
Dhanraj M1, Abinaya. K1 and Ashish. R. Jain2
1Department of Prosthodontics, Saveetha Dental College and Hospitals Chennai, India.
2Department of Prosthodontics, Saveetha Dental College, and hospitals, saveetha University, Chennai, India.
Corresponding Author E-mail: dr.ashishjain_r@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/1267
Abstract
To assess the knowledge, attitude and practice among dental practitioners regarding management of short abutments receiving complete veneer crowns. A cross sectional survey was conducted with a pre-tested structured questionnaire containing 18 composite choice based questions among 250 practicing dentists on management of failed complete veneer crowns over short clinical abutments. Pertinent data were extracted and analyzed. 74% practitioners have agreed on modifying their tooth preparation after failure to enhance retention. 14.8% of the survey participants agreed on having performed crown lengthening for the same. 5.2% of the practitioners had performed orthodontic extrusion for the same. 20% reported to having relieved prematurities and 74% had stated to have relieved them out of occlusion. While 67% of them had tried post and core restorations to manage the same. Accomplishing retention in complete veneer crowns placed over short abutments has always posed a great challenge to the clinician. The knowledge and awareness level elicited in this questionnaire study is moderate. Hence more awareness programs and hands-on clinical training needs to be conducted to address this.
Keywords
Abutments; Crown Lengthening; Orthodontic Extrusion; Retention; Short Clinical Crowns
Download this article as:| Copy the following to cite this article: Dhanraj M, Abinaya K, Jain A. R. Management of Short Abutments Receiving Complete Veneer Crowns-A Cross Sectional Survey. Biomed Pharmacol J 2017;10(3). |
| Copy the following to cite this URL: Dhanraj M, Abinaya K, Jain A. R. Management of Short Abutments Receiving Complete Veneer Crowns-A Cross Sectional Survey. Biomed Pharmacol J 2017;10(3). Available from: http://biomedpharmajournal.org/?p=15953 |
Introduction
Fixed dental prosthesis being one of the preferred fixed modalities in replacement of missing teeth, has its limitations and difficulties in compromised clinical scenarios. One such scenario is availability of clinical crown height of potential abutments being shorter than ideal requirement. A short clinical crown is defined as any tooth with less than 2 mm of sound, opposing parallel walls remaining after occlusal and axial reduction.1 With occlusal wear of abutment teeth due to severe attrition, reduction in clinical crown height with root canal treatment, presence of wear facets opposing a plunger cusp, supra eruption of potential abutment teeth owing to long standing absence of opposing edentulous space which requires extensive preparation of abutment teeth to achieve adequate clearance, extensive carious lesions and compromised anatomy of the abutment tooth, the clinician encounters marked difficulties in providing a prosthesis with good prognosis.2,3 Caries, erosion, bruxism, tooth malformation, tooth malposition, fracture, eruption disharmony, exostosis, genetic variations in addition to the above contribute to the etiology of short clinical crowns.4-8It is in such cases that a compromise in the retention form and the resistance form are being encountered. With a normal preparation in such cases, dislodgement of the crown provided owing to inadequacy in the preparation with respect to retention and resistance form may be anticipated. It is then that the clinician starts relying on the luting cement to combat this undesirable outcome.9 Mechanical lack of retention, often observed in case of short clinical crowns, accounted for over two-thirds of failed units.10 With an array of difficulties faced post-restoration of abutment with short clinical crowns, it becomes a bitter experience for the patient and a matter of hassle for the clinician in the long run. Hence it is paramount the clinicians should be aware of the various remedial measures such as tooth preparation modification, crown lengthening, post and core preparation, orthodontic extrusion, which may be resorted to combat the compromises that would be foreseen with a conventional preparation.4,11,12,13
AIM
To assess the knowledge, attitude and practice among dental practitioners regarding management of short abutments receiving complete veneer crowns.
Methodology
A cross-sectional questionnaire based survey was performed among 250 participants. The survey was chiefly exploring the ways that clinicians used as remedial measures when they encountered short clinical crowns. Survey instrument was a structured questionnaire pre-tested by ten randomly chosen practicing dentists who were not included in the list of participants chosen. A list of practicing dentists across various districts was procured from the state dental association. Two hundred and eighty dentists falling within the inclusion criteria were retrieved in random and were mailed inquiring their consent towards participating in the questionnaire study. Two hundred and fifty willing participants were then provided with a questionnaire. The inclusion criteria were practicing dentists of both genders and all specialties falling under all age groups. The exclusion criteria included non-willingness of the subject to participate.Cronbach’s α determination was performed to measure the internal consistency among the surveyed items to assess the reliability of the questionnaire. The Cronbach’s α calculated was 0.84.The study was approved by the Institutional Human Ethical and Scientific Committee of the University and informed consent was obtained from the respondents and complete confidentiality about identity and responses was ensured.A response rate of 100% was obtained from the included respondents, of which 73.6% were male and 26.4% were female. The questionnaire had 18 standardized, pretested questions with both multiple choice and descriptive areas (Table I).There were no drop outs and no incomplete answers provided by the participants in the study performed.The first part of the questionnaire consisted of the demographic aspects (Table II) which consisted of the basic information of the practicing dentists including their gender and practice.This was followed by a core part which had questions being posed on management of short clinical crowns and the methods they preferred in their practice. They were also questioned on management of the cementation failures that they encountered (Table III).
Table 1:Sample Questionnaire Form
| S.No | Sample Questionnaire |
| 1. | How long have you been practicing?
a) 0-2 years b) 2-5 years c) 5-10 years d) 10-15 years |
| 2. | Have you treated patients with short clinical crowns for full coverage restorations?
a) Yes b) No |
| 3. | Have you experienced cementation failure in those crowns?
a) Yes b) No |
| 4. | How many times have you experienced failure?
a) Once b) Twice c) More than twice |
| 5. | Did you modify tooth preparation after failure?
a) Yes b) No |
| 6. | What modifications have you made?
a) Added grooves on either side b) Added grooves on both sides c) Prepared boxes |
| 7. | What other measures have you taken? |
| 8. | Have you changed the luting cements? If yes with what?
a) Yes – with resin modified GIC b) Yes – with resin cements c) No |
| 9. | What type of cement do you prefer for luting short crowns?
a) Resin cements b) Glass ionomer cement |
| 10. | Have you done crown lengthening for the same?
a) Yes b) No |
| 11. | Have you done osteoplasty along with crown lengthening?
a) Yes b) No |
| 12. | Have you done orthodontic extrusion?
a) Yes b) No |
| 13. | Have you given splinted crowns to manage the same?
a) Yes b) No |
| 14. | Have you done occlusal adjustments to manage this? If yes how?
a) Yes – by relieving prematurities b) Yes – by relieving it out of occlusion c) No |
| 15. | Have you given instructions regarding dietary practices on avoidance of sticky food? |
| 16. | Have you tried sand blasting the intaglio surfaces?
a) Yes b) No |
| 17. | Have you tried post and core restorations to manage the same?
a) Yes b) No |
| 18 | Have you placed or preferred sub gingival margins for the same?
a) Yes b) No |
Table 2: Demographic characteristics of the participants.
| S. No. | Demographic Data | Variables | Number (Percentage) |
| 1 | Gender | Male | 184 (73.6%) |
| Female | 66 (26.4%) | ||
| 2 | Age | 23 – 30 years | 70 (28%) |
| 30 – 40 years | 110 (44%) | ||
| 40 – 50 years | 45 (18%) | ||
| 50 – 60 years | 25 (10%) | ||
| 3 | Years of practice | 0 – 2 years | 78 (31.2%) |
| 2 – 5 years | 107 (42.8%) | ||
| 5 – 10 years | 41 (16.4%) | ||
| 10 – 15 years | 24 (9.6%) | ||
| 4 | Qualification | General Practitioner | 136 (54.4%) |
| Specialist | 114 (45.6%) |
Table 3: Responses to the questions
| S.No. | Question No. | Questions | Percentage | |
| Yes
(Percentage) |
No
(Percentage) |
|||
| 1 | Q2 | Treated patients with short clinical crowns | 246 (98.4%) | 4 (1.6) |
| 2 | Q3 | Cementation Failures | 39 (15.6%) | 211 (84.4) |
| 3 | Q5 | Tooth Preparation Modification | 185 (74%) | 65 (26%) |
| 4 | Q8 | Change of luting cements | 190 (76%) | 60 (24%) |
| 5 | Q10 | Crown lengthening | 37 (14.8%) | 213 (85.2%) |
| 6 | Q11 | Osteoplasty | 22 (8.8%) | 228 (91.2%) |
| 7 | Q12 | Orthodontic extrusion | 13 (5.2%) | 237 (94.8%) |
| 8 | Q13 | Splinted crowns | 45 (18%) | 205 (82%) |
| 9 | Q14 | Occlusal adjustments | 235 (94%) | 15 (6%) |
| 10 | Q15 | Dietary Practices | 210 (84%) | 40 (16%) |
| 11 | Q16 | Sandblasting of Intaglio Surfaces | 20 (8%) | 230 (92%) |
Results
A response rate of 100% was obtained from the included respondents, of which 73.6% were male and 26.4% were female.Out of the 250 dentists questioned 78 dentist were holding a practice ranging between 0-2 years, 107 were practicing for 2–5 years, 41 had a practice of 5-10 years and 24 of them had their practice falling between 10-15years.On questioning about them on providing full coverage restoration for patients with short clinical crown 246 of them gave an affirmative response and 4 of them stated they had no such experience.39 of the 250 respondents gave a history of experiencing cementation failures in those cases.On being questioned on the frequency of cementation failures experienced in such cases, 86% of them reported on having faced cementation failure once, 12% of them reported facing the same twice while 2% had faced cementation failure more than twice.74% practitioners have agreed on modifying their tooth preparation after failure to enhance retention (Fig. 1)
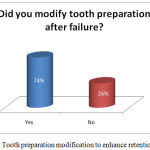 |
Figure 1: Tooth preparation modification to enhance retention. |
On being questioned on the type of modification performed, it was found that 64% added grooves on one of the either sides, 24% added grooves on both sides and 12% prepared boxes.
Other remedial measures taken were reported to be crown lengthening by 15%, orthodontic extrusion by 2%, placement of subgingival margins by 28% and changing to resin cements for luting by the rest (45%)A majority of the respondents agreed to change the luting cements, with 52% using resin cements and 24% preferring resin modified glass ionomer cement.On being questioned on the type of cements preferred for luting short crowns, 36% reported using resin cements and 64% reported of having used glass ionomer cement.14.8% of the survey participants agreed on having performed crown lengthening for the same (Fig. 2). 8.8% of the respondents have reported to have performed osteoplasty along with crown lengthening to gain height of the clinical crown.5.2% of the practitioners had performed orthodontic extrusion for the same (Fig. 3).18% of the 250 participants had given splinted crowns as a measure of combating cementation failure in case of short crowns.Moving on to the occlusal adjustments done on the grounds of its management, 20% reported to having relieved prematurities and 74% had stated to have relieved them out of occlusion (Fig. 4).84% of the surveyed participants had instructed the patients to avoid sticky foods to prevent future dislodgements.8% of the practicing dentists had tried sand blasting the intaglio surface of the crowns as an aid to enhance retention.While 67% of them had tried post and core restorations to manage the same (Fig. 5).34% of the dentists surveyed had admitted to preferring placement of a subgingival margin for management of short clinical crowns.
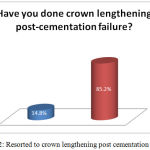 |
Figure 2: Resorted to crown lengthening post cementation failure. |
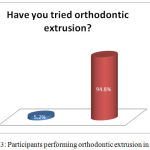 |
Figure 3: Participants performing orthodontic extrusion in practice. |
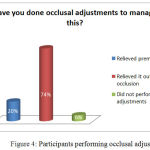 |
Figure 4: Participants performing occlusal adjustments. |
 |
Figure 5: Participants performingpost and core. |
Discussion
With various remedial measures attributed to management of short clinical crowns in the literature, it is essential for the clinician to have a sound knowledge on all aspects involved.14,15 Various tooth preparation modifications have been done to manage dislodgement of crowns in abutment teeth with reduced clinical height. Common modifications that could be done include incorporation of interproximal grooves with 1mm width and depth in the gingival base was found to be a contributory factor in improving the retention of crown in compromised conditions.16,17 Reduction of total occlusal convergence at the cervical level is known to show better effects in terms of retention as compared to proximal grooves. Other modifications include buccal grooves and proximal boxes. In our study, 64% added grooves on either side, 24% added grooves on both sides and 12% prepared proximal boxes. Awareness on this aspect still being questionable, performance of studies in this aspect is essential to evaluate the superiority of one modification over the other.
Crown lengthening being one of the most preferred methods in management of short clinical crowns, has its own pitfalls when compared to other methods.18-25 When compared to orthodontic extrusion, crown lengthening shows deleterious effects by hampering the biological width. Crown lengthening has two variants: one being only gingivoplasty and the other being gingivoplasty in combination with osteoplasty. With presence of appropriate osseous levels, soft tissue greater than 3mm from bone to gingival crest and on determination that an adequate zone of attached gingiva will remain even after surgery, gingivoplasty may be performed.26 When the diagnostic procedures reveal osseous levels close to the CEJ, a gingival flap with osteoplasty followed by gingivoplasty or apical repositioning of flap before closure may be performed. In our study, 15% of the survey population having admitted to performing crown lengthening and 9% has admitted to having done osteoplasty along with gingivoplasty to manage short clinical crowns.
During the process of devesting and finishing of cast metal crowns, the intaglio surface is sand blasted or electro etched to remove impurities and bring about an increase in the level of retention.27,28 Electroetching of nonprecious alloys promotes bonding of composites to metals. It has been successfully used for resin-bonded retainers.29,30 Occlusal adjustments as a way to combat fatigue failure in prosthesis had been known in the dental literature.31 Though relieving the restoration completely out of occlusion is a known aspect in implant therapy, it being a remedial measure is the scenario of failed full coverage restorations in shortened clinical crowns is an aspect that is yet to be explored.
Placement of sub gingival margins is yet another modality that has been used in management of short clinical crowns.32 However, it is not widely preferred owing to increased plaque retention and accelerated periodontal break down although improved esthetics may be observed.33-35 And with time, the gingiva starts receding resulting in an unaesthetic display of the margin. In our study, 34% of the population has admitted to having taken up placement of subgingival margins as a remedial measure. Awareness on the detrimental effects of placement of subgingival margins and the weightage of their pros over cons need to be performed in order to validate this modality an effective remedial measure.Orthodontic extrusion being a remedial measure in management of short clinical crowns has its application in clinical practice based on various factors.36,37 In orthodontic patients with missing teeth, extrusion of short clinical crowns may be a promising option. In non-orthodontic cases, though orthodontic extrusion might be friendly to the supporting structures and not hamper the biological width as seen in crown lengthening or placement of sub gingival margins; it has its own factors of consideration such as bracket placement, forces applied, compromise in crown root ratio and time required for the procedure to take place.38,39 Though it has better effects in the periodontal aspect, time constraint is a big factor which affects the feasibility and acceptance in patient level. In our study, 5% survey population has admitted to having used orthodontic extrusion in the management of short clinical crowns.
The amount of desired forced eruption must be determined beforehand because landmarks change during the eruptive process. It should be achieved at a rate of 1 mm every 1 to 2 weeks. After forced eruption is accomplished, the tooth of interest should be placed in retention for a period of 2 to 3 months to allow the bone and soft tissue to move with the tooth. In cases where esthetic correction is required by crown lengthening, the biologic width is hampered and the interdental bone is involved, osseous correction is preferred. In such cases, teeth that have undergone forced eruption should be placed in retention post operatively over a span of 3 – 6 months before final restoration is placed.The final remedial measure appraised in this study is post and core restoration to manage short clinical crowns. Factors such as training and practice in post and core use, materials employed and their effect on the structural and functional components may also be considered before resorting to this measure.40 In our study about 67% of the survey population had used post and core in the clinical scenario of our interest.
Conclusion
The knowledge and awareness level elicited in this questionnaire study is moderate. Though there is a moderate level of knowledge and awareness present, the level applied in practice is poor, the reason being lack of training and incomplete understanding on this grounds. Hence more awareness programs and hands-on clinical training needs to be conducted to address this.
References
- Seol H. W., Koak J. Y., Kim S. K., Heo S. J. Full mouth rehabilitation of partially and fully edentulous patient with crown lengthening procedure: a case report. J Adv Prosthodont. 2010 1;2(2):50-3.
- Smith B. G. Dental crowns and bridges: design and preparation. Year Book Medical Publishers. 1986.
- Chu S. J., Karabin S., Mistry S. Short tooth syndrome: diagnosis, etiology, and treatment management. J Calif Dent Assoc. 2004;32(2):143-52.
- Davarpanah M., Jansen C. E., Vidjak F., Etienne D., Kebir M., Martinez H. Restorative and periodontal considerations of short clinical crowns. Int J Periodontics Restorative Dent. 1998 1;18(5).
- Johansson A., Omar R., Carlsson G. E. Bruxism and prosthetic treatment a critical review. J Prosthodont Res. 2011;55(3):127-36.
CrossRef - Tomar N., Bansal T., Bhandari M., Sharma A. The perio-esthetic-restorative approach for anterior rehabilitation. J Indian Soc Periodontol. 2013;17(4):535.
CrossRef - Turner K. A., Missirlian D. M. Restoration of the extremely worn dentition. J Prosthet Dent. 1984;52(4):467-74.
CrossRef - Brown K. E. Reconstruction considerations for severe dental attrition. J Prosthet Dent. 1980;44(4):384-8.
CrossRef - El-Mowafy O. M., Fenton A. H., Forrester N., Milenkovic M. Retention of metal ceramic crowns cemented with resin cements: effects of preparation taper and height. J Prosthet Dent. 1996;76(5):524-9.
CrossRef - Walton J. N., Gardner F. M., Agar J. R. A survey of crown and fixed partial denture failures length of service and reasons for replacement. J Prosthet Dent. 1986;56(4):416-21.
CrossRef - Assif D., Pilo R., Marshak B. Restoring teeth following crown lengthening procedures. J Prosthet Dent. 1991;65(1):62-4.
CrossRef - Smukler H., Chaibi M. Periodontal and dental considerations in clinical crown extension a rational basis for treatment. Int J Periodontics Restorative Dent. 1997;17(5).
- Kalaivani S., Manohar J., Shakunthala P., Sujatha S., Rajasekaran S. A., Karthikeyan B,. Kalaiselvan S. Crown lengthening procedure in the management of amelogenesis imperfecta. J Pharm Bioallied Sci. 2015;7(Suppl 2):S769.
- Gupta G., Gupta R., Gupta N., Gupta U. Crown Lengthening Procedures-A Review Article. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS). 1(14):27-37.
- Hempton T. J., Dominici J. T. Contemporary crown-lengthening therapy: a review. J Am Dent Assoc. 2010;141(6):647-55.
CrossRef - Roudsari R. V., Satterthwaite J. D. The influence of auxiliary features on the resistance form of short molars prepared for complete cast crowns. J Prosthet Dent. 2011;106(5):305-9.
CrossRef - Proussaefs P., Campagni W., Bernal G., Goodacre C., Kim J. The effectiveness of auxiliary features on a tooth preparation with inadequate resistance form. J Prosthet Dent. 2004;91(1):33-41.
CrossRef - Planciunas L., Puriene A., Mackeviciene G. Surgical lengthening of the clinical tooth crown. Stomatologija. 2006;8(3):88-95.
- Talbot T. R., Briggs P. F., Gibson M. T. Crown lengthening-a clinical review. Dent Update. 1993;20:301-3.
- Baima R. F. Extension of clinical crown length. J Prosthet Dent. 1986 May 1;55(5):547-51.
CrossRef - Dibart S., Capri D., Kachouh I., Dyke T. V., Nunn M. E. Crown lengthening in mandibular molars: a 5-year retrospective radiographic analysis. J Periodontol. 2003;74(6):815-21.
CrossRef - Jorgensen M. G., Nowzari H. Aesthetic crown lengthening. 2000. 2001;27(1):45-58.
- Lanning S. K., Waldrop T. C., Gunsolley J. C., Maynard J. G. Surgical crown lengthening: evaluation of the biological width. J Periodontol. 2003;74(4):468-74.
CrossRef - Nethravathy R., Vinoth S. K., Thomas A. V. Three different surgical techniques of crown lengthening: A comparative study. J Pharm Bioallied Sci. 2013;5(5):14.
CrossRef - Palomo F., Kopczyk R. A. Rationale and methods for crown lengthening. J Am Dent Assoc. 1978;96(2):257-60.
CrossRef - Dolt A. H., Robbins J. W. Altered passive eruption: an etiology of short clinical crowns. Quintessence Int. 1997;28:363-74.
- O’Connor R. P., Nayyar A., Kovarik R. E. Effect of internal microblasting on retention of cemented cast crowns. J Prosthet Dent. 1990;64(5):557-62.
CrossRef - Shahin R., Kern M. Effect of air-abrasion on the retention of zirconia ceramic crowns luted with different cements before and after artificial aging. Dent Mater. 2010;26(9):922-8.
CrossRef - Chan K. C., Boyer D. B., Denehy G. E., Aunan D. C. Effect of metal etching on crown retention. J Prosthet Dent. 1986;55(1):18-21.
CrossRef - Livaditis G. J., Thompson V. P. Etched castings: an improved retentive mechanism for resin-bonded retainers. J Prosthet Dent. 1982;47(1):52-8.
CrossRef - Torbjörner A., Fransson B. Biomechanical aspects of prosthetic treatment of structurally compromised teeth. Int J Prosthodont. 2004;17(2).
- Newcomb G. M. The relationship between the location of subgingival crown margins and gingival inflammation. J Periodontol. 1974;45(3):151-4.
CrossRef - Wilson RD, Maynard G. Intracrevicular restorative dentistry. Int J Periodontics Restorative Dent. 1980;1(4):34-49.
- Maynard Jr J. G., Wilson R. D. Physiologic dimensions of the periodontium significant to the restorative dentist. J Periodontol. 1979;50(4):170-4.
CrossRef - Sharma A., Rahul G. R., Poduval S. T., Shetty K. Short clinical crowns (SCC)–treatment considerations and techniques. J Clin Exp Dent. 2012;4(4):e230.
CrossRef - Johnson G. K., Sivers J. E. Forced eruption in crown-lengthening procedures. J Prosthet Dent. 1986;56(4):424-7.
CrossRef - Shiloah J. Clinical crown lengthening by vertical root movement. J Prosthet Dent. 1981;45(6):602-5.
CrossRef - Stern N., Becker A. Forced eruption: biological and clinical considerations. J Oral Rehabil. 1980;7(5):395-402.
CrossRef - Maglad A. S., Wassell R. W., Barclay S. C., Walls A. W. Risk management in clinical practice. Part 3. Crowns and bridges. Br Dent J. 2010;209(3):115-22.
CrossRef - Akbar I. Knowledge attitudes and practice of restoring endodontically treated teeth by dentists in north of Saudi Arabia.Int J Health Sci (Qassim). 2015;9(1):41.
CrossRef

