
Amira M. Zakaria
Biotechnology Research Institute, New campus Ismailia, Egypt.
Corresponding Author E-mail: amirazakaria2013@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1453
Abstract
Serological approaches such as Rose Bengal Test (RBT) and enzyme linked immunosorbent assay (ELISA) are common tests, however they are generally not sensitive or specific enough for diagnosis of Brucella because of cross-reactivity with different bacterial antigens. The work objected to evaluate the sensitivity and specificity of rose Bengal and modified in-house ELISA using IS711 real time PCR as a gold test to detect Brucella in calves sera. Two hundred and thirty (n=230) blood samples were collected from (2-3) years asymptomatic male calves in two Egyptian abattoirs. Rose Bengal test (RBT) and modified in-house ELISA were applied to determine the seroprevalence of brucellosis in abattoirs animals while quantitative Taqman real-time PCRs (RT-PCR) were implemented for the identification of Brucella genus. The overall prevalence of brucellosis was (53.9 %), (75.2 %) and (79.1 %) as determined by ELISA,RBT and RT- PCR assays respectively. Regarding statistical analysis of the reported data and considering real time PCR the gold standard, the RBT recorded a sensitivity of (79.12%) and a specificity of (39.58 %) with an accuracy of (70.87%). While (83.24%) was reported as positive predictive value and (33.33 %) as a negative predictive value. The sensitivity and specificity of ELISA were (55.49%) and (52.08 %) respectively while the accuracy was (54.78%). Positive predictive value and negative predictive value for ELISA were determined as (81.45%) and (23.58 %) respectively. RBT can be routinely used for diagnosis of Brucella as cost effective , more sensitive and accurate test than ELISA However, real time PCR is highly recommend as gold test for identification and differentiation of bovine brucellosis.
Keywords
Brucellosis; ELISA; Rose Bengal Test; Sensitivity; Specificity
Download this article as:| Copy the following to cite this article: Zakaria A. M. Comparative Assessment of Sensitivity and Specificity of Rose Bengal Test and Modified In-House ELISA by using IS711 Taqman Real Time PCR Assay as a Gold Standard for the Diagnosis of Bovine Brucellosis. Biomed Pharmacol J 2018;11(2). |
| Copy the following to cite this URL: Zakaria A. M. Comparative Assessment of Sensitivity and Specificity of Rose Bengal Test and Modified In-House ELISA by using IS711 Taqman Real Time PCR Assay as a Gold Standard for the Diagnosis of Bovine Brucellosis. Biomed Pharmacol J 2018;11(2). Available from: http://biomedpharmajournal.org/?p=20837 |
Introduction
Brucellosis is a global zoonosis induced by bacteria of the genus Brucella, and considered as a crucial public health issue across the world. The great variety of clinical evidences of the human brucellosis makethe diagnosis relatively difficult,1,2,3 This absence of certain symptoms makes it challenging to differentiate brucellosis from numerous febrile diseases that commonly appear in the same regions so that laboratory testing is very important for diagnosis.4 Among these tests, exclusively the isolation of the organism presents an absolute evidence of infection however bacteriological diagnosis is costly and even hazardous. Alternatively, serological tests are simpler to apply and a significant assistance in diagnosis. Direct agglutination, Rose Bengal test, Coombs test and ELISA are the most desired methods for the serological diagnosis of brucellosis.5.6.7
Serological tests are commonly employed to perform several epidemiological researches as well as diagnostic applications, but there is no ideal serological test.8 However, the diagnostic efficiency and discriminative capacity of a test are usually assessed by comparing the sensitivity and specificity of different tests analytically.9 The diagnostic capability of a test could be evaluated by comparison with standard reference test and examined by gold standards.10 Molecular diagnosis of brucellosis by PCR techniques has often been utilized as an additional alternative. Genus-specific PCR assays are relatively inexpensive diagnostic tests for screening with the possibility to recognize the causative agent even with minimal concentrations of DNA,11 The objective of this study was to evaluate diagnostic effectiveness and discriminative power of Rose Bengal Plate Test (RBT), and in-house indirect enzyme linked immunosorbent assay (I-ELISA) tests utilized for diagnosis of bovine brucellosis in Egypt choosing real time PCR as the gold test. This study is amongst a type in the context of field diagnostic test evaluation for bovine brucellosis in Egypt which has considerable importance for disease surveillance and long term control plans.
Material and Methods
Ethical Statement
The protocol for collection of animal materials was approved by districts veterinary and agricultural authorities. Sampling process was carried out during the daily slaughtering work on the slaughtering panel so that no IRB was required.
Blood Sample and Serum Separation
A total of (230) blood sample were collected from the main abattoir of the region throughout a period of 15 months. Labeled sterile vacutainers were used to collect blood from animals at the time of slaughter (on the slaughtering panel) so no IRP was required. 5ml blood were collected in anticoagulant -free bottles which kept in slanted positions prior to being transported to the laboratory for serum separation.Clotted samples were centrifuged (4,000Xg for 15 min). Animal sera were stored at – 20°C till assay application.12
Serological Assays
Rose Bengal Test (Rbt)
Rose Bengal Test was applied to serologically estimate the prevalence of brucellosis associated with Egyptian abattoirs.All serum samples were tested for agglutination against Brucellaantigen using (PrioCHECK® BrucellaRose Bengal Test Kit, Prionics -Switzerland) by qualitative method according to the enclosed instructions. Briefly, equal volumes up to 30µl from both serum sample and Brucellaantigen were mixed together and manually agitated for 2 minutes. Agglutination was considered a positive result and indicates the presence of specific antibodies to Brucellain the animal serum. While no agglutination was considered as a negative test result and indicates absence of specific antibodies to Brucella.13 For increasing the test sensitivity, all positive sera were diluted by isotonic saline into 1/2, 1/4, 1/8, 1/16, 1/32, 1/64 dilutions and examined semi quantitatively.14
Modified In-House ELISA for Bovine Brucellosis Diagnosis
Modified in-house ELISA assay was performed for rapid diagnosis of bovine brucellosis as described in.15,16 96 well ELISA plates (ICN Biomedicals, OH) were coated with antigens: B. abortus antigen (BD). Serum samples were diluted using the appropriated conjugating buffer to 1:160 and 1:320 dilutions. 100 µl from samples, Blank, positive and negative controls were introduced into the coated plates in two wells (duplicate), covered with a lid and incubated for one hour at 37°C in a humid chamber. Contents were discarded, washed three times and then loaded with the conjugate (Anti-Bovine IgG (H+L)−Peroxidase antibody produced in goat KPL). After that Plates were Incubated for 30 min at 37°C in a humid chamber. Then contents were discards and washed three times .100 µl of the prepared substrate (Sigma-Fast OPD tablets) solution were added to each well. Plates then were incubated for 30 min at room temperature (aprx 25°C-27°C) in the dark. 50 µl of stopping solution (1 M H2SO4)were added to each well. Developed color intensity ( optical density OD) were read at 492 nm. An OD cutoff point of 0.38 has been established as the cut-off of the assay. Any sample showed an OD value ≥ 0.38 was considered initially reactive at serum titer > 1: 320 are considered reactive for the presence of anti-Brucellaantibodies. Samples showed OD > 0.38 at 1:160 and < 0.38 at 1:320 were considered equivocal. Sample show an OD < 0.38 at 1:160 was considered non-reactive and was reported as negative for anti-Brucellaantibodies.
Genomic DNA Extraction
Total DNA was extracted from serum samples using a genomic DNA mini kit (Qiagen, QIAampminprep, USA) according to the manufacturer’s protocol. The extracted DNA was stored at -20°C for further use. DNA concentration and purity of stock solutions were measured by with a Nano-Drop ND-1000 spectrophotometer at 260 and 280 nm.
Taqman Real-time PCR Assay
Serum samples were evaluated by Taqman real time assays for 11S7 gene amplification for identification of Brucella genus as described in.17 The real-time PCR assays were carried out for Brucellaidentification using IS711 oligonucleotides pairs(forward: GCTTGAAGCTTGCGGACAGT) and (reverse GGCCTACCGCTGCGAAT and dual labeled FAM and BHQ probe(FAM-AAGCCAACACCCGGCCATTATGGT-BHQ-1)commercially purchased from ( Biosearch Technologies USA). Typical 25 µL reaction contained: 12.5 µL Taqman Universal PCR Master Mix (Applied Bio-systems, USA), 300 nM concentration of each forward and reverse primer, 200 nM concentration of the labeled probe and 2.5ng of sample DNA. Taqman real-time PCR reactions were developed in (Step one plus – Applied Bio-systems equipment). The reaction mixture was initially incubated for 5 min at 95°C. Amplification was performed for 45 denaturation cycles at 95 °C for 20 s, annealing and extension at 60°C for 1 min. Samples exhibited sigmoid amplification peaks with below 40 cycle thresholds (CTs) were considered as positive.
Statistical Analysis
Statistical analysis was performed as described in.18,19 Considering the real time PCR the gold standard , the sensitivity and specificity of RBT and ELISA tests wereevaluated using a total of 230 sera samples collected from two focal abattoirs. Each serum sample was subjected to the three tests and the resultswere entered into the computer. The reported data of the three tests’ results was summarized in cross tabulation. Data were statistically analyzed using (Med-Calc statistical software). sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, prevalence, positive predictive value, negative predictive value and accuracy with relevance to 95% confidence intervals (CI) were calculated for serological tests in comparison to real time PCR as a gold test.
Identification of statistical variables (Table 2,4)
|
True positives |
= a | Animals with real time positive and are test positive |
|
True negatives |
= d | Animals with real time negative and are test negative |
| False positives | = b |
Animals with test positive and are real time negative |
| False negatives | = c |
Animals with real time positive and are test negative |
Results
Prevalence of Brucella in Male Calves
A total of n= 230 serum sample were obtained from two main focal abattoirs in Egypt. All sera samples were tested blindly for the presences of Brucella using three assays ELISA , RBT and Taqman real time PCR. The prevalence of brucellosis varied according to the applied test (Table 1). The overall prevalence of brucellosis was n=124 (53.9 %) , n=173 (75.2 %) and n= 182 (79.1 %) as determined by ELISA ,RBT and RT- PCR assays respectively.
Table 1: Prevalence of brucellosis in asymptomatic male calves in the two slaughterhouse (abattoirs) by number and percentage of positive results per test used for detection.
| Sample( N) | ELISA | RBT | IS711 real time PCR |
| 230 | 124 ( 53.9 %) | 173 (75.2%) | 182 (79.1) |
Comparison of Sensitivity and Specificity of Serological Tests to IS711 Taqman Real time PCR
In this study we compared the results of n= 230 serum sample obtained from serological tests to the results determined by Taqman real time PCR as a sensitive and gold standard test.Raw data including; positive , negative values and percentages for each test is indexed in (Table 2).
Table 2: Raw data obtained from Rose Bengal Test (RBT) where true positives = (a), true negatives= (d), false positives= (b) and false negatives= (c)
| Real time PCR | Brucella (RBT) | ||
| Positive | Negative | Total | |
| Positive | (a) =144 | (b) =38 | (a+b) =182 |
| Negative | (c) =29 | (d)= 19 | (c+d) =48 |
| Total | (a+c) =173 | (b+d) =57 | n=230 |
Comparison of Rose Bengal test to IS711 Taqman Real time PCR (Table 3 )
From (n=182) positive RT-PCRup to(n=144) were positive and (n=38) sample were negative to RBT respectively. Using Med-Calc statistical software and by considering RT-PCR as the gold standard:the sensitivity, specificity and accuracy of RBT were calculated as79.12% ,39.58 % and70.87% respectively with a 95% confidence interval (CI) of (72.49% – 84.78%), (25.77% – 54.73%) and( 64.54% – 76.66%) respectively. Moreover, positive likelihood ratio (PLR) for RBT test was 1.31 while negative likelihood ratio(NLR) was determined as 0.53. For rose Bengal Test, positive predictive value(PPV) 83.24% was reported as while the negative predictive value (NPV) was reported as 33.33%.
 |
Table 3: Statistical data of RBT for diagnosis of bovine brucellosis in comparison to real time PCR in a 95% confidence interval (CI).
|
Table 4: Raw data obtained from ELISA where true positives = ( a), true negatives= (d), false positives= (b) and false negatives= (c)
| Real time PCR | In-house ELISA | ||
| Positive | Negative | Total | |
| Positive | (a) = 101 | (b) = 81 | (a+b) =182 |
| Negative | (c) = 23 | (d) = 25 | (c+d) =48 |
| Total | (a+c) = 124 | (b+d) = 106 | n=230 |
Comparison of ELISA test to IS711 taqman Real time PCR (Table 5)
Regarding to ELISA assay only (n=101) sample from (n=182) positive RT-PCR were positive while (n=81) sample were negative. The test sensitivity was55.49% witha 95% confidence interval (CI) of(47.96% – 62.85%) and the specificity was 52.08 %witha 95% confidence interval (CI) of (37.19% – 66.71%) in addition to an accuracy of 54.78% witha 95% confidence interval (CI) of(48.11% – 61.33%). The positive likelihood ratiofor ELISA test was evaluated as 1.16while negative likelihood ratiowas determined as 0.85. The positive predictive valuewas reported as 81.45% while the negative predictive value was reported as 23.58 % %.Our results indicated that rose Bengal test is superior in sensitivity and specificity, followed by I-ELISA.
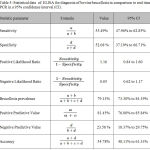 |
Table 5: Statistical data of ELISA for diagnosis of bovine brucellosis in comparison to real time PCR in a 95% confidence interval (CI).
|
Discussion
Screening and confirmatory diagnostic tests are the principal toolfor efficient epidemiological analysis.19 In Egypt although several papers were published to figure out the incidence of bovine brucellosis in various animal settings, only very few data are available on sensitivity and specificity of the serological tests.
Understanding the diagnostic sensitivity and specificity of an assay would contribute to minimize diagnostic problems in classifying diseased and non-diseased animals accurately in order to prevent unnecessary economical deficits in cases the animals are incorrectly identified by the tests.20 In accordance with our results rose Bengal test had the superior performance and then ELISA in descending order of sensitivity, specificity and accuracy. RBT continues to be the preferred screening tool owing to its fast result and cost availability21 A test with suitable positive predictivity (PPV) is necessary for ensuring the presence of disease, in addition to a test with good negative predictivity (NPV) to exclude the infection.22 The purpose of diagnosis is usually to search for cases while maintaining false positives to a minimal level. One of the most important drawbacks of rose Bengal test is the considerable high numbers of false positive results which are commonly explained as a result of cross reactivity of the test with different types of bacteria.Considering the real time PCR the gold standard, the present study indicated that the sensitivity of rose Bengal test is 79 %, while Cernysevaet al.22 found that the sensitivity of the test was 68.6%, Mesa et al23 and Altwegget al24 place the quantity at 93.8 and 100%, respectively.The sensitivity of the RBT relies on the antigenic concentration and commercial antigenic formula utilized which provide a clarification for the differences of viewpoint present in the literature around the sensitivity of the RBT.
The sensitivity and specificity of ELISA in the present study (55.49%and 52.08 %respectively) are deviate from those experienced in other reports, for instance,25 stated an ELISA sensitivity of 71.3% and a specificity of 100%. The lower sensitivity of ELISA in our study could be also due to the participation of animal with former or possibly chronic infection where the titer of antibodies is relatively low.As determined by the results acquired from the current study, the employment of real-time PCR approach along with one or more serological assay, particularly RBT is highly advisable for appropriate diagnosis of bovine brucellosis in developed and low resources regions.
Conclusion
There is no individual serological test is convenient in all epidemiological conditions and all animal species. all tests have constraints especially when examining individual animals. Attention is required to be given to all variables that affect the relevance of the test procedure and test results to a certain diagnostic interpretation or utility. Therefore, carrying out test validation is extremely necessary to know the test properties and to decide the type of test we need to use for the study objective, epidemiological monitoring, or global trade. However, the assessment for the diagnostic test for diverse purposes not only depends on the accuracy, but also should take into account the capacity for the test throughput, technical intricacy, as well as affordability.
References
- Kumar A, Gupta V, Verma A, Sahzad K, Singh A, and Reddy N. Seroprevalence and risk factors associated with bovine brucellosis in western Uttar Pradesh, India. Indian journal of animal sciences.2016;86:131-135.
- Kumar N, Pal B, Yadav S, Verma A, Jain U, and Yadav G. Prevalence of bovine brucellosis in Uttar Pradesh, India. Journal of Veterinary Public Health. 2009;7:129-131.
- Neha W, Verma A, Jain U, and Bist B. Brucellosis in organized dairy farm: an investigation. Asian Journal of Animal Sciences. 2014;8:29-33
CrossRef - Atluri V, Xavier M, de Jong M, den Hartigh A, and Tsolis R. “Interactions of the human pathogenic Brucella species with their hosts,” Annual Review of Microbiology. 2011;65:523–541.
CrossRef - Toft N Jørgensen, and Højsgaard S. “Diagnosing diagnostictests: evaluating the assumptions underlying the estimation of sensitivity and specificity in the absence of a gold standard,” Preventive Veterinary Medicine.2005;68: 19–33.
CrossRef - Gari G, Biteau-Croller F, Le Goff C, Caufour P, and Roger F.“Evaluation of the indirect fluorescent antibody test for the diagnosis and screening of lumpy skin disease.” Veterinary Microbiology.2008;129:269–280.
CrossRef - Sanogo M, Thys E, Achi Y. et al., “Bayesian estimation of the true prevalence, sensitivity and specificity of the Rose Bengal and indirect ELISA tests in the diagnosis of bovine brucellosis. Veterinary Journal. 2013;195:114–120.
CrossRef - Tsegay A, Tuli G, Kassa T, and Kebede N. Seroprevalence and risk factors of brucellosis in abattoir workers at DebreZeit and Modjo export abattoir, Central Ethiopia. BMC Infectious Diseases. 2017;17:101.
CrossRef - Mantur B, Parande A, Amarnath S, Patil G, Walvekar R, Desai A. et al., ELISA versus conventional methods of diagnosingendemic brucellosis. American Journal Of Tropical Medicine And Hygiene. 2010;83:314-18.
CrossRef - Erfanian MSeyyed, Nouzadi S,Jarahi L. Evaluation of Diagnostic Sensitivity of Wright, Coombs Wright and 2-Mercapto Ethanol in Diagnosis of Brucellosis. Evidence-based Care Journal. 2013;2: 69-74.
- Amin M, Ahmed S, Zaki H, Ismail R. Serological and molecular studies on the diagnosis of bovine brucellosis. Nature and Science. 2012;10;68-76.
- O’Leary S,Sheahan M,Sweeney, T. Brucellaabortusdetection by PCR assay in blood, milk and lymph tissue of serologically positive cows. Research in Veterinary Science. 2006;81:170-176.
CrossRef - Altwegg M,and Bohl E. Evaluation of a rapid, reliable, and inexpensive screening test for the serological diagnosis of human brucellosis. ZentralblBakteriolMikrobiolHyg [A].1985;260:65-70.
- Baum M,Zamir O,Bergman-Rios R, Katz Beider Z, Cohen A,Banai, M. Comparative evaluation of microagglutination test and serum agglutination test as supplementary diagnostic methods for brucellosis. Journal of Clinical Microbiology. 1995;33:2166-70.
- Fadeel M,Wasfy M, Pimentel G,Klena J, Mahoney F, Hajjeh R, Rapid enzyme-linked immunosorbent assay for the diagnosis of human brucellosis in surveillance and clinical settings in Egypt. Saudi Medical. 2006;27:975-98.
- Fadeel, M.Robyn, A. Pimentel, Alex, R.etal. Comparison of four commercial IgM and IgG ELISA kits for diagnosing brucellosisJournal of Medical Microbiology. 2011;60: 1767–1773.
- Hinić V, Brodard I, Thomann A, Cvetnić Z, Makaya P,Frey J, Abril C. Novel identification and differentiation of Brucellamelitensis, abortus, B. suis, B. ovis, B. canis, and B. neotomae suitable for both conventional and real-time PCR systems. Journal of Microbiological Methods. 2008;75:375-8.
CrossRef - Chatfield C. Confession of a pragmatic statistician. The Statistician 51 (part 1).2002:1-20.
- Joyee A,Thyagrajan S, Sowmya B, Venkatesan S,Ganapathy M. Need for specific & routine strategy for the diagnosis of genital chlamydial infection among patients with sexually transmitted diseases in India. Indian Journal of Medical. 2003;118:152-157.
- Lucero, N. Ayala, S. Escobar, G. Jacob, N. The value of serologic tests for diagnosis and follow up of patients having brucellosis. Journal of . Infectious. Diseases. 2007;3:27–35.
CrossRef - Rahman M. Experimental Infection and Protective Immunity of Sprague-Dawley Rats with Brucella abortus. PhD Thesis, Graduate School of Chonbuk National University, Jeonju. 2003.
- Chachra D,Saxena H, Kaur G, Chandra, M. Comparative efficacy of Rose Bengal plate test, standard tube agglutination test and dot ELISA in immunological detection of antibodies to Brucella abortus in sera. Journal of Bacteriological Research. 2009;1:30–33.
- Cernyseva M Knjazeva and Egorov L. Study of agglutination test with Rose Bengal antigen for diagnosis of human brucellosis. Bulletin. W.H.O. 1977;55:669-674.
- Mesa J,Gonzalez1 J,Reguera M, Martin L, Palmero S, Colmenero J. Rose Bengal test: diagnostic yield and use for the rapid diagnosis of human brucellosis in emergency departments in endemic areas. Clinical Microbial Infection. 2005;11:221–225.
CrossRef - Altwegg M, and Bohl E. Evaluation of a rapid reliable and inexpensive screening test for serological diagnosis of human brucellosis. Zentbl. Bakteriol. 1985;260:65-70.
- Waffa A, Shaimaa A, Ameer H, Nawal D, Nameer I, Saeed Y. Sensitivity and specificity of various serological tests for detection of Brucella spp. infection in male Goats and sheep. Advances in Microbiology. 2016;6:98-103.
CrossRef

