
Manuscript accepted on :20 June 2018
Published online on: 27-06-2018
Plagiarism Check: Yes
Ashith M. V1 , B. K. Shetty2, Yash Shekatkar3, Utkarsh Mangal4and Mithun K5
, B. K. Shetty2, Yash Shekatkar3, Utkarsh Mangal4and Mithun K5
1Department of Orthodontics and Dentofacial Orthopedics Manipal College of Dental Sciences, Mangalore Manipal Academy of Higher Education Karnataka, India.
2Department of orthodontics Coorg Institute Of Dental Sciences Coorg District, Virajpet, Karnataka, India.
3Department of Orthodontics YMT dental college and hospital Mumbai, Maharashtra, India.
4Consultant Orthodontist, Jaipur, Rajasthan, India.
5Department of Orthodontics, A.J Institute of Dental Sciences,Kuntikana,Mangalore, Karnataka, India.
Corresponding Author E-mail: Utkmangal@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1456
Abstract
Anchorage in orthodontics is a decisive factor in progress and outcome of a case. With the advent of mini-implants, great advances have been achieved in terms of absolute anchorage. The following article compares the use of stainless steel and titanium implants in a split mouth, controlled clinical study, having direct in vivo comparison. 10 patients were selected for the same and carefully evaluated. The mini-implants were placed in the buccal mucosa, under local anaesthesia, after radiographic safe zone selection. The loading protocol was standardised with low immediate load, followed by incremental load up to 150g. For the study, the cases planned with en-masse retraction of the anteriors into the premolar space were selected for the uniformity in mechanics. The results are discussed with comparative analysis between the two materials and their success rate individually and in relation to upper and lower jaw respectively. In results, a significant success rate has been found with use of titanium implants, with higher implant failure in upper jaw compared to lower jaw.
Keywords
Anchorage; Mini-Implants, Orthodontics; Stainless Steel; Titanium
Download this article as:| Copy the following to cite this article: Ashith M. V, Shetty B. K, Shekatkar Y, Mangal U, Mithun K. Assessment of Immediate Loading with Mini-Implant Anchorage in Critical Anchorage Cases Between Stainless Steel Versus Titanium Miniscrew Implants: A Controlled Clinical Trial. Biomed Pharmacol J 2018;11(2). |
| Copy the following to cite this URL: Ashith M. V, Shetty B. K, Shekatkar Y, Mangal U, Mithun K. Assessment of Immediate Loading with Mini-Implant Anchorage in Critical Anchorage Cases Between Stainless Steel Versus Titanium Miniscrew Implants: A Controlled Clinical Trial. Biomed Pharmacol J 2018;11(2). Available from: http://biomedpharmajournal.org/?p=21015 |
Introduction
In the current era of modern orthodontic practice, the traditional envelope of discrepancy has been amended with the introduction of the temporary anchorage devices (TAD). The advent of TAD has given a unique boost to the anchorage system by providing absolute anchorage which was not possible earlier.1 Mini implants as a form of temporary anchorage devices have been used for over a few decades in all parts of the world and have found utility in diverse types of tooth movements ranging from en-masse retraction to occlusal cant correction or true up righting of molars.
The material of choice for the mini–implant system has been widely accepted to be titanium, due to its excellent biocompatibility and environmental stability.2 However, titanium by availability and processing proves to be more expensive and relatively less affordable. This particularly has impact in developing nations, where scope and quality of treatment gets directly influenced by affordability. Hence, alternative materials have been proposed of which stainless steel meets the minimum requirements, for a mini-implant adequately.
Therefore, this study aims to compare the success rate between the mini-screw implant systems of two different materials viz. Titanium and Stainless steel under immediate loading for various applications in orthodontic treatment.
Material and Methodology
This prospective controlled clinical study was based on a sample size of 10 patients (for type 1 error of 5% with an 80% power of the study), (15-25 years of age) who were selected for use of mini-implants. Two categories of implant materials titanium and stainless steel were selected to be compared as per the aim of the study. Insertions were planned in upper or lower arch, based on clinical requirement of enhanced anchorage. The placement of implants was bilateral with a split mouth study pattern. For maintaining the uniformity in terms of application, all mini-implants were planned for a direct anchorage en-masse retraction. The screws were placed in the buccal mucosa in the inter-radicular region between the first molar and second premolar in all subjects to facilitate retraction of anteriors into the premolar extraction space. The exclusion criteria for case selection was: known case of allergy to foreign substances and being allergic to any metallic objects, history of previous orthodontic treatment and poor oral hygiene.
The subjects selected were pre-screened by intra-oral periapical radiographic technique to confirm suitable bone support and inter-radicular space with adequate safety margins from vital structures. All the implants were placed in the selected safe zone between molar and premolar of the respective jaw, by the same operator, by self-drilling method under local anaesthesia. Topical anaesthesia was given to reduce the prick of the needle for infiltration anaesthesia. About one-fourth (0.5mL) of infiltration anaesthesia was given to only desensitise the soft tissues.
The implants based on materials were divided into two types
| TYPE | Material | Dimension |
| A | Stainless steel miniscrew implant (S.K Surgicals) | 1.3mm diameter and 8mm length |
| B | Titanium mini Screw implant (Dentos) | 1.3mm diameter and 8 mm length |
The placement of the screws was done at placement angle of 30-40 degrees in upper and 20-60 degrees in the lower in relation to the long axes of the teeth. The stability of the mini-implant post insertion was checked and radio graphs were taken to confirm the location of the implant and rule out undesirable proximity to sinus or the root.3 All subjects were provided with clear specific instructions to maintain good oral hygiene, with emphasis on regular use of mouthwash. Following placement, the implants were immediately loaded, with initial low force of 50-70g followed by scheduled increment after 2 months of follow up. Regular periodic follow up were planned, of 30 days interval, to assess the stability of the implant in relation to peri-implant infection, ulceration, inflammation or increased mobility of the implant per se. This was scheduled to be assessed within a span of one year or till the end of treatment, if the treatment finished before one year.
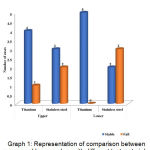 |
Graph 1: Representation of comparison between upper and lower arches with different test materials |
Statistical Analysis
Mann – Whitney Test
This test is useful for testing the difference between unpaired observations. Here the observation is arranged in the order of their magnitude taking observation of both the samples together. Proper tags was made to distinguish the observation of both the samples together. Then the ranks are assigned to the combined observation according to the magnitude.
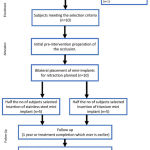 |
Figure 1: Description of the stages of the study protocol |
Chi-Square Tests
Under the alternative hypothesis the probability of an observation from one population (X) exceeding an observation from the second population (Y) (after correcting for ties) is not equal to 0.5. The alternative may also be stated in terms of a one-sided test.
Results
Comparing the success rates of Type A (Titanium Screw) implant and Type B (Stainless Steel) implant.
Table 1 compares the two types of mini implants Type A and Type B with respect to Mann Whitney test. On comparison the upper arch the Type A implant had a duration of score of 4 + 1.87 and Type B mini implant it is 3.2 + 2.167 and p = 0.511 which was in significant.
Table 1: Means and standard deviation of clinical variables in success and failure rate of Type A and Type B mini implant based on the duration.
| GROUP | MATERIAL | N | Mean | Std. Deviation | Z | P (< 0.05) |
| Upper | Titanium | 5 | 4.0000 | 1.87083 | .65700 | p=0.511 (NS) |
| Stainless Steel | 5 | 3.2000 | 2.16795 | |||
| Lower | Titanium | 5 | 5.0000 | .70711 | 1.20500 | p=0.228 (NS) |
| Stainless Steel | 5 | 2.8000 | 2.48998 |
NS= statistically non significant
In lower arch duration of Type A mini implant was 5 + 0.70711 has p= 0.324 Type B in lower arch is 2.8 + 2.48 and the p = 0.822 which was not significant.
Table 2: Success rate and number of screws according to clinical variable of subject treated with type A and type B mini implant in upper and lower arch.
|
GROUP |
MATERIAL | Total | ||||
| Titanium | Stainless Steel | |||||
| Upper | Stable | Count | 4 | 3 | 7 | |
| % | 80.0% | 60.0% | 70.0% | |||
| Failed | Count | 1 | 2 | 3 | ||
| % | 20.0% | 40.0% | 30.0% | |||
| Total | Count | 5 | 5 | 10 | ||
| % | 50.0% | 50.0% | 100.0% | |||
| Lower | Stable | Count | 5 | 2 | 7 | |
| % | 100.0% | 40.0% | 70.0% | |||
| Failed | Count | 0 | 3 | 3 | ||
| % | 0% | 60.0% | 30.0% | |||
| Total | Count | 5 | 5 | 10 | ||
| % | 50.0% | 50.0% | 100.0% | |||
The success rate of titanium implants in the lower arch (100%) was higher than in the upper arch (80%) whereas the failure rates were higher in the upper arch (20%) as appreciated in table 1 and graph 2. But the difference was not statistically significant (p=0.324). The stainless steel implant exhibited a higher success rate in the upper arch (60%) than in the lower arch (40%), whereas the failure rate was higher in the mandibular arch (60%), but this difference was also not statistically significant (p=0.822). [Table 3]
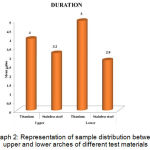 |
Graph 2: Representation of sample distribution between upper and lower arches of different test materials |
Table 3: Mean and standard deviations of clinical variable in success and failure of Type A and Type B mini implant based on the duration.
| MATERIAL | GROUP | N | Mean | Std. Deviation | Z |
| Titanium | Upper | 5 | 4.0000 | 1.87083 | .98600 |
| Lower | 5 | 5.0000 | .70711 | p=0.324 (ns) | |
| Stainless Steel | Upper | 5 | 3.2000 | 2.16795 | .22400 |
| Lower | 5 | 2.8000 | 2.48998 | p=0.822 (ns) |
ns- non significant
Comparison of implant stability based on the duration, showed that the titanium implant was more stable than the stainless steel implant in both the maxillary and mandibular arch (Table 2). However the titanium screw implant was more stable in the mandibular arch (100%) than the maxillary arch (80%), whereas the stainless steel implant was more stable in the maxillary arch (60%) than the mandibular arch (40%). These differences were not statistically significant.
Comparison of the overall failure rates revealed that stainless steel implants had a higher failure rate (50%) as compared to titanium screw implants (10%) and this difference was statistically significant (p=0.0325) (table 4)
Table 4: Failure of Type A and Type B mini implant in both the arches.
| MATERIAL | TOTAL | |||
| TITANIUM | STAINLESS STEEL | |||
| STABLE | COUNT | 9 | 5 | 14 |
| % | 90% | 50% | 70% | |
| FAILED | COUNT | 1 | 5 | 6 |
| % | 10% | 50% | 30% | |
| TOTAL | COUNT | 10 | 10 | 20 |
| % | 100% | 100% | 100% | |
A.X2= 3.84, P=0.0325 (p<0.05= statistically significant)
Discussion
Achieving absolute anchorage has been one of the main objectives for orthodontist and mini implants have become one of the most effective and powerful tools for achieving it. The present implant systems are bound to change and evolve into more patient friendly and operator convenient designs. A variety of implant systems ranging from the conventional prosthetic implants to small diameter mini screws used as temporary anchorage devices have been utilized world over for achieving absolute anchorage1. Endosseous implant and palatal onplants,4 are thought to provide absolute or rigid anchorage, they integrate with the surrounding bone and thus remain absolutely stationary under orthodontic loading. Stability of the mini-screws is derived from both the resistance from the cortical bone and secondarily from the integration to the bone.
Also, it has been suggested that a waiting period for bone healing and osseointegration before loading is unnecessary because the primary stability (mechanical retention) of the screws is sufficient to sustain a regular orthodontic loading2.
Though the material of choice in mini-implants have been titanium alloy,5 the high cost associated with the titanium based mini screws can form a limiting factor. Fractures of the oro-facial region have had been successfully treated by use of stainless steel screws and plates in oral and maxillofacial surgery and have been used for skeletal anchorage in orthodontics.6,7 However, the use of Stainless steel screw in the form of temporary mini-screw anchorage system has not been the material of choice for the manufacture of these implant has always been a titanium alloy5, especially because of the sole property of biocompatibility. However, titanium alloy are expensive. It’s a very well-known fact that the fractures of the oro facial region are being successfully treated with stainless steel screw and plates by the oral and maxillofacial surgeon. Similar plates have also been used in orthodontics for the purpose of skeletal anchorage.8 But stainless-steel screw has not been used for skeletal anchorage purpose in orthodontics as much as counterpart titanium.
Cheng et al (2004),9 conducted a study to assess the risk factor associated with failure of titanium alloy mini screw and stainless steel mini plates used as orthodontic anchorage. The study confirmed the reliability of mini screw and mini plate, though the failure was more likely when the implants were placed in the posterior mandible. The result justifies with the result of our study in which the failure of implant was 60% in lower arch. Adjustment of the treatment plan or modification in the technique of the implant placement may help improve the success rate. Shouichi et al (2003),10 examined the success rates and the factors associated with the stability of mini-screw placed into the buccal alveolar bone of the posterior region using titanium mini screw with different diameters and length. The reason for the mobility of implant according to them was inflammation of peri-implant tissue. In the present study, with the use of mini-implant of both types, the sites associated with the implant failure showed increased inflammation in surrounding tissues. The assessment of the peri-implant tissue was made with subjective parameters, such as increased redness and oedematous ulcerative margins. The observation was concorded by two examiners and the stability of the implant verified using a probe. Implants that showed increased mobility from the time of loading were categorised as failed and removed. Thus, the result of our study is in close agreement with the above study. However, as in the present study no definite objective assessment of peri-implant tissue response was made, further research would be required to quantify the biochemical tissue response for correlation to stability. Kuroda et al (2007),8 evaluated the clinical usefulness of miniscrew implants as orthodontic anchorage: success rates and post-operative discomfort. The results showed that the success rate for each type of implant was greater than 80%. This is also true with titanium implants in our study were the success rate was 90%. It was found out that mini screws placed without flap surgery had high success rates with less pain and discomfort.11
The evaluation of the stability in the present study was independent of the site of the mini screw placement, which could be a factor in difference of stability, considering the variable density of the bone in the maxillary and mandibular region. The difference in the density of the bone with age can also influence the primary stability of the implant, though long term stability will not have a significant influence.
Conclusion
The present study showed both that the titanium and stainless steel implants can be used for orthodontic anchorage purpose. The result of this study showed that the success rate of titanium implants were more than stainless steel implants. In accordance with the previous studies there was higher success rate in the maxilla than the mandible. Some of the probable reason for failure of stainless steel implant might be peri-implantitis and less biocompatibility when compared to titanium implants. Improvements in the material property may increase the success rate of stainless steel implants in future. From the present study it can be concluded that titanium implants can be successfully used as a temporary anchorage device.
Further Scope
The study sample can be made more specific with standardisation of bone density parameters based on CBCT scans.
Analyses of the stability specific to maxillary or mandibular arch form can be done with larger sample size with comparison between anterior and posterior regions to illuminate the statistical probability of success.
Conflicts of Interest
There is no conflicts of interest.
Funding of Source
There is no funding of source
Acknowledgement
The author(s) received no specific funding for this work.
References
- Costa A, pasts A, Bergamaschi G. Intraoral Hard and Soft tissue depths for temporary Anchorage Devices. Semin Orthod. 2005;11;10-15.
CrossRef - Buchter A, Wiechmann D, Koerdt S, Wiesmann H.P, Piffko J, Meyer U. Load-related implant reaction of mini-implants used for orthodontic anchorage. Clin Oral Implants Res. 2005; 16(4):473-9.
CrossRef - Schnelle M.A, Beck F.M, Jaynes R.M, and Huja S.S. A Radio graphic Evaluation of the Availability of Bone for Placement of miniscrew. Angle orthod. 2004;74:832-837.
- Kang S, Lee SJ, Ahn S.J, Heo M.S and Kim T.W. Bone thickness of the palate for orthodontic mini- implant anchorage in adult. Amj Orthod Dentofacial Orthop. 2007:131;00.
- Park S.H, Jeong S.H and kwon O.W. Factors affecting the clinical success of screw implants used as orthodontic anchorage .Am.J orthod Dentofacial Orthop. 2006;130:18-25.
CrossRef - Sukegawa S, Kanno T, Shibata A, Takahashi Y, Furuki Y. Use of templates and self-tapping metal screws for temporary fixation of a resorbable plate system. Ann Maxillofac Surg. 2015;5:231-3.
CrossRef - Disegi J.A, Eschbach L. Stainless steel in bone surgery. Injury. 2000;1(31):D2-6.
CrossRef - Kuroda S, Sugawara Y, Deguchi T, Kyung H.M, Yamamoto T. Clinical use of mini implant as orthodontic anchorage: success rate and post operative discomfort. Am .J Orthod Dentofacial Orthop. 2007;131:9-15.
CrossRef - Cheng S.J, Tseng I.Y, lee J.J, Kok S.H. A prospective study of the risk factors associated with failure of mini- implant used for orthodontic anchorage. Int. J Oral Maxillofac Implant. 2004;19:100-106.
- Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Yamamoto T.T. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Ortho Dentofacial Orthop. 2003:124:373-378.
CrossRef - Kanomi R. Mini implant for orthodontic anchorage. J Clin Orthod. 1997;31:763-767.

