
I. Made Pande Dwipayana1, I. B. Aditya Nugraha1, Siswadi Semadi1 and I. Made Suma Wirawan2
1Division of Endocrine and Metabolic, Department of Internal Medicine, Faculty of Medicine, Udayana University-Sanglah General Hospital Denpasar Bali.
2Faculty of Medicine, Udayana University Denpasar Bali.
Corresponding Author E-mail: dwipayanapande@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1232
Abstract
Male 33 years old patient came with complaint of fever. Positive NS1 and DEN-3 dengue virus were revealed. Patient also with multiple nodules thyroid gland with increased of thyroxine hormone level and Burch Wartofsky 45. Patient was dignosed of thyroid crisis triggered by Den-3 serotype of dengue virus. It was life-threatening case and treated at high care unit. Early diagnosed and prompt treatment safe patient life.
Keywords
DEN-3 serotype dengue virus; multiple nodules thyroid Thyroid crisis; thyroxine hormone;
Download this article as:| Copy the following to cite this article: Dwipayana I. M. P, Nugraha I. B. A, Semadi S, Wirawan I. M. S. Thyroid Crisis in A Toxic Multinodular Goiter Patient Triggered by A Den-3 Subtype Dengue Infection. Biomed Pharmacol J 2017;10(3). |
| Copy the following to cite this URL: Dwipayana I. M. P, Nugraha I. B. A, Semadi S, Wirawan I. M. S. Thyroid Crisis in A Toxic Multinodular Goiter Patient Triggered by A Den-3 Subtype Dengue Infection. Biomed Pharmacol J 2017;10(3). Available from: http://biomedpharmajournal.org/?p=16669 |
Introduction
Thyroid crisis is ranked first in the spectrum of endocrine emergency. The incidence of this case is rare, not more than 10% of patients treated with thyrotoxicosis. However, the mortality rate is quite high with a range of 20-30%. Clinical presentations include fever, tachycardia, hypertension, neurological and gastrointestinal abnormalities.1
Thyroid crisis generally occurs in patients with hyperthyroidism who are not given adequate therapy and are triggered by an uncontrolled infection, trauma, thyroid surgery, or diabetes mellitus. There is no single biochemical indicator capable of predicting thyroid crisis, so our actions depend on clinical sign. With a high mortality rate, suspicion of thyroid crisis is enough to become the basis for aggressive action. Patients usually show a hyper metabolic state which is characterized by high fever, tachycardia, nausea, vomiting, agitation, and psychosis. In the advanced phase, the patient may fall in a stupor or coma accompanied by hypotension.1,2
Infection as one of the things that can trigger a thyroid crisis need to get a special attention, for instance dengue virus infection. In general, dengue infection is rare infection that can cause or trigger the emergence of diseases or abnormalities in the field of thyroid. There have been reported only 2 cases of dengue fever in the presence of a thyroiditis in Pakistan in 2012, as well as India in 2013. It is one of the many consideration for the author to report this case in order to increase awareness and share knowledge about what factors affects and how to treat a thyroid crisis case.1-4
Case
Adult male patient, 33 years old, came with a chief complaint of an acute fever. Fever is said to appear suddenly start 5 days before entering the hospital. When the fever began to appear, patient also complaint of having a restless, sudden decreased of consciousness, and delirious. In addition to the fever of the patient also complained of trembling hands and heart pounding. These two symptom appeared simultaneously with the fever. In addition to all of these complaints patients also complained of decreased appetite, and experienced nausea and vomiting. Nausea and vomiting lasted almost every after meal. Three days before being taken to the emergency unit of district hospital, the patient was taken to the internal medicine polyclinic and was advised to do thyroid studies by doing thyroid hormones examination. The result there was an increase in the value of thyroid function. There was no family history of thyroid disorders.
The general condition of patients was in moderate illness, fully alert (Glasgow Comma Scale E4V5M6), blood pressure 100/80 mmHg, with axilla temperature 37.70C, with the pulse rate 110x/minute, respiration frequency 22x/minute, with oxygen saturation of 98%.
On physical examination of the eye was not anemic nor jaundice, with normal pupil reflex, and exophthalmic looks of both eyeballs. Examination of the throat ear and nose was normal with Jugular Venous Pressure (JVP) ± 0 cmH20, calm impression, neck examination, on the inspection got the impression of enlargement on the thyroid gland, the palpation obtained the enlarged thyroid gland multiple nodules with the largest diameter 3 cm, with soft consistency.
On examination of the heart and lungs obtained impression frequency irregular heart rate, increased, 110x/minute, without murmur, ronchi, or wheezing. On abdominal examination no distension is found, auscultation sounds normal bowel sounds, palpation is not obtained by mass, liver and lien is not palpable, percussion is found tympanic in all areas of the stomach. The extremities are palpably warm and moist due to sweat, no tremor is found. Burch Wartofsky score calculation got value 45.
From the initial complete blood test, the leukocyte count was 4.86 x 10 μg / μL, hemoglobin 16.3 gram / dl, hematocrit 46.5%, platelet 157 x 10³ / μL. In blood chemistry examination was obtained SGOT 637 U / L, SGPT 403 U / L, BUN 7.61 mg / dl, creatinine 1.0 mg / dl, blood sugar at 107 mg / dl, FT4> 100.0 pmol / L ( 12.8 to 20.4 pmol / L), TSHs <0.05μU / ml (0.3-4.2μU / ml), sodium 138 mmol / L, potassium 4.0 mmol / L, chloride 97 mmol / L .
Because initially the patient complained of fever, with a pattern of fever that resembles the dengue heat pattern, had also done the examination of Non Structural Antigen 1 (NS1) and obtained positive NS1 results.
ECG examination shows atrial fibrillation with rapid ventricular response with a rate range of 110-120 times per minute. On thyroid ultrasound (ultrasound) examination, there is a conclusion of the multi-nodular right and left goiter.
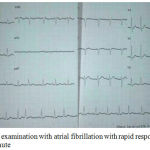 |
Figure 1: ECG examination with atrial fibrillation with rapid response of rate 110-120 x / minute
|
From the data obtained from the history, the physical examination and investigation of the patient were then diagnosed early with a thyroid crisis with suspicion of multinodular toxic strum (Plummer disease) triggered by dengue virus infection.
Initially management was a closed observation in the Emergency Room (ER) and given initial treatment with IVFD Ringer Lactat 30 drip per minute, O2 administration with 2-4 liters per minute, intravenous 2 x 62.5 mg intravenous methylprednisolone, ceftriaxone 2×1 gram intravenous injection, propranolol 40 mg orally every 6 hours (via nasogastric tube (NGT) because patients was unable to eat and nausea vomiting constantly), 4 mg intravenous injection ondancentron for patients with severe nausea and vomiting, prophyltyuracyl (PTU) tablets 3×200 mg orally, Installation of dower catheters, and patients are planned to be treated in intensive care unit.
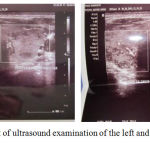 |
Figure 2: Result of ultrasound examination of the left and right thyroid of the patient
|
In third day of treatment there was already an improvement in level of consciousness (GCS E4V5M6), BP = 130/90 mmHg, pulse = 90x / min, normal sinus ECG description with HR = 92x / min, the patient was eventually transferred to the usual treatment room. The results of the complete blood serial examination as follows: leukocyte count 2.23 x 10³ / μL, hemoglobin 16.0 grams / dl, hematocrit 45.4%, platelets 126 x 10³ / μL.
In the fourth day of treatment found the condition of patients with no fever, NGT has been revoked and patient was able to diet liquid. Examination of vital signs showed good progress with GCS E4V5M6, BP = 120/80 mmHg, pulse = 92x / min, normal sinus ECG description with HR = 88x / min. Full blood serum examination result as follows: leukocyte count 1.72 X 10³ / μL, hemoglobin 15.4 grams / dl, hematocrit 44.4%, platelet 64 x 10³ / μL.
On the fifth day of treatment patient with conditions that are still the same as the previous day. From examination of vital signs showed good development with GCS E4V5M6, BP = 130/70 mmHg, pulse = 90x / min, normal sinus rhythm on ECG description with HR = 88x / min. Full blood serum examination as follows: leukocyte count 5.33 x 10³ / μL, hemoglobin 16.48 grams / dl, hematocrit 47.8%, platelet 31 x 10³ / μL. Monitoring is also performed for signs of warning sign dengue, monitoring the balance of liquid obtained balance +500 cc.
On the seventh day of treatment, dengue serologic examination was performed and the complete blood serial examination was performed as follows: IgG anti dengue (+), IgM anti dengue (+), with virus serotype showing DEN-3 type. Complete blood count with leukocyte count 1.72 x 10³ / μL, hemoglobin 15.4 gram / dl, hematocrit 44.4%, platelet count 64 x 10³ / μL.
On day eight day of treatment with improved clinical parameters, as well as full blood examination show results of an improvement by an increase of platelet level and decreased of hematocrit, eventually the patient was discharged and advised to keep control to the polyclinic part of the disease within 3 days after outpatient. The results of laboratory tests on the last day are as follows: leukocyte count 1,85 x 10³ / μL, hemoglobin 15.0 gram / dl, hematocrit 43.5%, platelet 85 x 10³ / μL. For oral therapy at the time of discharge patient was given propranolol tablets 3×10 mg per oral, and with prophyltyuracyl (PTU) tablets 3×200 mg orally, and roburantia 1×1 tablet.
One month after being discharged, the patient is advised to perform thyroid function checks (TSHs and FT4). At the time of subsequent control re-examination of thyroid function, obtained levels of 0.018 μIU / mL of TSHs (0.270-4.700 μIU / mL) while FT4 levels 2.87 ng / dL (0.933-1.200 ng / dL). Administration of propanololol was followed by a dose of 3×10 mg, and PTU with a dose of 3 × 200 mg. The last follow up in August 2015 was examined for FT4 levels obtained results 0.868 (0.933-1,200 ng / dL) PTU dose was reduced to 2×200 mg.
Discussion
Thyroid hormone is one of the hormones in the body that function is to regulate metabolism function to keep running normally. However, if there is an aberration or disruption of dams and production processes this will cause a dysregulation or abnormalities of its quantity in the body. A hyperthyroid state can be fatal and life-threatening. This is often referred to as thyroid crisis.1,3
The term hyperthyroidism and thyrotoxicosis are often mistaken in its use. Thyrotoxicosis is a term related to a physiological and biochemical complex that is found when a tissue gets excessive thyroid hormone in any source. While hyperthyroidism is a result of an increase production of thyroid hormone itself. Thyrotoxicosis is divided into abnormalities associated with hyperthyroidism and those not associated with hyperthyroidism. The most common cause of hyperthyroidism is Graves’ disease which is approximately ± 90%.2,3,4. Subsequent causes by toxic solitary adenomas or toxic multinodular goiter. Other causes of hyperthyroidism include hypersecretion of thyroid carcinoma, thyrothropin-secreting pituitary adenoma, teratoma, HCG-secreting hydatiform mole. Giving interferon-α and interleukin-2 can disrupt the thyroxine bond with globulin so that free thyroxine levels increase so that it can trigger the occurrence of hyperthyroidism that if not handled properly will trigger thyroid crisis.1 The following describes some of the causes of hyperthyroidism as listed in Table 1.
Table 1: Hyperthyroid Etiology (1)
| Common | Grave Disease
Toxic Thyroid Nodule |
| Uncommon | Neonatal Hyperthyroidism
Inappropriate TSH secretion by the pituitary which can be caused by tumor condition, or non-tumor (thyroid hormone resistance syndrome) Exogenous Iodine |
| Rare | Metastatis thyroid cancer
Choriocarcinoma and Mola Hydatidosa Ovarium Struma Testicular embryonal carcinoma Pilyostotic fibrous dysplasia (Syndrome Mc-Cune Albright) |
Several factors can trigger thyrotoxicosis into a thyroid crisis such as: surgery, trauma, myocardial infarction, pulmonary embolism, cerebrovascular disorders, diabetic ketoacidosis, toxemia gravidarum, and infection. Disobedience in taking thyroid medication, coupled with inadequate dosage therapy may also affect the occurrence of this thyroid crisis. 1,2,4Various signs and symptoms of thyrotoxicosis can be seen in table 2 below.
Table 2: Sign and Symptoms of Thyrotoxicosis.1
| Organ System | Symtomps | Sign |
| Neuropsychiatric (Neuromuscular) | Emotional Instability
Anxiety Confusion Comma |
Muscle wasting
Hyperreflexia Tremor Periodic Paralysis |
| Gastrointestinal | Hyperdefecation
Diarrhea |
|
| Reproduction | Oligomenorrhea
Decrease of Libido |
Gynecomastia |
| Thyroid Gland | Neck fullness
Tenderness |
Bruit |
| Heart and Lung | Palpitation
Dyspnea Chest Pain |
Atrial fibrilattion
Sinus tachycardia Hyperdynamic precordium Congestive Heart Failure |
| Skin | Hair Loss | Pretibia myxedema
Warm, moist skin Erythema palmaris |
| Eye | Diplopia
Eye Iritation |
Exopthalmus
Ophtalmoplegia |
In this case the patient is treated with hyperthyroidism that is thought to be a toxic multi-nodular goiter (Plummer disease). This is supported by data that in the case occurs in adulthood, and obtained multiple nodules and from laboratory results lead to signs of hyperthyroidism. Hyperthyroidism in this case becomes a thyroid crisis which is caused by infection.Thyroid crisis is a severe and life-threatening clinical condition due to the acute exacerbation of thyrotoxicosis. Occurrence 1-2% of patients treated with or without prior anti thyroid treatment history before. The incidence of thyroid crisis mostly occurs in Graves Disease with history of dropouts of treatment or can also in an undiagnosed hyperthyroidism. Clinical symptoms that often arise are fever, sweating, tachycardia to atrial fibrillation, nausea, vomiting, diarrhea, agitation, and altered consciousness. Sometimes it can also be accompanied by jaundice which is a marker of a poor prognosis. In a thyroid crisis, a pattern of elevated T4 and T3 levels is free with suppression of thyrotropin (<0.05μU / mL) levels comparable to those hormone levels at thyrotoxicosis. After the synthesis of the thyroid hormone, the main thyroid gland secretes T4. It is estimated that 80% of circulating T3 is derived from T4 monodeiodination in peripheral tissue, whereas only 20% of T 3 is produced directly by the thyroid gland.11
Infection becomes one of the factors that trigger the occurrence of thyroid crisis. From the literature we get it is indeed a viral infection as one of the factors that trigger the occurrence of thyroiditis which in turn can trigger the occurrence of thyroid crisis. Infection by dengue virus is suspected to cause disturbance to the thyroid metabolism itself so it is suspected to be one cause of thyroid crisis.13,4
This immunopathological mechanism of dengue virus work can also explain how regulatory changes or thyroid hormone regulation occur especially in cases of thyroid crisis. There is not much literature or source specifically explaining the case, but it is explained in the case of acute infection of dengue virus itself that a rapid decrease in serum T3 is more or less occurring within 24 hours, which is also due to a decrease in the conversion of T4 to T3, Turnover of the thyroid hormone itself. In accordance with several theories about the pathogenesis of dengue hemorrhagic fever is also explained about the involvement of the humoral immune response in the pathogenesis of dengue. Humoral response in the form of antibodies that play a role in the process of neutralization of the virus. Antibodies against this dengue virus play a role in accelerating viral replication in monocytes or macrophages. This hypothesis is called antibody dependent enhancement (ADE). Both T-helper (CD-4) and T-cytotoxic (CD-8) lymphocytes play a role in cellular immune response to dengue virus. T-helper differentiation ie TH1 will produce IFN-γ, IL-2, and lymphocyte. The TH2 will produce IL-4, IL-5, IL-6, and IL-10. Monocytes and macrophages that will phagocytosis the virus by opsonization by antibodies. However, this phagocytosis process actually causes increased viral replication and cytokine secretion by macrophages. This is also in consistent with the results of several studies in dengue hemorrhagic cases where it showed by producing some pro-inflammatory cytokines such as IL-1, and IL-6, and TNF plays an important role in the decline of T3 function, thereby disrupting the hypothalamic-pituitary axis -and thyroid gland itself. 9,10,11
In these thyroid crisis situations, there can also be several findings from laboratories associated with thyrotoxicosis, such as hyperglycaemia, hypercalcemia, leukocytosis, liver enzyme abnormalities, elevated alkaline phosphatase enzymes, and increased glycogenolysis.11
In some places with inadequate laboratory facilities, for diagnosis of suspected thyroid crises may use diagnostic criteria from Burch-Wartofksy in 1993 as in Table 3 below. This is especially important because with earlier diagnosis will determine the next step in therapy so as to prevent the risk of worse mortality.11
Tabel 3: Burch-Wartofsky criteria for thyroid crisis diagnosis. 11
| Heat control dysfunction | Cardiovascular dysfunction |
| Temperature (in 0 Fahrenheit) | Tachycardia ( in times/minute) |
| 99-99,0 5 | 99-109 5 |
| 100-100,9 10 | 110-119 10 |
| 101-101,9 15 | 120-129 15 |
| 102-102,9 20 | 130-139 20 |
| 103-103,9 25 | >140 25 |
| >104,0 30 | Congestive Heart Failure (CHF) |
| Effect on central nervous system | No CHF 0 |
| No effect 0 | Mild (leg edema) 5 |
| Mild(agitation) 10 | Moderate (basal rhonchi) 10 |
| Moderate(delirium,severe lethargic) 20 | Severe (lung edema) 15 |
| Severe(coma,seizure) 30 | Atrial Fibrilation |
| Gastrointestinal-liver dysfunction | No Atrial Fibrillation 0 |
| No dysfunction 0 | Yes 10 |
| Mild(diarrhea,nausea/vomit) 10 | History of trigger |
| Severe(unclear cause of icteric) 20 | |
| Negative 0 | |
| Positive 10 |
Score interpretation : ≥45 highly suggestive ; 25-44 suggestive of impending storm ; <25 unlikely thyroid storm
In the case obtained of Burch-Wartofsky score criteria scored 45, obtained with details for the score of respiratory function regulation setting with a score of 10 (temperature axilla 39.5ºC), then early admission with delirium with score 20, and on the dysfunction score Cardiovascular with a tachycardia condition 110-119 times per minute with a score of 10, with a total score of 45 indicating a very highly suggestive for thyroid crisis.
The treatment of choice in patients with thyroid crisis is the same as the treatment given to patients with hyperthyroidism, but the medication is given in higher dosage and the longer of time interval that is given. In patients with thyroid crisis should be immediately addressed to the emergency department or ICU. Diagnosis and therapy as soon as possible in patients with thyroid crisis is important to reduce morbidity and mortality from this disorder.12-15
In the case of thyroid crisis, hyperpyrexia should be treated promptly. In this case the administration of the drug type of acetaminophen is preferred over aspirin which can increase serum T3 and T4 free concentration. The administration of beta-blockers is an important primary therapy in the treatment of most patients with hyperthyroidism. Propanolol is the first choice drug used as an initial which can be given intravenously. The given dose is 1mg / min to several mg until the desired effect is achieved or 2-4 mg / 4hr intravenously or 60-80 mg / 4hr orally or via nasogastric tube (NGT).13-15
Administration of tionamide such as methimazole or PTU is to block the hormone synthesis. Tionamide blocks the synthesis of thyroid hormone within 1-2 hours of admission. However, tionamide has no effect on synthesized thyroid hormones. Some approaches using PTU rather than tionamide as an option in thyroid crisis because PTU can block the conversion of T4 to T3 at the peripheral level. Methimazole has a longer duration time than PTU so it is more effective. The administration of glucocorticoids also decreases the conversion of T4 to T3 and has a direct effect in the autoimmune process if thyroid crisis stems from Graves’ disease. The dose used is 100 mg / 6-8 hours intravenously in the case of thyroid crisis. Where stable, hydrocortisone 15-30 mg orally per day or equivalent dose: prednisone 5-7.5 mg orally / day, dexamethasone 0.75-1.25 mg orally / day. Doses can be given once a day (morning) or divided with more morning doses of the afternoon.11-14
In the management of the patient has been performed according to the theory by giving IVFD Ringer Lactate 30 drip per minute, giving oxygen with 2-4 liters per minute, methylprednisolone injection 2 x 62.5 mg intravenously, ceftriaxone 2×1 gram intravenous injection, propranolol tablet 3×10 mg orally (via NGT because patients cannot eat and nausea vomiting constantly), 4 mg intravenous injection ondancentron for patients with severe nausea and vomiting, diazepam 2mg intravenous injection when patients are agitated, prophyltyuracyl (PTU) tablets 3×200 mg orally, dower catheter insertion, and patients are planned to be treated in intensive care unit ward.
Investigation for the causative agent of thyroid crisis is conducted, where suspected of infection due to dengue virus. NS1 examination was performed on day 1 of fever with positive results, and serology, and antibodies obtained serotype DEN-3 virus, and IgG and IgM positive on day 8 treatment with clinical symptoms of fever starting 5 days before MRS, with clinical weakness, decreased appetite, whole body pain, and in the laboratory there was a decrease in platelet levels, and elevated hematocrit levels according to the diagnosis of dengue hemorrhagic fever. For further management has also been submitted to the intensive care unit ward, so it can be monitored more closely. At follow up therapy the patient is found to be in improved condition and was discharged on the 8th day of treatment. Monthly monitoring is recommended for patients in the internal medicine polyclinic for evaluating of thyroid function.
Conclusion
It has been reported a case of an adult men, 33 years of age, with a diagnosis of thyroid crisis with a toxic multi nodular goiter triggered by dengue virus infection. Thyroid crisis is a condition of thyrotoxicosis which suddenly worsen and accompanied by among others the existence of fever, delirium, tachycardia, severe dehydration and can be triggered by among others: infection and surgery. Dengue virus infection itself as one of the causes that can cause the incidence of this thyroid crisis. Proper diagnosis and management is very important to prevent the occurrence of mortality.
Refferences
- Talib S. H., Sainani R., Chordiya A. Expanded Dengue Syndrome : Presenting as Overt Thyrotoxicosis without stigmata og Graves disease ( A Case Report). JDMS. 2013;5(3):4-6.
- Bahn R. S., Burch H. B., Cooper D., Garber J. R., Greenle C. M., Klein I., et al. Hyperthroidism and Other Causes of Thyrotoxicosis : Management Guidelines of The American Thyroid Association and American Association of Clinical Endocrinologists. Endocr. Pract. 2013;17(3):1-65.
- Desailloud R., Hober D. Viruses and thyroiditis : an update Review. Vir. J. 2009;6(5):1-14.
CrossRef - Wacharasindhu S., Bunjobpudsa Y., Tongmeesee S. Endocrine changes in children with dengue virus infection. Asian Biomedicine. 2009;3(5):557-61.
- Lee L. S., Guzman M. G.,Martinez E., Tan L. H., Hung N. T. Overview, differential diagnosis, and dengue diagnostics. In: Akbar N, Aloun DS, eds. Handbook For Clinical Management of Dengue. 1st Genewa : WHO-TDR Publication. 2012:1-20.
- Guzman M. G., Rosario D., Kouri G. Molecular Biology of the Flaviviruses. In: Kalitzky M., Borowski P., eds. Diagnosis of dengue virus infection. 1st London. Horizon Bioscience. 2009:21-40.
- Kumarasamy V. Evaluation of a commercial dengue NS1 antigen-capture ELISA for laboratory diagnosis of acute dengue virus infection. J. Vir. Methods. 2007;140(1):75-9.
CrossRef - Varquez S. Serological Markers during dengue 3 primary and secondary infections. J. Clin. Vir. 2005;32:132-37.
CrossRef - Juffrie M., Meer G. M., Hack C. E., Hassnoot K., Veerman A. J., Thijs L. G. Inflammatory Mediators in dengue virus infection in children : Interleukin-6 and it’s relation to C-Reactive Protein and Secretory Phospholipase A2. Am. J. Trop.ed. Hyg M. 2001;65:70-5.
CrossRef - Langouche L., Berghe V. The dynamic neuroendocrine response to critical illness. Endocrinol. Metab. Clin. N. Am. 2006;35:777-91.
CrossRef - Migneco A., Ojetti V., Testa A., Lorenzo D., Silveri N. G. Management of thyrotoxic crisis. Eur. Rev. Med. Pharmacol. 2005; 9: 69-74.
- Sarlis JN, Gourgitotis F. Thyroid Emergencies. Rev. End. Metab. Dis. 2003;4:129-36.
CrossRef - Jiang Y., Karen A. H., Bartelloni P. Thyroid Storm Presenting as Multiple Organ Dysfunction Syndrome. Chest. 2000;118:877-79.
CrossRef - Djokomoeljianto R.,Tiroid K.,dan Hipertiroidisme H. In : Sudoyo A. W., Setiyohadi B., eds. Buku Ajar Ilmu Penyakit Dalam. 5th Jakarta : Interna Publishing. 2009:1993-2008.
- Jameson L., Weetman A. Disorders of the thyroid gland. In: Branwald E., Fauci A., Kasper D., eds. Harrison Principles of Internal Medicine. 18th New York: McGraw-Hill. 2011;2060-84.

