
Subbaiah Pradeep1 , Mysore Rajashekar Dhakshaini2, Nagasunder Raghunath Rao1, Vidya Doddawad3 and Bhagyalashmi Avinash2
, Mysore Rajashekar Dhakshaini2, Nagasunder Raghunath Rao1, Vidya Doddawad3 and Bhagyalashmi Avinash2
1Department of Orthodontics and Dentofacial Orthopedics JSS Dental College and Hospital JSS University , Mysuru.
2Department of Prosthodontics and crown and bridge JSS Dental College and Hospital JSS University , Mysuru.
3Department of Oral Pathology JSS Dental College and Hospital JSS University, Mysuru.
DOI : https://dx.doi.org/10.13005/bpj/1336
Abstract
Orthodontic treatment in adult patients is one of the most frequently encountered components involving Interdisciplinary approaches. The present case report is on such situation where orthodontic treatment of ectopically erupted incisors and canines resulted in a periodontal pathology. However, periodontal intervention and endodontic treatment was carried out to stabilize the achieved occlusion. The ectopically erupted teeth have been brought into occlusion and class I canine relationship has been achieved. The periodontal complications after movement of teeth into proper alignment can be better dealt with a combined teamed approach.
Keywords
Dilacerated Incisor; Ectopic Eruption; Interdisciplinary Approaches Orthodontic Treatment;
Download this article as:| Copy the following to cite this article: Pradeep S, Dhakshaini M. R, Rao N. R, Doddawad V, Avinash B. An Interdisciplinary Collaboration for the Management of Dilacerated Central Incisor and Ectopically Erupted Teeth. Biomed Pharmacol J 2017;10(4). |
| Copy the following to cite this URL: Pradeep S, Dhakshaini M. R, Rao N. R, Doddawad V, Avinash B. An Interdisciplinary Collaboration for the Management of Dilacerated Central Incisor and Ectopically Erupted Teeth. Biomed Pharmacol J 2017;10(4). Available from: http://biomedpharmajournal.org/?p=18200 |
Introduction
Normal intra-arch and inter-arch relationships have long been considered as an anatomic prerequisite for the preservation of dental health and function. Certain malocclusion traits are associated with difficulties in maintaining good oral hygiene and as a consequence to poor periodontal condition. Therefore, proper alignment of the teeth provided by orthodontic treatment may promote good control of soft deposit and calculus and subsequent periodontal inflammation.The tendency of orthodontic appliances, particularly the brackets and bands to promote the accumulation of plaque and thus increasing the risk of developing localized periodontal disease must however be constantly emphasized.1
Orthodontic treatment can facilitate management of several restorative and esthetic problems relating to fractured teeth, tipped abutment teeth, excess spacing, inadequate pontic space, malformed teeth and diastema. Orthodontic treatment may improve periodontal health in these circumstances, but it also holds some potential for harm to the periodontal tissues. Thus, orthodontic treatment can be referred to as a two-edge sword, which may be sometimes essential in increasing periodontal health status while at certain times be followed by several types of periodontal complications.2
The present case report is on such situation where orthodontic treatment of ectopically erupted incisors and canines resulted in a periodontal pathology. However, periodontal intervention was carried out to stabilize the achieved occlusion.
Case Report
A 27 years old male presented with chief complaint of irregularly placed upper and lower front teeth and he desired to get it corrected. Examination from the front showed a symmetrical and well-balanced mesocephalic facial pattern. A convex profile and a competent lip seal was observed (Fig.1a).
Clinical examination revealed a class I malocclusion with ectopically erupted 21, 22, 23. The deciduous left canine was over-retained, and the permanent cuspid was migrated labially. The dental midlines upper was shifted toward left by 3mm (Fig 1a).
 |
Figure 1a: Pre orthodontic treatment
|
The patient had a carey’s analysis tooth material excess 7mm in upper arch and lower by 5mm respectively.
Cephalometric measurements were within normal limits (Table 1).
Table 1: Cephalometric Data
| Varaibles | Pretreatment | Posttreatment |
| Sna | 81 | 81 |
| Snb | 80 | 80 |
| Anb | 1 | 1 |
| Gogn To Sn | 29 | 29 |
| Angle of Inclination | 88 | 88 |
| Lower Anterior Facial Height | 71 | 72 |
| Y-Axis | 65 | 66 |
| U1-Na(Angle) | 30 | 25 |
| U1-Na (Mm) | 8mm | 5mm |
| L1-Nb(Angle) | 27 | 25 |
| L1-Nb (Mm) | 5mm | 4mm |
| L1-A-Pogline | 4mm | 3mm |
Patient was diagnosed of having ANGLE’S class I malocclusion on skeletal class I jaw bases with horizontal growth pattern and ectopically erupted 21,22,23.
Treatment Plan
The treatment objectives were to align or decrowd upper and lower arches, to obtain ideal overjet and overbite, to maintain class I molar and canine relationship and functionally stable occlusion, to obtain esthetically pleasing smile.
Treatment plan involved all first pre-molar and retained deciduous left canine extraction, decrowding of upper and lower arch with individual canine retraction using T- loop (maximum anchorage). And appliance used was edgewise 0.22 slot MBT prescription.
Treatment Progress
The maxillary and mandibular first molars were banded, with .022″ X .028″ X .050″ double tubes. Segmental arch wire technique i.e., burstone T-looped used for individual canine retraction (Fig.1b).
 |
Figure 1b: Segmental arch wire technique
|
After 3-months upper and lower continuous initial wire 0.14 HANT was place and to reinforce the anchorage in upper arch transpalatal arch was used.
After one month upper 17 x 25 stainless steel base arch wire used with overlay 0.14 HANT with open coil spring with respect to 11 and 22 and lower 0.18 stainless steel wire placed.
Following 1 month later, for 21 E-chain was placed mesial wing to 11 and from distal wing blue elastic was placed inter arch on 33 (Fig. 1c).
 |
Figure 1c: 21 E-chain placed on mesial wing to 11 and from distal wing blue elastic placed on inter arch on 33
|
Presently status achieved is an ideal overjet and overbite with class I canine and molar relationship (Fig.1d) and treatment is in progress. However, as the tooth 21 was ectopically erupted and corrected orthodontically, a periodontal opinion was sought.
 |
Figure 1d: Present status after achieving ideal overbite and overjet
|
Periodontal Intervention
The patient was referred for periodontal opinion regarding the status of tooth 21. On examination the tooth was found to have a periodontal pocket measuring 6mm (fig 2a) and the tooth was found to be non vital. The IOPAR i.r.t. 21 revealed that the tooth had a dilacerated root(fig 2b). The further periodontal therapy was delayed until the completion of endodontic treatment. After the endodontic treatment was completed the patient was prepared for the periodontal surgery after the routine phase I therapy. The complete hemogram revealed the patient’s healthy status.
 |
Figure 2a: Periodontal pocket measuring 6mm
|
 |
Figure 2b: IOPAR i.r.t. 21 revealed dilacerated root
|
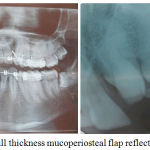 |
Figure 2c: Full thickness mucoperiosteal flap reflected
|
 |
Figure 2d: Dilaceration seen
|
The surgical area of interest was anaesthetized with local infiltrations and anterior palatine block using 2 % lignocaine and 1:80000 adrenaline. A full thickness mucoperiosteal flap was reflected (fig 2c). On reflection the labial plate of bone i.r.t. 21 was found to be completely resorbed and the root tip revealed the dilacerations (fig 2d). The dilacerated portion of the root was smoothened (fig 2e) and the exposed root apex was sealed with glass ionomer cement (fig 2f). Perioglas® bone graft was placed i.r.t. 21 and Periocol® GTR was positioned to cover the graft particles and sutured with interrupted and sling sutures (fig 2g). Finally the flap was repositioned and sutured with absorbable 5-0 vicryl sutures (fig 2h). A periodontal pack (Coe pack) was used to cover the surgical area (fig 2i). Antibiotics and analgesics were prescribed for the patient. The patient was also instructed to use chlorhexidine mouthwash. At 10 days follow up the periodontal pack was removed and the operated area revealed satisfactory. The sutures were however left in place to resorb to avoid disturbing the GTR.
 |
Figure 2e: smoothening of dilacerations
|
 |
Figure 2f: Exposed root apex sealed with glass ionomer cement
|
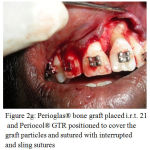 |
Figure 2g: Perioglas® bone graft placed i.r.t. 21 and Periocol® GTR positioned to cover the graft particles and sutured with interrupted and sling sutures
|
 |
Figure 2h: Flap repositioned and sutured with absorbable 5-0 vicryl sutures
|
 |
Figure 2i: Periodontal pack (Coe pack) placed
|
Presently, the patient is being followed-up with recall visits being scheduled at every 3 months (fig 2j). The first 3 months recall visit clinically showed 1mm gingival recession.
 |
Figure 2j: Post op after 3 months follow up of periodontal surgery
|
Discussion
The maxillary incisors and canines, often referred to as the ‘social six’, are the most prominent teeth in an individual’s smile. They are also the teeth that are on maximum display during speech in most individuals. The normal eruption, position and morphology of these teeth are crucial to facial esthetics and phonetics. The clinician is often faced with challenging situations where deviations from the normal eruption sequence, position or abnormalities in morphology are observed. Deviations in eruption of the incisors are a frequent clinical presentation. Since eruption has a strong influence on the craniofacial development and incisors are amongst the first teeth to erupt in both the primary and permanent dentition, eruption disturbances of the incisors can be a harbinger of a local or systemic condition.3
Ectopic eruption refers to the eruption of a tooth in a position that is not its normal position in the dental arch. Theories have attempted to explain the etiology of ectopic eruption. However, the multifactorial process of growth and development makes it difficult to identify specific primary etiological factors of ectopic eruption. The prevalence of ectopic eruption has been reported to be 5.6% and the majority of these are permanent central incisors. 3 The present case report also showed a similar situation where the maxillary left central incisor showed ectopic eruption at the vestibular depth.
Orthodontic treatment aims at providing an acceptable functional and aesthetic occlusion with appropriate tooth movements. These movements are strongly related to interactions of teeth with their supportive periodontal tissues. Experimental studies have shown that loss of periodontal attachment does not occur during orthodontic tooth movement provided the periodontium is maintained in a state of health. Accordingly, the variable loss of periodontal support observed in clinical studies may reflect the hygiene challenge associated with fixed orthodontic appliances. Maintaining adequate plaque control around a labially placed incisor may be particularly difficult due to the combination of its position, and the irritation from orthodontic attachments.4 The results from our study proved that orthodontic alignment of labially placed incisor is associated with loss of periodontal support. Appliances and attachments frequently cross the embrasure and may increase the tendency for inflammation. 4 The present results indicate a significant loss of periodontal attachment of the incisor after completion of orthodontic treatment, without significant deepening of pockets on the labial side, but showing slightly deeper pockets and significant bone loss on the mesial side. Also, there was a dehiscence noted on the labial surface of root associated with a dilacerated root.
A recent clinical study concluded that the risk of pulp damage from orthodontic treatment is minor in the average patient.5 However, the possibility of pulp changes may exist in individual cases where large amounts of tooth movement are required.6 The present case also confirmed that excessive tooth movement increases the risk of pulpal changes, with pulpal obliteration. Thus root canal treatment was completed prior to periodontal intervention. This finding supports results of experimental studies, and suggests that extreme types of tooth movement may cause changes in pulpal blood flow. However, the relationship between the magnitude of vascular impairment and the onset of pulpal changes remain undetermined.
The treatment plan established for the present case was an endodontic intervention followed by periodontal flap surgery, with an attempt for regeneration using Perioglas® bone graft and Periocol® GTR.
The 3 month recall visit clinically showed 1mm gingival recession. This has been supported by Aldritt et al 1968 and Lost et al 1984, where they proposed that the classic developmental defect which is thought to predispose to gingival recession is dehiscence. Anatomically dehiscence may be present where, because of the direction of tooth eruption or other developmental changes, the root has become placed more bucally or lingually to adjacent teeth so that cervical portion protrudes through the crestal bone. Dehiscences may be present where bucco-lingual thickness of a root is similar to or exceeds, the crestal bone thickness. Olsen and Lindhe (1991) considered that morphological biotypes characterized by narrow long teeth are more prone to dehiscences than individuals with broad short teeth.7
Conclusion
At the present time, there is little evidence to indicate that orthodontic treatment will either enhance or detract from the periodontal health of the patient or that it will increase or decrease the longevity of the teeth. However, much of the orthodontic treatment is undertaken on an esthetic or empirical basis. The orthodontist should make certain that teeth are being moved into a greater volume of bone. The bite plane is of great value in allowing continuous eruption of the teeth and their supporting structures and in eliminating additional trauma by enabling the teeth to move into their correct cusp-fossa relationships unimpeded by the inclined planes of the opposing teeth, the knowledge of which is of great value for an orthodontist. In spite of the lack of knowledge about the interrelationships between orthodontic treatment and periodontal health and disease, the general practitioners and the various specialists of dentistry, each seeking a rationale for their preventive and therapeutic procedures, subject the patient to treatment based on concepts of the occlusion which have yet to be corroborated. In addition to the need for research in this field, a common language between the periodontist and the orthodontist must be established to eliminate the existing communications barrier. Once basic principles can be determined, elucidated, and applied correctly, the periodontal complications after movement of teeth into proper alignment can be better dealt with a combined teamed approach of an orthodontist and periodontist.
References
- Burden D.,Harper C., Mitchell L.,Mitchell N., and Richmond S. Management of unerupted maxillary incisors, in National Clinical Guidelines 1997, ed. Faculty of Dental Surgery, Royal College of Surgeons of England, London, Chapter 2, section II. 1997.
- DiBiase D. Midline supernumeraries and eruption of maxillary central incisors, Trans. Br. Soc. Study Orthod. 1969;55:83-88.
- Kristin L. H., Suri L. Eruption disturbances of maxillary incisors: A Literature Review. J Clin Pediatr Dent. 2008;32(3):221-230.
CrossRef - Woloshyn H., Artun J. Pulpal and periodontal reactions to orthodontic alignment of palatally impacted canines. Angle orthod. 1994;64(4):257-264.
- Popp T. W., Artun J. Pulpal response to orthodontic tooth movements in adolescents: A Radiographic study. Am J Orthodon. 1992;101:228-233.
CrossRef - Azaz B., Steinman Z. The sequelae of surgical exposure of unerupted teeth. J Oral Surgery. 1980;38:121-127.
- Smith R. J. Gingival recession: Reappraisal of an enigmatic condition and a new index for monitoring. J Clin Periodontol. 1997;24:201-205.
CrossRef

