
Pollyana Coutinho Cunha1, Darlene Cristina Ramos Eloy Dantas2, Ana Isabella Arruda Meira Ribeiro2, Alidianne Fábia Cabral Cavalcanti2, Rodivan Braz3 and Alessandro Leite Cavalcanti2
1DDS, Private Practice.
2School of Dentistry, State University of Paraiba, Campina Grande, PB, Brazil.
3School of Dentistry, Universidade de Pernambuco, Camaragibe, PE, Brazil.
Corresponding Author E-mail: alessandrouepb@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1344
Abstract
Marginal microleakage is one of the major disadvantages of resin composite restorations. The purpose of this study was to evaluate in vitro the effect of reinforcement with fiberglass in Class I restorations with composite resin on the marginal microleakage.The sample was composed by 30 human third molars, which were divided into 3 groups: G1 (no fiberglass – control group), G2 (1 layer of fiberglass) and G3 (2 layers of fiberglass). The restorations were subjected to a total of 300 thermal cycles and were immersed in solution of methylene blue 2%. The analysis of microleakage was performed in a stereomicroscope and measured Data were analyzed statistically by the Chi-square and ANOVA tests at 5% significance level. G3 presented the lower infiltration index, but it was not statistically significant (p>0.05), indicating that use of fiberglass did not appears effective against microleakage. Although the use of layers of fiberglass slightly reduces polymerization shrinkage, the incremental technique seems to be more viable clinically.
Keywords
Composite Resins; Dental Restoration;Dental Leakage Permanent;
Download this article as:| Copy the following to cite this article: Cunha P. C, Dantas D. C. R. E, Ribeiro A. I. A. M, Cavalcanti A. F. C, Braz R, Cavalcanti A. L. In vitro Evaluation of the Effect of Reinforcement with Fiberglass in Class I Restorations with Composite Resin. Biomed Pharmacol J 2018;11(1). |
| Copy the following to cite this URL: Cunha P. C, Dantas D. C. R. E, Ribeiro A. I. A. M, Cavalcanti A. F. C, Braz R, Cavalcanti A. L. In vitro Evaluation of the Effect of Reinforcement with Fiberglass in Class I Restorations with Composite Resin. Biomed Pharmacol J 2018;11(1). Available from: http://biomedpharmajournal.org/?p=19642 |
Introduction
Resinous materials have evolved throughout the time, and many difficulties have been arising, especially as regards tooth adherence.1,2 Their purpose is to fulfill dental cavity, replacing carious or damaged tissue by a biocompatible material, which may recover the function of the dental element.3 Acid-etching of enamel increases bond strength by producing a micromechanical union between the adhesive and the enamel.1 Adhesive systems presenting excellent behavior on enamel are still questioned as regards their efficiency on dentin. Those systems have been shown to be present several changes, both in compositions and presentations.
Although composite resin presents work and color properties similar to tooth structure, it is still has enormous disadvantage, once a hermetic marginal sealing is not achieved, leading to microleakage. Restoration sealing failure is an important factor that may result in fillings loss, since it clinically contributes to the occurrence of post-operative sensibility, secondary carious lesions, staining and pulp pathologies.
The magnitude of stresses generated during composite resin polymerization is influenced by several factors related to material, technique and cavity preparation, considering that the interrelationship of these factors dictates the occurrence of contraction for a given restoration. Among the aspects, which favor stresses, generation are: volumetric polymerization shrinkage, elasticity modulus, resin flowage, composite adherence to dental substrate and cavity configuration factor of the restoration.4
The use of glass fibers aims to increase composite resin physical properties, acting as reinforcement, similarly to a metallic scaffold in the concrete structure.5 These fibers surrounded by a resinous matrix have been used as substructures to receive composite resin cover layers, showing a significant increase in the physical properties over the unreinforced material.6
The purpose of this study was to in vitro evaluate the influence of glass fibers use on marginal microleakage of composite resin fillings.
Materials and Methods
For this research were used 30 human third molars. After extraction, the specimens were stored in aqueous thymol 0.2% for 24 hours for disinfection. Then they were washed in running water and cleaned with curettes and prophy brushes (KG Sorensen Ind. Com. Ltda., Cotia, SP, Brazil) coupled to the handpiece (Kavo do Brasil Ind. Com. Ltda., Joinvile, SC, Brazil), associated with a paste of pumice and water.
The roots of the teeth were sealed with light-cured composite resin (Filtek Z350 – 3M/ESPE Brasil, Sumaré, SP, Brazil). Afterwards, the teeth were stored in distilled water at 4°C, replaced weekly for a maximum period of six months. Next, Class I cavities were prepared in dentin, totaling 30 restorations. For the confection of these cavities were standardized its dimensions (depth, width and length), which were achieved through the use of digital calipers, dermographic pencil and millimeter probe.
The cavities were prepared with a round end shaped carbide drill 330 (SS White Artigos Dentários Ltda, Rio de Janeiro, RJ, Brazil) at high-speed refrigerated, being replaced every five teeth. Later, it was established a buccolingual depth of 4 mm, 5 mm in length (mesiodistal) and 4 mm in occluded-pulp way, with aid of a digital caliper (Digimess Instrumentos de Precisão Ltda, São Paulo, SP, Brazil). For the finishing of the walls were used low speed drills.
The division of the 30 teeth was done randomly. The specimens were divided into 3 groups (n=10), in a total of 30 restorations. After the preparation of Class I cavities, the teeth were washed under running water, was held prophylaxis with pumice and water, using a prophy brush at low speed and subsequently, stored in distilled water at 4°C. The using of demineralizing agents, the application of the adhesive system and the preparation of composite resin restorations class I were performed according to the instructions of each manufacturer.
To prepare the composite resin restoration, the technique was the incremental (where were placed increments of composite resin), in which each increment was light cured for 30 seconds under halogen light intensity of 500 mW/cm² (Curing Light POLY 600S – Kavo, (Kavo do Brasil Ind. Com. Ltda., Joinvile, SC, Brazil), measured by a radiometer (Gnatus Equip. Médico-Odontológicos, Ribeirão Preto, SP, Brazil). The use of fiber glass was as follows: Group I – no fiberglass, Group II – was used a layer of fiberglass between the increments of resin and Group III – were used two layers of fiberglass; the first layer on the basis of restoration and the second between the layers of composite resin.
Next, the specimens were stored for 24 hours in plastic containers with distilled water and each container properly identified according to the restorative technique and kept in an incubator (Fanen Ltda., Guraulhos, SP, Brazil) at a temperature of 37°C. The samples received 300 cycles of thermal baths at temperatures of 5°C to 55°C in an interval of 30 seconds for each one.
After this step, the specimens were prepared to test the microleakage, applying over them a layer of fast-setting glue (Super bonder, Loctite Agro Ind. Com. Ltda, São Paulo, Brazil), limiting its termination to 1.0 mm from the restoration, and two layers of red nail polish (Risqué®, Coty Inc., São Paulo, Brazil) to prevent the penetration of the tracer agent.
The specimens were immersed in a solution of methylene blue 2% (tracer agent) for 24 hours and kept in a biological greenhouse.7 Afterwards, they were washed in running water for 2 hours. Then, the teeth were cut with diamond disc (KG Sorensen Ind. Com. Ltda., Cotia, SP, Brazil) at low speed in mesiodistal way: a cut localized at 0.2 mm from the center of the restoration comprising in two interfaces for evaluation.
The scores to measure the infiltration of the tracer agent in the mesial and distal walls were: Level 0 = No dye penetration; Level 1 = when dye penetration up to half of the surrounding wall; Level 2 = when the dye penetrates into all of wall area; Level 3 = when the dye penetration occurs at surrounding and axial walls.7
The readings were made in a stereomicroscope with 30x increase by three previously calibrated researchers, and it was established the Kappa coefficient.
The results of statistical analysis were obtained by means of descriptive and inferential analysis through the tests ANOVA and Chi-square.
Results
We found that inserting one more layer of fiberglass there was a slight decrease in the level of infiltration (Figure 1). However, this difference was not statistically significant by ANOVA analysis. It means that there are sufficient evidences that the infiltration will be the same, irrespective of the number of layers of fiberglass applied to the tooth (p = 0.32).
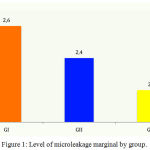 |
Figure 1: Level of microleakage marginal by group.
|
Ninety evaluations were conducted in which only 3.3% were observed total absence of infiltration and the majority has obtained the maximum infiltration represented by score 3 (Figure 2).
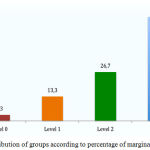 |
Figure 2: Distribution of groups according to percentage of marginal microleakage.
|
The Figure 3 showed the relationship between the groups with their treatments and their proper levels of infiltration/scores, in which was observed in the control group (G1) that 63.3% of teeth had score 3 and none of them score 0 (0.0%).
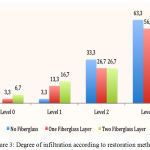 |
Figure 3: Degree of infiltration according to restoration method.
|
Therefore, there was evidence that although there was a slight difference between the levels of infiltration, with its gradual decrease through the application of fiberglass, this difference was not statistically significant (p = 0.49).
Discussion
The oral cavity is the adequate environment for predicting the degradation and durability of dental materials, but given the complexity of intra-oral conditions, in vitro studies are performed to simulate the oral environment.8-10
There are many materials in dentistry to restore teeth function and aesthetics in the oral cavity,2,11 and the material of choice for this purpose is composite resin, which besides giving a good aesthetic performance also allows restoring to a proper function of the teeth.12
Marginal microleakage is one of the major disadvantages of resin composite restorations13 and may be defined as the passage of bacteria, toxins, fluids, molecules and ions across the interface tooth / restoration.14,15 The control of polymerization shrinkage has been longed for since the beginning of the use of these resins in an attempt to minimize microleakage and thus prevent the development of post-operative sensitivity, recurrent caries and pulp damages. However, this control should be done without damaging the characteristics of the material, trying to attach the ideal properties and a lesser polymerization shrinkage magnitude.16-19 The percentage of polymerization shrinkage and modulus of elasticity of the material influence the final result of pressure generated on the tooth-restoration interface.
Many authors have analyzed the microleakage between restorations and tooth, in particular, between the restorative material and dentin substrate, which presents with a higher level of marginal microleakage.20-23 Dye penetration test is recommended to anticipate material’s clinical performance, being therefore the main technique used to evaluate marginal microleakage.7 The incremental technique favors the reduction of microleakage because the least amount of walls involved, that leads to a larger surface free area generating a relaxation of the tensions.
The choice of one type of restorative material should also be based on its clinical effectiveness proven by judicious clinical trials.24 The data generated by this study proved that the insertion of fiberglass in the restoration reduced the microleakage of composite resin, but this result did not justify the superiority of technique. Although there was an improvement, this was little or statistically null and, thus, being not advantageous add the fiberglass in restorations. In addition, it takes the operative procedure more expensive.
In face of the discussion, it was noted the necessity for more research involving microleakage tests, because the demand for esthetic restorations is increasing every day. For that it is necessary a greater knowledge about the behavior of the resin in cavity preparations to promote a longevity and quality of restorative procedures, reaching the promotion of oral health.
In this study, the use of fiberglass did not appear effective against microleakage. Despite studies that have been developed and the changes in formulation of the composite resin, still it was not possible eliminate infiltration of esthetic restorations.
Conclusion
The insertion of one or two layers of glass fiber showed a slight improvement in rate of infiltration when compared to control group and the incremental technique was more viable than the insertion technique with fiberglass.
References
- Morais J. F., Chaves L. V. F., Chaves V. S. F., Costa G. P. F., Santos A. J. S., Neto C. R. G., Machado C. T. Shear bond strength and adhesive remnant of three protocols used for bonding orthodontic brackets. Braz Res Pediatr Dent Integr Clin. 2016;16(1):433-440.
CrossRef - Zaia W. L. S., Fiqueiredo J. L. G., Leite L. M., Satake A., Medeiros I. S. Bond strenght of zirconia submitted to different surface treatments. Braz Res Pediatr Dent Integr Clin. 2015;15(1):387-398.
CrossRef - Moura K. V. M., Pacheco M. T. T. Stress related to polymerization of light cure composites resin and how to minimize them. A literature review. Arq Bras Odontol. 2006;2(1):32-38.
- Peutzfeldt A., Asmussen E. Determinants of in vitro gap formation of resin composites. J Dent. 2004;32(2):109-15.
CrossRef - Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20(1):37-46.
CrossRef - Hirata R., Mazzetto A. H., Yao E. Clinical alternative of laboratory composite resin systems – when and how to use. J Bras Clin Estet Odontol. 2001;4(19):13-21.
- Alvim H. H., Campos N. M., Vasconcellos W. A., Silva V. A., Moreira A. N., Gatti A. Influence of different photoinitiators on polymerization kinetics and marginal microleakage in restorations using photopolymerizable dental composites. Pesq Bras Odontoped Clin Integr. 2017;17(1):e2833.
- Vieira B. R., Firmino B. O., Medeiros M. I. D., Santos R. L., Guênes G. M. T., Carvalho F. G. In vitro effect of erosive challenge on surface microhardness of orthodontic composites. Braz Res Ped Dent Integr Clin. 2016;16(1):43-50.
CrossRef - Resende L. C. M., de Araújo T. P., Resende A. B., Cavalcanti Y. W., de Almeida L. F. D., Padilha W. W. N., Carvalho R. A., Sousa S. A. Fracture resistance of endodontically treated teeth restored with different types of intracanal posts. Pesq Bras Odontoped Clin Integr. 2017;17(1):e2995.
- dos Santos M. P. A., Patrocínio A. L., Fidalgo T. K. S., Camargo Jr. S. S., Maia L. C. Surface degradation of resin-based materials by pediatric syrup containing amoxicillin under erosive challenge. Pesq Bras Odontoped Clin Integr. 2017;17(1):e3446.
- Bandeira M. B., Queiroz I. M. S., Fernandes S. K. S. C., Freitas Jr. A., Özcan M., Martinelli A. E., Queiroz J. R. C. Evaluation of surface roughness of monolithic zirconia after using different polishing kits. Pesq Bras Odontoped Clin Integr. 2017;17(1):e2984.
- Silva H. A., Arossi G. A., Damo D. M., Tovo M. F. Effect of grape derived beverages in colour stability of composite resin submitted to different finishing and polishing methods. Pesq Bras Odontoped Clin Integr. 2017;17(1):e3435.
- Nik I. R., Naseri E. B., Majidinia S., Nik S. R., Giv M. J. Effect of chlorhexidine and ethanol on microleakage of composite resin restoration to dentine. Chin J Dent Res. 2017;20(3):161-168.
- Pashley D. H. Clinical considerations of microleakage. J Endod. 1990;16(2):70-7.
CrossRef - Yap A. U., Lim C. C., Neo J. C. Marginal sealing ability of three cervical restorative systems. Quintessence Int. 1995;26(11):817-20.
- Ferrari M., Mannocci F., Vichi A. Simplification of restorative procedures: an overview. In: Internacional Symposium. Reconstructions with carbon fiber system and the optimum adhesive system. Proceedings. 1998;41-3.
- Goracci G. The latest discoveries in adhesion recent studies. In: International Symposium Reconstructions with carbon fiber system and the optimum adhesive system Proceedings. 1998; 36-40.
- Fares N. H., Coutinho K. Q., Couto M. G., Couto-Júnior M., Nagem-Filho H. Tensões de Contração das Resinas Compostas Geradas durante a Polimerização. Rev Port Estomatol Cir Maxilofac. 2004; 45(3):177-84.
- Basavanna R., Garg A., Kapur R. Evaluation of gingival microleakage of class II resin composite restorations with fiber inserts: An in vitro study. J Conserv Dent. 2012;15(2):166-9.
CrossRef - Brackett W. W., Haisch L. D., Pearce M. G., Brackett M. G. Microleakage of class V resin composite restorations placed with self-etching adhesives. J Prosthet Dent. 2004;91(1):42-5.
CrossRef - Vallittu P. K., Narva K. Impact strength of a modified continuous glass fiber–poly(methyl methacrylate). Int J Prosthodont. 1997;10(2):142-8.
- Corona S. A., Borsatto M. C., Pecora J. D., De S. A .,Rocha R. A., Ramos T. S., Palma-Dibb R. G. Assessing microleakage of different class V restorations after Er: YAG laser and bur preparation. J Oral Rehabil. 2003;30(10):1008-14.
CrossRef - Loguercio A. D., de Bauer J. R. O., Reis A., Grande R. H. In vitro microleakage of packable composites in class II restorations. Quintessence Int. 2004;35(1):29-34.
- Corteleti J. F., Ota C. M., Briguet J., de Novaes T. F., Raggio D. P., Imparato J.C. P. Conservative treatment of deep dentin lesions in primary molars Case-series. Braz Res Ped Dent Integr Clin 2015;15(1):337-344.
CrossRef

