
Arta Eka Putra, Lely Rahayu and Edward Limantara
Department of Otorhinolaryngology, Medical Faculty of Udayana University, Sanglah Hospital, Denpasar, Indonesia.
Corresponding Author E-mail: aep.tht@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1191
Abstract
In children, adenoid and tonsil infection tends to reccurent and chronic infection in both lymphoid tissue leads into oxygenation obstruction in airway, especially in sleep, that resulted in altered quality of life in children. Breathing disorder in sleep, obviously in children, will affect their routines in daytime including studying, learning, and attention deficit disorder. This research is a pre-experimental study with one group pre-post test design (before-after study). In this study, we have one group of children undergoing adenotonsillectomy. Then we will assess the quality of life by using PedsQL before adenotonsillectomy and after adenotonsillectomy, and then we will compare the PedsQL score between before and after adenotonsillectomy. In this study, we can obtain an improvement of physic activity function, feeling or emotion function (mental), sociality function, child function in school, and significant quality of life based on PedsQL score in children with chronic adenotonsilitis after underwent adenotonsillectomy operation.
Keywords
Adenotonsillectomy; PEDS-QL; children; RSUD Badung
Download this article as:| Copy the following to cite this article: Putra A. E, Rahayu L, Limantara E. Differences in Pediatrics Quality of Life (Peds-Ql) Test in Children Before and After Adenotonsillectomy in 2016. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Putra A. E, Rahayu L, Limantara E. Differences in Pediatrics Quality of Life (Peds-Ql) Test in Children Before and After Adenotonsillectomy in 2016. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=15392 |
Introduction
Upper respiratory tract infection is one of the most common diseases in primary care centers and specifically in the Ear Throat Ears (ENT), infection in adenoids and tonsils are also one of the most common diseases. In children, adenoid and tonsils infections remain recurrent and chronic infection in both lymphoid tissue can cause oxygenation obstruction in respiratory tract, especially during sleep that will ultimately affect the quality of life in children. Sleep disordered breathing is commonly found in 11-40% of the children population, especially those with chronic adenotonsillitis. Sleeping breathing disorders in children will affect routine activities during the daytime including playing, studying, and attention distraction.1
Bhatt et al. (2014) mentioned that chronic adenotonsilitis in children also cause sleep disorder (sleep disordered breathing) which result in decreasing quality of sleep. Decreased of muscle tone in sleeping can cause the airway to become narrower and when accompanied by chronic adenotonsilitis, it will increase an airflow resistance and cause severe breathing work. 2
Ilias et al. (2012) conducted a quality of life research in 79 children under the age of 15 with chronic adenotonsilitis.3 They obtained a conclusions of decreased quality of life during activity, sleep diordered breathing, increased number of visits to the doctor, decreased of concentration in school and frequent absences. Children with chronic adenotonsilitis tend to have lower quality of life that affects health status, daily physical activity, playing and learning activity when compared with children without chronic adenotonsillitis.4
Adenotonsillectomy (ATE) is considered effective because it can reduce the rate of recurrence of throat infection in children.5 Another consideration of adenotonsillectomy is the provision of antibiotic therapy that is less successful against recurrence of chronic adenotonsilitis.6
In the United States, each year more than 500,000 ATE procedures are performed and is the third most surgical procedure done after circumcision and ear tube installation. Europan statistics noted that by 2013, in Germany and Finland, 170 ATE operations are performed per 100,000 population. New Zealand’s health quality and safety supervisory agency in 2010-2015 noted that ATE procedure has been done by 4 per 1000 children. In Indonesia there is still no official data on the number of ATE procedur, only mentioning about the prevalence of chronic tonsillitis in Indonesia, especially in 7 provinces during 1994-1996, was 3.8%.7 Based on the Household Health Survey in 1995, chronic adenotonsilitis was ranked five among the common diseases found in children and occured at most in the age of 5 to 14 years.7 At RSCM Jakarta in 1999-2003, 427 procedure of ATE8 were obtained.
The quality of life assessment is an assessment that encompasses broad physical and psychological characteristics that describe a person’s ability to play a role in his environment and gain satisfaction from what he does. The quality of life assessment is influenced by the physical, mental, social and emotional state. This assessment can be done using quality of life instrument, such as the pediatrics quality of life (PedsQL).9 The importance of assessing the quality of life in pediatric patients with chronic adenotonsilitis is to determine the improvement of quality of life gained between before and after ATE procedure. Ramin et al. (2014) suggests that ATE in children with chronic adenotonsillitis is expected to improve quality of life, especially improvements in sleep quality.10 Most ATE measurement (79%) are aimed at improving the quality of life of children, especially sleep quality and improving the quality of physical activity by decreasing recurrence.11 Goldstein et al. (2008) reported in his study of 92 children who had performed adenotonsillectomy,12 there was a significant improvement in the quality of life in daily physical activity, a decrease in the number of visits to doctors or health services due to a decrease in recurrence rate. Alcantara et al. (2008) also reported significant improvements in quality of life after ATE,13 especially in sleep quality as many as 62%, improvements in learning ability and school attendance were 75% and 76%. Patient parents satisfaction after their children underwent ATE is quite high, namely 75%, as the feel that their children has been significantly improved.13
Research about improvement in children quality of life before and after the ATE has been done in overseas, but in Indonesia, especially in Bali province has not been done so that researchers are interested to know the improvement of quality of life before and after doing ATE procedure.
Method
Study Design
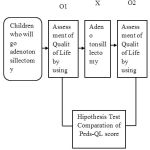
This research will be a pre-experimental study with pre-post test design (before-after study). The reason for choosing the design is that this study has one group of children who will undergo adenotonsillectomy. Then a quality of life evaluation was performed by using PedsQL before adenotonsillectomy and after adenotonsillectomy and then we compared the PedsQL score between before and after adenotonsillectomy. The design of this research can be made as scheme, just as follows:
 |
Graph 1
|
Explanation
O1 : pre test in group before undergo an intervention
X : Treatment in intervention group compatible with the protocol
O2 : post test in group after underwent an intervention
Study Sample
Prospective study will conducted in THT-KL policlinic RSUD District Badung Mangusada, from June 1st until August 15th , 2016. Each children with age of 5 until 12 years old, appropriate with inclusion criteria, that come into THT-KL Policlinic RSUD District Badung Mangusada, and will be done adenotonsillectomy drom June 1st until August 15th, 2016, will included to be subject in this research, until minimal number has been fulfilled. Election way of the sample will be done by using consecutive sampling method
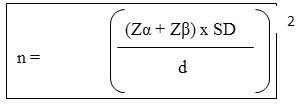
Number of samples will be calculated by using formula:
Explanation
n : number of samples
SD : Standard deviation from the mean of difference = 10 (Goldstein dkk., 2008; Ericson dkk., 2009)
Zα : type I error, α: 0,05 so Zα=1,96
Zβ : type II error, β: 80% so Zβ=0,842
D : Mean difference between the two clinically important groups (clinical judgement) = 5 (Ericson dkk., 2009)
n = [(1,96 + 0,842) x 10 / 5]2
n = [2,802 x 10 / 5]2
n = 31,404 samples à rounded up to 32 samples
So, for this study, we need 32 samples of children that will undergo adenotonsillectomy procedure
Data Collection
Children population in age of 5 until 12 years old with chronic adenotonsilitis that fulfill inclusion criteria will be choose as a sample. Then, we asked them to fill the PedsQL questionnaire before undergo adenotonsillectomy procedure and 30 days after adenostonsillectomy
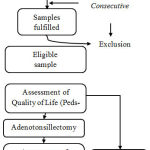 |
Graph 2 Click here to View graph |
Data analysis in this research consisted of descriptive statistical analysis and comparison analysis of paired sample mean. Descriptive statistical analysis aims to describe the characteristics of research subjects and research variables. Scaled numerical data variables are displayed in the mean and standard deviation. Categorical data-scale variables are displayed by using numbers and percentages. By knowing the characteristics of research subjects then it can be assessed later on the representation of the population.
Mean comparison analysis is for paired samples. To perform this analysis, firstly, we tested the normality of the study. Normality test aims to determine whether the data distribution from the quality of life scores have normal distribution or not. To perform the normality test, we used the normality test from Saphiro-Wilk. It is called normal distribution if the p value of the normality test of Saphiro-Wilk > 0.05. If the distribution of data on the two quality of life measurements before and after are normal distribution, the test used will be paired t-test at the 0.05 significance margin and if the data distribution of one measurement or both does not normally distributed then we used non parametric test from Wilcoxon.
The whole process of data analysis above is done by using the help of SPSS 20.0 software.
Research Result
This research was conducted at RSUD District Badung Mangusada. This study is an experimental pre-post test design (before-after study) in which the subjects were patients aged 5-12 years who suffered from chronic adenotonsillitis and underwent adenotonsillectomy. Then a quality of life evaluation was performed by using PedsQL before adenotonsillectomy and 30 days after adenotonsillectomy and then we compared the PedsQL score between before and after adenotonsillectomy. Through the sample calculation formula, obtained the number of samples as much as 32 people and the selection of samples we performed a consecutive sampling.
Characteristics of Research Subjects
Characteristics of research subjects observed included gender, age, adenoid hypertrophy (assessed by looking at the AN-ratio, equal to or greater than 0.73) and the degree of enlarged tonsils. Of the 32 research subjects obtained 20 boy children and 12 girl children. Subject characteristics by gender, age group, AN-ratio and degree of tonsil enlargement can be seen in Table 1.
Table 1: Characteristic of research sample based on gender, age group, AN-ratio, and degree of tonsil enlargement
| Characteristic | n = 32 |
| Gender
Boy Girl |
20 (62,5%) 12 (37,5%) |
| Age (years old)
Mean ± SD Minimal – maximal |
8,5 ± 1,9 5 – 12 |
| AN-ratio
Median (Inter Quartil Range/IQR) |
0,75 (0,037) |
| Degree of tonsil enlargement
T2 T3 T4 |
13 (40,6%) 16 (50%) 3 (9,4%) |
Based on the characteristics of research subjects such as gender, age, AN-ratio value and the degree of tonsils enlargement in 32 selected children as the subjects of the study then obtained boy childred as much as 20 patients or 62.5% and the girl children as many as 12 patient or 37.5% and the mean age was 8.5 years with an SD score of ± 1.9, the youngest age of pediatric patients who were the subject of the study was 5 years and the oldest age was 12 years. The median AN-ratio obtained from 32 subjects of this study was 0.75 where the inter quartile range (IQR) value was 0.037 and based on the degree of tonsil enlargement from 32 subjects it was obtained that T2 enlargement was 13 or 40.6%, enlargement of T3 tonsils was 16 or 50.0% and T4 degrees was 3 or 9.4%.
Improved Physical Activity Function After Adenotonsillectomy Based on Pedsql
The improvement of physical activity function after ATE based on PedsQL can be seen in Table 2. In the physical activity function before ATE procedure, the median value was 90.6 with inter quartil range (IQR) of 11,7 and after ATE we obtained the score of 90.6 with inter quartile range IQR) of 6.25 where p value < 0.001. The difference of median and IQR values on physical activity function between before and after ATE can be seen in Figure 1.
Table 2: Improvement in physical activity function after adenotonsillectomy based on PedsQL
| Quality of Life | Physical Activity | ||
| Median (IQR) | Adenotonsilectomy | Before | 90,6 (11,7) |
| After | 90,6 (6,25) | ||
| Minimal Maximal | Adenotonsilectomy | Before | 62,5 (100) |
| After | 68,75 (100) | ||
| P value | <0,001 | ||
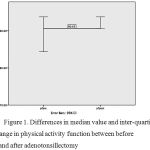 |
Figure 1: Differences in median value and inter-quartile range in physical activity function between before and after adenotonsillectomy Click here to View figure |
Improvement in Feeling/Emotion Function After Adenotonsillectomy Based on Pedsql
Improvement in feeling/emotional function after adenotonsillectomy based on PedsQL can be viewed in Table 3. Feeling/emotional function before adenotonsillectomy procedure, we obtained median value as 90,0 with inter-quartil range (IQR) as 10 and after underwent adenotonsillectomy, reported a median value as 95,0 with inter-quartil range (IQR) as many as , wehre p value < 0,001. Differences in median value and IQR in feeling/emotional function between before and after adenotonsillectomy can be seen in Figure 2.
Table 3: Improvement of feeling/emotional function after adenotonsillectomy based on PedsQL
| Quality of Life | Feeling/Emotion | ||
| Median (IQR) | Adenotonsilectomy | Before | 90,0 (10) |
| After | 95 (5) | ||
| Minimal Maximal | Adenotonsilectomy | Before | 75,8 (100) |
| After | 85 (100) | ||
| P value | <0,001 | ||
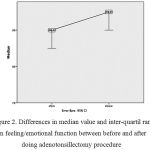 |
Figure 2: Differences in median value and inter-quartil range in feeling/emotional function between before and after doing adenotonsillectomy procedure Click here to View figure |
Improvement of Socialization Function After Adenotonsillectomy Based on Pedsql
Improvemnet of socialization function after underwent adenotonsillectomy based on PedsQL is listed in Table 4. In socialization function before adenotonsillectomy procedure, we obtained a median value as 90,0 with inter-quartil range (IQR) as many as 5 and after adenotonsillectomy, we can obtain median value as 90,0 with inter-quartil range (IQR) of 9, where p value < 0,001. Differences in median value and IQR of socialization function before and after adenotonsillectomy can be seen in Figure 3.
Table 4: Improvement of socialization function after adenotonsillectomy based on PedsQL
| Quality of Life | Socialization | ||
| Median (IQR) | Adenotonsilectomy | Before | 90,0 (5) |
| After | 90,0 (9) | ||
| Minimal Maximal | Adenotonsilectomy | Before | 65,00 (95,00) |
| After | 70,00 (95,00) | ||
| P value | <0,001 | ||
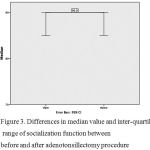 |
Figure 3: Differences in median value and inter-quartil range of socialization function between before and after adenotonsillectomy procedure Click here to View figure |
Improvement of Children Function at School After Adenotonsillectomy Based on Pedsql
Improvement of children function at school after adenotonsillectomy based on PedsQL is listed in Table 5. In children function at school before adenotonsillectomy, we obtained median value as 75,0 with inter-quartil range (IQR) as 15 and after adenotonsillectomy procedure, median value was 80,0 with inter-quartil range (IQR) 9, where p value < 0,001. Differences in median value and IQR of children function at school between before and after adenotonsillectomy can be seen in Figure 4.
Table 5: ‘Improvement of children function at school after adenotonsillectomy absed on PedsQL
| Quality of Life | At School | ||
| Median (IQR) | Adenotonsilectomy | Before | 75 (15) |
| After | 80 (9) | ||
| Minimal Maximal | Adenotonsilectomy | Before | 50 (90) |
| After | 60 (90) | ||
| P value | =0,005 | ||
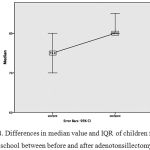 |
Figure 4: Differences in median value and IQR of children function at school between before and after adenotonsillectomy Click here to View figure |
Improvement of Children Quality of Life from overall Score in Pedsql Between Before and After Adenotonsillectomy
Improvement of children overall quality of life after adenotonsillectomy based on PedsQL can be seen in Table 6. Overall score of PedsQL before adenotonsillectomy was 85,6 with inter-quartil range (IQR) of 5,6 and after adenotonsillectomy, we obtained the score was 88,4 with inter-quartil range (IQR) of 4,7, where p value < 0,001. Differences in median value and inter-quartil range (IQR) in overall score PedsQL between before and after adenotonsillectomy can be seen in Figure 5.
Table 6: Improvement of children overall quality of life between before and after adenotonsillectomy based on PedsQL
| Quality of Life | Total Score of PedsQL | ||
| Median (IQR) | Adenotonsilectomy | Before | 85,6 (5,6) |
| After | 88,4 (4,7) | ||
| Minimal Maximal | Adenotonsilectomy | Before | 66,88 (92,97) |
| After | 77,81 (92,97) | ||
| P value | <0,001 | ||
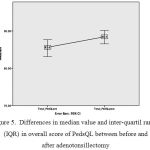 |
Figure 5: Differences in median value and inter-quartil range (IQR) in overall score of PedsQL between before and after adenotonsillectomy
|
Discussion
This research is a pre-experimental study with one group pre-post test design (before-after study). This retrospective study was conducted in THT-KL policlinic RSUD District Badung Mangusada with target population of children patient who will be done adenotonsillectomy with the age of 5-12 years old. Ramya et al (2016) reported that in 100 children who went into adenotonsillectomy procedure had a majority age research subject (65%), in group of 5-10 years old.14 In this study, we found a ratio of boy children vs girl children, namely 1,6 : 1,0. Many literatures did not say about the relationship between gender and incidence of chronic adenotonsillitis.
Naiboglu and colleague (2010), in their study of 40 children who underwent ATE procedure, then assessed the quality of life by using PedsQL, they reported any improvement in physical activity function, which is score of PedsQL before ATE procedure was 64,81, then after the patient had been done the ATE procedure, the score was significantly increased, into 83,67. So that, they obtained an improvementacore by 18,86.15 In this study, we found a median value of PedsQL in physical activity function before ATE was 90,6 and after ATE procedure, the score remained 90,6. Eventhough median value in before and after ATE was still the same, but the inter-quartil range (IQR) score was shortened, from 11,7 into 6,25. Even after that, we can state that there was an improvement statistically.
Chronic adenotonsilitis that commonly found in children is one of the risk factors associated with sleep disordered breathing (SDB). Kaditis et al. (2015) stated that SDB is a syndrome of upper respiratory tract dysfunction that occurs at the time of sleep one of which is marked by sound snoring.16 Kaditis et al (2015) also mentioned that the presence of adenoid and tonsil hypertrophy contributed to SDB incidence but was not the sole determinant factor in the degree of severity of airway obstruction.16 In children, SDB is associated with behavioral disorders.17,18 Gupta et al. (2013) in his study of 131 children undergoing ATE treatment and then observed for 2 years after ATE procedure, they assessed the improvement of emotional / feeling function and concluded 50% of respondents stated no change in feeling / emotional function and 30% respondents stated that they got improvement on emotion / feeling function.19 In this study, the median value of PedsQL in feeling / emotional function before ATE procedure was 90.0 and 30 days after ATE with median value was 95.0. Similarly, the value of inter quartile range (IQR) before ATE, 10 and 5 after ATE. So it can be concluded that the ATE procedure is able to provide improvements to the feelings / emotions based on PedsQL.
Naiboglu et al. (2010) in his study of the quality of life in children with chronic adenotonsilitis using PedsQL questionnaire scored in the socialization function of pre ATE was 76.37 and obtained an increased into 85.75, marked an improvement after ATE.15 Although the study found no improvement in the socialization function, the median value before ATE and after ATE was 90, for each; and inter quartile range from before ATE was 5 to 9 after ATE. Where the minimal-maximal score range before ATE is 65-95 then the range narrowed into 70-95 after ATE.
Barraclough & Anari (2014) in his meta-analysis study reported a study using PedsQL instruments after ATE, they found an improvement of quality of life in children function at school, especially in the number of attendance as it improved because the decreased of recurrence rate.20 In this study there was also a significant improvement in the children function at school, namely from the median value of 75 before ATE into 80 after ATE and inter quartil range (IQR) that narrowed from 15 before ATE to 9 after ATE. Where the minimum-maximum score range before ATE is 50-90 then the range narrowed into 60-90after ATE.
ATE procedure in pediatric patients with chronic adenotonsilitis in overall can improve the quality of life of children, this can be seen from various studies of the children’s quality of life.10,12,13,14,21 This proves an improvement in quality of life based on PedsQL score of 2.8%, which was observed 30 days after the ATE procedure. So it can be said that with the ATE procedure in chronic adenotonsillitis could give an improvement in children’s quality of life.
Conclusion
From this research, we can obtain an improvement of physical activity function, feeling or emotional function, children function at school, and significant quality of life based on PedsQL score in children with chronic adenotonsillitis after underwent adenotonsillectomy procedure.
References
- Jeon, Y.J., Song, J.J., Ahn, J.C., Kong, G.I. 2016. Immidiate and sustained improvement in behavior and life quality by adenotonsillectomy in children with sleep disordered breathing. Clinical experimental otorhinolaryngology. 9(2):136-142.
CrossRef - Bhatt, S.P., Guleria, R., Kabra, S.K. 2014. Obstructive Sleep Apnea Syndrome in Children. International Journal of Medicine and Medical Sciences. 1(2):14-20.
- Ilias, K., Nekatarios, A., Argyrios, M. 2012. Parental expectations after tonsillectomy focused on disease-specific quality of life utilizing a modified PedsQL questionnaire. Greece Otorhinolaryngologia – Head and Neck Surgery. 50:12-16.
- Wayne, J.B., Dan, K., Webb, C.K, Giultoni, K. 2014. Select Health of South Carolina: Clinical Guideline Tonsillectomy and/ or Adenoidectomy. South Carolina: 1-17.
- Burton, M.J., Glazziou, P.P., Chong, L.Y., Venekamp, R.P. 2014. Tonsillectomy or adenotonsillectomy versus non-surgical treatment for chronic/recurrent acute tonsillitis. Cochrane Database of Systematic Reviews2014, Issue 11. Art. No.: CD001802. DOI: 10.1002/14651858.CD001802.pub3.
CrossRef - Ghiyasi, S.J.E, Naderpour, M., Raouf, F., Sabermarouf, B. Adenotonsillectomy and its Effect on the Quality of Life in Adult Patients. Advances in Bioscience and Clinical Medicine Journal. 2(2):77-82.
- Sakka, I.,Sedjawidada, R., Kodrat, L., Rahardjo, S.P. Kadar imunoglobulin A sekretori pada penderita tonsilitis kronik sebelum dan setelah tonsilektomi. Jurnal ORLI Oto Rhino Laryngologica Indonesiana. 41(3):1-5.
- Hermani, B. 2004. Health Technology Indonesia 2004: Tonsilektomi pada Anak dan Dewasa. Unit Pengkajian Teknologi Kesehatan Direktorat Jenderal Pelayanan Medik Departemen Kesehatan RI. HTA Indonesia 05/2004/x.
- Nilsson, E. 2012. “Aspects of Health-related Quality of Life Associations with psychosocial and biological factors, and use as patient-reported outcome in routine health care” [Dissertations]. Linkoping University, Sweden.
- Ramin, Z., Mirzadeh, M., Farsi, M.M, et al. 2014. The Effect of Adenotonsillectomy on Children’s Quality of Life. Iranian Journal of Otorhinolaryngology. 26(4): 199-205.
- Wong BYH, Ng YW, Hui Y. 2007. A 10 year Review of Tonsillectomy in a Tertiary Care. HK J Pediatr Journal. 12:297-99.
- Goldstein, N.A., Stewart, M.G, Witsell, D.L, Hannley, M.T., Weaver, E.M. 2008. Quality of Life After Tonsillectomy in Children With Recurrent Tonsillitis. Journal Otolaryngology-Head and Neck Surgery. 138:S9-16.
CrossRef - Alcantara, L.J., Pereira, R.G., Mira, J.G., Soccol, A.T., Tholken, R. 2008. Adenotonsillectomy Impact on Children’s Quality of Life. Brazil Int. Archives of Otorhinolaryngology. 12(2):172-78.
- Ramya, B., Viswanatha, B., Siddappa, M., Mohan, A. 2016. Quality of life post adenotonsillectomy in children with adenotonsillar hypertrophy: a prospective study. Research in Otolaryngology. 5(2):32-38.
- Naiboglu, B., Kuleckci, S., Kalaycik, C., Sheidaei, S., Toroz, S.Z., Egeli, E. 2010. Improvement in Quality of Life by Adenotonsillectomy in Children with Adenotonsillar Disease. Clin. Otolaryngol 35:383-89.
CrossRef - Kaditis, A.G., Alvarez, M.L., Boudewyns, A., Alexopoulus, E.I. 2015. Obstructive sleep disordered breathing in 2-18 years-old children: diagnosis and management. ERJ express.doi: 10.1183/13993003.00385-2015.
CrossRef - Jeyakumar, A., Miler, S., Mitchell, R.R. 2014. Adenotonsillar Disease in Children. In: Johnson, J.T., Rosen, C.A., editors. Bailey’s Head and Neck Surgery Otolaryngology. 5th. Ed. Philadelphia: Lippincott Williams and Wilkins. p.1430-1444.
- Stewart, M.G., Sulek, F.M., Hulka, G.F., Kuppersmith, R.B. 2000. Quality of life and health status in pediatric tonsil and adenoid disease. Arch Otolaryngol Head Neck Surg. 126(2000):45-48.
CrossRef - Gupta N, Vaid L, Singh PP. 2013. Impact of Tonsillectomy on Quality of Life in Chidren: Our Experience. Indian Journal of Clinical Practice. 24(6): 543-46.
- Barraclough, J and Anari, S. 2014. Tonsillectomy for recurrent sore throats in children: indications, outcomes and efficacy. Otolaryngology-Head and Neck Surgery. 150(5):722-29.
CrossRef - Garetz, S.L and Arbor, A. 2014. Quality of Life and Obstructive Sleep Apnea Symptoms After Pediatric Adenotonsillectomy. American Academy of Pediatrics Journal. 135(2):477-86.

