding Biomedical Waste Management among staff of a tertiary healthcare centre in coastal Karnataka. J Pub Health Med Res. 2014;2(1):20-4.
- Pattnaik S, Reddy M.V. Assessment of Municipal Solid Waste management in Puducherry (Pondicherry). India. Resources, Conservation and Recycling. 2010;54:512-20.
CrossRef - Mathur V, Dwivedi S, Hassan M.A, Misra R.P. Knowledge, Attitude, and Practices about Biomedical Waste Management among Healthcare Personnel: A Cross-sectional Study. Indian J Community Med. 2011; 36:143-5.
CrossRef - Radha R. Assessment of existing knowledge, attitude, and practices regarding biomedical waste management among the health care workers in a tertiary care rural hospital. Int J Health Sci Res. 2012;2(7):14-19.
- Verma L.K, Mani S, Sinha N, Rana S. Biomedical waste management in nursing homes and smaller hospitals around Delhi. Waste Management. 2008;28:2723-34.
CrossRef - Kumar S, Bhattacharyya J.K, Vaidya A.N, Chakrabarti T, Devotta S, Akolkar A.B. Assessment of the status of solid waste management in metro cities, state capitals, class I cities, and class II towns in India: An insight. Waste Management. 2009;29:883-95.
CrossRef - Pandit N.B, Mehta H.K, Kartha G.P, Choudhary S.k. Management of biomedical waste: Awareness and practices in a district of Gujarat. Indian J Public Health. 2005;49:245-7.
- Rao P.H. Report: Hospital waste management – awareness and practices: A study of three states in India. Waste Manage Res. 2008;26:297-303.
CrossRef - Kishore J, Goel P, Sagar B, Joshi T.K. Awareness about biomedical waste management and infection control among dentists of a teaching hospital in New Delhi, India. Indian J Dent Res. 2000;11:157-61.
- Saini S, Nagarajan S.S, Sarma R.K. Knowledge, Attitude and Practices of Bio-Medical Waste Management Amongst Staff of a Tertiary Level Hospital in India. Journal of the Academy of Hospital Administration. 2005;17(2).
- Yadavannavar M.C, Berad A.S, Jagirdar P.B. Biomedical waste management: A study of knowledge, attitude, and practices in a tertiary health care institution in Bijapur. Indian Journal of Community Medicine. 2010;35(1):170-71.
CrossRef

