
Manuscript accepted on :16 May 2018
Published online on: 02-06-2018
Plagiarism Check: Yes
I. Gusti Lanang Sidiartha1, I. Gusti Ngurah Suarba1, Dyah Kanya Wati1, Eka Widyadharma2 and Mahadewa Tjokorda3
1Department of Child Health, Faculty of Medicine, Udayana Universit- Sanglah Hospital, Bali, Indonesia.
2Department of Neurology, Faculty of Medicine, Udayana University- Sanglah Hospital, Bali, Indonesia.
3Department of Neurosurgery, Faculty of Medicine, Udayana University-Sanglah Hospital, Bali, Indonesia.
Corresponding Author E-mail: tjokmahadewa@unud.ac.id
DOI : https://dx.doi.org/10.13005/bpj/1442
Abstract
Antiepileptic drugs (AEDs) are widely used to control seizure in children with epilepsy. These drugs are commonly used for a long time and are related with abnormalities of bone metabolism. This study investigates the correlation between calcium serum levels and bone mineral density (BMD) with duration of AEDs treatment. Thirty children with epilepsy on AEDs treatment for more than six months were evaluated. Data calcium serum, BMD, and duration of treatment were collected on the same time. Calcium serum and BMD was examined using immunoradiometric assay and dual energy X-ray, respectively. Pearson Correlation test was used to analyze the correlation between variable with significances if P value < 0.05. The subjects included 12 girls and 18 boys with mean age 8.5 years old. Duration of AEDs treatment, calcium serum levels, and BMD were 20.5 months, 9.35 (SD 0.32) mg/dl, and 0.81 (SD 0.07) g/cm2, respectively. It was moderate correlation between calcium serum and duration of treatment (r=-0.493; P=0.006). It was weak correlation between BMD and duration of treatment (r=-0.251; P=0.181). Duration of AEDs treatment in children with epilepsy correlated with calcium serum levels and BMD
Keywords
AEDs; BMD; Calcium; Epilepsy
Download this article as:| Copy the following to cite this article: Sidiartha I. G. L, Suarba I. G. N, Wati D. K, Widyadharma E, Tjokorda M. Correlation Between Calcium Serum Levels and Bone Mineral Density with Duration of Antiepileptic Drugs Uses in Children with Epilepsy. Biomed Pharmacol J 2018;11(2). |
| Copy the following to cite this URL: Sidiartha I. G. L, Suarba I. G. N, Wati D. K, Widyadharma E, Tjokorda M. Correlation Between Calcium Serum Levels and Bone Mineral Density with Duration of Antiepileptic Drugs Uses in Children with Epilepsy. Biomed Pharmacol J 2018;11(2). Available from: http://biomedpharmajournal.org/?p=20556 |
Introduction
Antiepileptic drugs (AEDs) include sodium valproate (VPA), phenobarbitone (PB), phenytoin (DPH), and carbamazepine (CBZ) is widely used to control seizure in epilepsy. These drugs are commonly used for a long time. Recently, the longer uses of AEDs are related in mineral and bone metabolism disorders. Its can cause osteoporosis and spontaneous bone fractures.1-3
The drugs such as CBZ, DPH, and PB are known inducing the activity of hepatic oxidase throughout the enzyme of microsomal (P450). They influence metabolism of mineral and bone by increasing vitamin D metabolism, that causing deficiency of vitamin D (VDD).4-6 This VDD inhibit intestinal calcium transport and absorption, that causing hypocalcaemia.7 The other mechanism of the AEDs is act directly on bone cells that influence bone formation and resorption. Both mechanisms associated with reduce of bone mineral density.7-10 Other AEDs such as VPA that is descriptively termed as hepatic noninducers affect bone metabolism by unclear mechanism.
In our pediatric department the most common use of AEDs are VPA, CBZ, DPH, and PB as a single or multiple therapies to control seizure in pediatric epilepsy. Until now, there is no routine investigation of most common abnormalities of laboratory in relation to chronic use of AEDs such as hypocalcaemia, hypophosphatemia, increased of alkaline phosphatase (AP), increased parathyroid hormone (PTH), and decreased 25-hydroxy vitamin D (25OHD) in our department. The study evaluates the correlation of long-term uses of AEDs with calcium serum levels and BMD in epileptic children.
Material and Methods
This correlative study was done to analyses 30 children aged 1-10 years old with epilepsy who were controlled in outpatient Pediatric Neurologic Clinic of Sanglah Hospital Denpasar Bali, between July and September 2016. Ethic Committee of Udayana University – Sanglah Hospital Denpasar Bali, approved this study and all subjects were signed in the informed consent.
Inclusion criteria were children aged 1-10 years old; use of first line AEDs (VPA, CBZ, DPH or PB) for 6 months or more; and agreed participating in this study. Exclusion criteria were epileptic children with cerebral palsy; receive calcium and vitamin D supplementation during therapy; severe malnutrition; and suffer from the illness that were known affecting bone metabolism including hepatic, hematologic, rheumatologic, renal, parathyroid, musculo-skeletal, thyroid, and gastrointestinal disorders or using medications that were known affecting bone turnover such as glucocorticoids, bisphosphonates, thiazides, anticoagulants, or steroids.
Demographic data of all subjects such as age, body weight, body height, gender, and history of the disease previously, history of the drugs consumption, history of the epilepsy and its therapy were collected from medical record. Nutritional status was determined using the WHO growth standard. Severe malnutrition was defined if weight-for height z scores less than -3SD. On the same day, blood samples and radiologic imaging were evaluated for measurement of calcium levels and bone mineral density. Levels of calcium serum was measured using immunoradiometric assay Roche/Hitachi Cobas c 311/501 analyzer and scan dual-energy X-ray (C.B.D.DEXA) GE Healthcare en CORE 2007 for measurement bone mineral density. Both laboratory and imaging measurement were done in Clinical Pathology and Radiology Department of Sanglah General Hospital Denpasar Bali.
The data were analyzed using SPSS 20. The variables of duration of AEDs used, calcium serum levels, and bone mineral density were analyzed initially by normality test of Shapiro Wilk. The Pearson correlation test was done between two continuous variables with normal distribution of the data. Significantly suggested if P value < 0.05.
Results
Fifty-five children with epilepsy came to outpatient of Pediatric Neurology Clinic Sanglah Hospital during study period. Twenty-five children were excluded. Among of them, ten children had cerebral palsy, five children had hypothyroid congenital, three children had puberty, five children used AEDs less than 6 months, and two children refused to participate. The characteristics of subjects are showed in Table 1.
Figure 1a and Figure 1b showed the correlation between duration use of AEDs and calcium serum levels and BMD. Duration use of AEDs showed moderate negative correlation with calcium serum levels (r = -0.493; P = 0.006), while duration use of AEDs showed negative correlation with BMD (r=-0.251; P=0.181).
Discussion
We have evaluated 30 children (18 boys and 12 girls) with epilepsy with their mean of age were 8.5 years old. Most of subjects used single
Table 1: Characteristics subjects
| Characteristic | Total |
| N=30 | |
| Gender, boys/girls, n | 18/12 |
| Age (y), mean and SD | 8.5 (1.9) |
| Weight (kg), mean and SD | 26.7 (8.1) |
| Height (cm), mean and SD | 125.1 (12.5) |
| Type of epilepsy, general/focal | 17/13 |
| Type of AEDs, inducer/non-inducer, n | 24/6 |
| Therapy AEDs, mono/poly-therapy, n | 24/6 |
| Calcium serum (mg/dL), mean (SD) | 9.35 (0.32) |
| BMD (g/cm2), mean (SD) | 0.81 (0.07) |
| Duration of AEDs (mo), median (min-max) | 20.5 (6-84) |
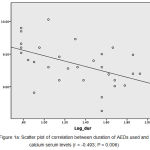 |
Figure 1a: Scatter plot of correlation between duration of AEDs used and calcium serum levels (r = -0.493; P = 0.006) |
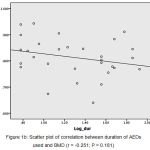 |
Figure 1b: Scatter plot of correlation between duration of AEDs used and BMD (r = -0.251; P = 0.181) |
AEDs, especially enzyme inducers AEDs such as CBZ, DPH, and PB. Its mean that first line AEDs that is classified as an enzyme inducer is commonly used in our department. These results were similar with another study that commonly used enzyme inducer AEDs for the epileptic patients, but mostly on multiple drugs regimens.11 In our department, multidrug AEDs are used if single AEDs cannot control the seizures during three months period of the treatment. In this study only six of 30 subjects received multidrug AEDs. The combination is commonly among enzyme inducer AEDs such as CBZ combine with PB or between enzyme inducer combine with non-enzyme inducer such as CBZ combine with VPA.
Both of enzyme inducer and non-inducer AEDs causing abnormalities of vitamin D metabolism. Many studies have published that serum 25-hydroxyvitamin D concentration is inadequate in children, adolescent, and adults with epilepsy who are treated with AEDs.4-6 Vitamin D is a pro-hormone that is metabolized in the liver and kidney to become an active metabolite.12 Enzyme inducer of AEDs inhibit the conversion of D vitamin in liver cells. Low serum vitamin D levels inhibits absorption of calcium in the intestinal tract and increase resorption of the bone calcium causing hypocalcaemia and low bone mineral density.6,9-11,13
This study found that chronic use of AEDs was significantly having a moderate negative correlation with concentration of calcium serum. It means that the longer use of AEDs the lower levels of calcium serum. Many studies had reported hypocalcaemia in epileptic subjects on AEDs management with incidence varying between 3% and 30%.14-16 The possible mechanisms of AEDs causing hypocalcaemia are stimulate catabolism of D vitamin, inhibits parathyroid hormone to induce calcium mobilization, and decrease dietary calcium absorption.16
Calcium and also D vitamin are an important micronutrient in developing and also maintaining bone health. All children with epilepsy who using AEDs for long time usually related with alteration of bone metabolism with decreased of BMD.8,9,11-13 The enzyme inducer AEDs stimulate hepatic cytochrome P450 to inactivated vitamin D. Inactivated vitamin D decrease calcium absorption in intestinal tract, and causing hypocalcaemia and increase circulating of parathyroid hormone. Parathyroid hormone increase mobilization of calcium from the bone that causing low BMD.14 Unfortunately, our study showed weak negative correlation between duration of the AEDs treatment and bone mineral density and statistically not significant. Our study mostly uses enzyme inducer AEDs, mono-therapy, and median duration of the AEDs treatment is 20.5 months. So the possibility reasoning of these results are mostly mono-therapy and less than 2 years of the AEDs uses.
Conclusion
It could be concluded that chronic use of AEDs having a moderate negative correlation with concentration of calcium serum and weak negative correlation with BMD.
Conflict of Interest
There were no financial supports or relationships between authors and any organisation or professional bodies that could pose any conflict of interest.
Acknowledgements
we would like to thank the pediatric student, Ayu Sinthia Santi for getting the samples and reviewing the records.
References
- Wu F.J, Sheu S.Y, Lin H.C. Osteoporosis is associated with antiepileptic drugs: a population-based study. Epileptic Disord. 2014; 16(3): 333-342.
- Lazzari A.A, Dussault P.M, Manisha T.J, Gagnon D, Baker E, Davis S.A., et al. Prevention of bone loss and vertebral fractures in patients with chronic epilepsy – antiepileptic drug and osteoporosis prevention trial. 2013; 54(11): 1997-2004.
- Nicholas J.M, Ridsdale L, Richardson M.P, Grieve A.P, Gulliford M.C. Fracture risk with use of liver enzyme inducing antiepileptic dugs in people with active epilepsy: Cohort study using the General Practice Research Database. Siezure. 2013; 22: 37-42.
CrossRef - Ramelli V, Ramelli G.P, Lava S.A.G, Siegenthaler G.M, Cantu M, Bianchetti M.G, et al. Vitamin D status among children and adolescents on anticonvulsant drugs in Southern Switzerland. Swiss Med Wkly. 2014;144:1-5.
CrossRef - Teagarden D.L, Meador K.J, Loring D.W. Low vitamin D levels are common in patients with epilepsy. Epilepsy Res. 2014; 108(8): 1352-1356.
CrossRef - Baek J.H. Seo Y.H. Kim G.H. Kim M.K. Eun B.L. Vitamin D levels in children and adolescents with antiepileptic drug treatment. Yonsei Med J. 2014; 55(2): 417-421.
CrossRef - Vera V, Moran J.M, Barros P, Canal-Marcias M.L, Rafael G.B, Carmen C.F., et al. Greater calcium intake is associated with better bone health measured by quantitative ultrasound of the phalanges in pediatric patients treated with anticonvulsant drugs. 2015; 7: 9908-9917.
- Zhang Y, Zheng Y, Zhu J, Zhang J, Zheng Z. Effects of antiepileptic drugs on bone mineral density nd bone metabolism in children: a meta analysis. J Zhejiang Univ-Sci B (Biomed & Biotechnol). 2015; 16(7): 611-621.
- Salimipour H, Kazerooni S, Seyedabadi M, Nabipour I, Nemati R, Iranpour D., et al. Antiepileptic treatment is associated with bone loss: difference in drug type and region of interest. J Nucl Med Technol. 2013; 41: 208-211.
CrossRef - Benicsky S.A, Viken J, Jensen L.T, Andersen N.B. Bone mineral density in adult patients treated with various antiepileptic drugs. 2012; 21: 471-472.
- Kulak C.A.M, Borba V.Z.C, Bilezikian J.P, Silvado C.E, Paola L, Boguszewski C.L. Bone mineral density and serum levels of 25 OH vitamin D in chronic users of antiepileptic drugs. Arq Neuropsiqulatr. 2004; 62: 940-948.
CrossRef - DeLuca H.F. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr. 2004; 80: 1689S-1696S.
CrossRef - Phabphal K, Limapichat K, Sathirapanya P, Setthawatcharawanich S, Leelawattana R, Thammakumpee N., et al. Bone mineral density following long-term use of antiepileptic drugs in a tropical Asian country. Epileptic Disord. 2008; 10: 213-218.
- Pack A.M. The association between antiepileptic drugs and bone disease. Epilepsy Currents. 2003; 3: 91-99.
CrossRef - Richens A. Rowe D.F.J. Disturbance of calcium metabolism by anticonvulsant drugs. Br Med J. 1970; 4: 73-76.
CrossRef - Smith M.V.B, Crofoot K, Rodriguez-Proteau R, Filtz T.M. Effects of phenytoin and carbamazepine on calcium transport in Caco-2 cells. Toxicology in Vitro., 2007; 21: 855-862.
CrossRef

