
Moshiri E1, Malekianzadeh B1, Modir H1 and Damanpak moghadam V2
1Department of Anesthesiology and Critical Care, Arak University of Medical Sciences, Arak, Iran.
2Resident of Anesthesiology, Arak University of Medical Sciences, Arak, Iran.
Corresponding Author E-mail: he_modir@arakmu.ac.ir
DOI : https://dx.doi.org/10.13005/bpj/1149
Abstract
Hemodynamic complications of regional anesthesia in patients with severe preeclampsia, has been faced challenges using of this approach.one way to overcome this problem is decreasing dosage of anesthetic drugs but this situation, can result in pain during surgery. The aim of our study is comparing spinal anesthesia with low and conventional doses of Bupivacaine on hemodynamic parameters in patient with severe preeclampsia whom underwent cesarean section.60 patients with severe preeclampsia who underwent cesarean delivery included in this clinical trial study randomly. Spinal anesthesia was done with injection of 7.5 and 12 mg Bupivacaine in two groups. Mean of blood pressure and heart rate were recorded at the beginning of induction and then during each 5 min until end of surgery. Data were compared with t test and repeated measure. Mean of hemodynamic parameters were significantly decreased during surgery in both groups but between groups we have hadn’t significant differences. Low dose of bupivacaine is suitable for cesarean section. however incidence of hemodynamic change hadn't significant difference versus conventional dose.
Keywords
Cesarean section; Hemodynamic; sever preeclampsia; spinal anesthesia
Download this article as:| Copy the following to cite this article: Moshiri E, Malekianzadeh B, Modir H, Moghadam V. D. Comparison of Spinal Anesthesia With Low and Conventional Doses of Bupivacaine on Hemodynamic Changes in Severe Preeclampsic Patients Candidate for Cesarean Section. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Moshiri E, Malekianzadeh B, Modir H, Moghadam V. D. Comparison of Spinal Anesthesia With Low and Conventional Doses of Bupivacaine on Hemodynamic Changes in Severe Preeclampsic Patients Candidate for Cesarean Section. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=15239 |
Introduction
The preferred method of delivery is the Caesarean section in patients with severe preeclampsia. Pathophysiological changes made in this patient makes the choice of anesthesia, challenging. If you use general anesthesia for these patients you are facing the risk of severely elevated blood pressure and increased risk of airway edema and difficult tracheal intubation. And these effects make using this method increase morbidity and mortality (1-3). In regional anesthesia, epidural and spinal anesthesia can be used for cesarean section. Spinal anesthesia with respect to the lack of need to insert the catheter can be used in emergency situations quickly and easily it also has relatively low cost and few side effects (4).But the major drawback of this method that makes us use with more caution is the severe reduction of blood pressure. On the one hand on the patient due to an underlying dysfunction in placental perfusion – uterine there is more risk of fetal harm and on the other hand offset the drop in pressure using rapid infusion of isotonic fluids may cause pulmonary edema and the patient’s response to vasopressor drugs may be dramatic (5, 6).
Previous studies have noted that perhaps one way to reduce complications of spinal anesthesia can be the reduction of the dose of medication and they have compared the dose of the reduced drug of spinal anesthesia to epidural analgesia procedures. They evaluated the efficacy of this method in establishing anesthesia (7, 8). According to our information, most previous studies have either compared different regional anesthesia methods or studied a method in patients with preeclampsia and normal patients. But so far only a pilot study on a limited number of patients compared different doses of bupivacaine used for spinal anesthesia in patients with severe pre-eclampsia. The aim of this study was to evaluate differences in the use of low-dose and high-dose bupivacaine on the drop in blood pressure in patients with severe preeclampsia who delivered by cesarean section.
Materials and Methods
In this study clinical trial is used. Patients with severe preeclampsia (high blood pressure 160/110 mmHg, proteinuria, epigastric pain and impaired vision), who referred to Taleghani Hospital in Arak who wanted to deliver by cesarean section were enrolled in study. Exclusion criteria included: platelet count less than 100,000 per microliter, ASA class III and above, sensitivity to local anesthetics, history of heart failure or kidney or liver disease, history of neurological disease, history of psychiatry, the patient’s lack of cooperation in determining the sensory level and the failure of spinal anesthesia. The study was approved by University of Medical Sciences Research Ethics Committee number IR.Arakmu.REC.1395.913 / 3/95. And in all stages of research, the provisions of the Declaration of Helsinki and all the letters of Ethics Committee of the Ministry of Health, Treatment and Medical Education were followed. This study with the numberIRCT2016091714056N9 was registered in Registration Database of Clinical studies in Iran.
After obtaining informed consent, patients were randomly divided into two groups: the first group of candidates for spinal anesthesia using a low dose (7.5 mg) of bupivacaine 0.5% and the second were candidate for spinal anesthesia using conventional dose (12.5 mg) bupivacaine 0.5%. Blood pressure, oxygen saturation and heart rate of patients were recorded before any intervention, as the basic parameters. Both groups of patients receive the 200 cc Ringer before spinal anesthesia. For spinal anesthesia, patients were sitting and anesthetic was injected by means of needle No. 25 quincke and in L4-L5 vertebral space.
Immediately after injection of local anesthesia, patients were placed in mild Trendelenburg position and the desired level of anesthesia was considered as T4. And those whose anesthesia level was lower than T6 were considered as failure of spinal anesthesia and were removed from the study. For all patients50 micrograms fentanyl was infused intravenously before surgery and for pain. Systolic and diastolic blood pressure and heart rate in the first minute and then every 5 minutes until the end of surgery were recorded. The Apgar score of babies in 1 and 5 minute after birth in both groups were recorded.In the process of investigating anesthesiologist responsible for data entry and all patients were unaware of the drug.To compare the mean of data, t test was used and repeated measure method was used to measure changes in data that were repeatedly assessed. P value less than 0.05 was considered statistically as significant level.
Results
Taking into account the inclusion and exclusion criteria, 30 patients were enrolled in each group. The average age of patients in group I than in group II were 23.93±4.83 years and 25.36 ± 4.15 years, respectively, with no significant differences. Also, the body mass index in group 1 was equal to 30.59 ± 1.74 and in the second group was equal to 30.01 ± 1.59 that had no significant differences. Also, in the average baseline systolic blood pressure, basic diastolic blood pressure, mean of arterial blood pressure and heart rate there was no significant difference between the two groups (Table 1).
Table 1: The basic parameters of the two groups before surgery
| First group | Second Group | |
| Mean of systolic blood pressure (mmhg) | 145.73 ± 6.79 | 148.36 ± 10.51 |
| Mean of diastolic blood pressure (mmhg) | 86.23 ± 8.27 | 84.46 ± 6.71 |
| Mean of arterial pressure (mmhg) | 105.33 ± 8.45 | 107.53 ± 5.96 |
| The average number of heart beats per minute | 106.63 ± 8.95 | 108.43 ± 8.67 |
The duration of getting the anesthesia level to T10 in the first group was equal to 9 ± 1.14 minutes and second group was equal to 6.66 ±0.66 minutes and duration of getting anesthesia to T4 level in the first group was equal to 10.83 ± 1.05 minutes and the second group was equal to 8.23 ± 0.85 minutes. The average amount of each variable in the second group was significantly lower than the first group. Also for the mean Apgar score of babies at one and five minutes a significant difference was not observed. (Table 2) .
Table 2: Comparison of Apgar score of infants in the two groups
| Apgar of 1 minute | 8.33 ±0.71 | 8.4 ± 0.62 |
| Apgar of 5 minute | 9.86 ± 0.34 | 9.93 ± 0.25 |
To investigate changes in mean of heart rate, mean of systolic and diastolic blood pressure, and mean of arterial blood pressure in groups and to investigate the differences between them, the variance with repeated measures were used. Mauchly’ssphericity test result in all the above parameters has rejected sphericity (p<0.001), therefore, assuming non-sphericity data, the correction Greenhouse-Geisser test was used. For variable of heart rate, test results of Greenhouse-Geisser shows that our independent variable, i.e., the drug used for spinal anesthesia on heart rate for intra-group has significant effects (p=0.04 and f= 2.19). Between-group analysis showed that the difference between the average heart rate between the groups were not statistically significant. (P= 0.31 and F= 1.04). (Figure 1).
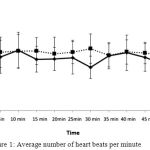 |
Figure 1: Average number of heart beats per minute
|
Between the two groups there was no significant difference in average heart rate
For the variable of mean of arterial pressure test results of Greenhouse-Geisser shows that our independent variable, i.e., the drug used for spinal anesthesia onmean of arterial pressure for intra-group has significant effects (p<0.0001 and F=32.44). And the mean arterial blood pressure significantly decreased in both groups compared to baseline but the average amount of the reduction between the two groups were not statistically different. (p=0.27 and f=1.20). (Figure 2).
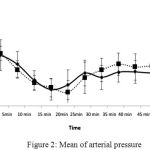 |
Figure 2: Mean of arterial pressure
|
Between the two groups there is no significant difference in mean of arterial pressure
For mean of systolic and diastolic blood pressure test results of Greenhouse-Geisser shows that our independent variable, i.e., the drug used for spinal anesthesia onmean of arterial pressure for intra-group has significant effects (p< 0.0001and F=195.28 ) and (p<0.0001 and f=50.77).And this means the mean of systolic and diastolic blood pressure significantly decreased in both groups compared to baseline but the average amount of the reduction between the two groups were not statistically different. (p=0.22 and f=1.52) and (p=0.92 and f=.0.009). (Figure 3 and 4).
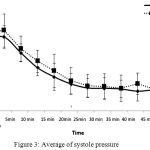 |
Figure 3: Average of systole pressure
|
There are no significant differences between the two groups in terms of mean of systolic pressure
 |
Figure 4: Average of diastolic pressure
|
Between the two groups there was no significant difference in the mean of diastolic pressure
Discussion
Our study shows that spinal anesthesia with low dose of bupivacaine prolongs the time to reach T4 anesthetic level. However given that the suitable anesthesia in all patients for surgery was achieved. Despite a significant mean arterial blood pressure, decrease there was no clinically significant difference. In this study we also concluded that the reduction in mean arterial blood pressure between the two groups receiving conventional-dose and low-dose of bupivacaine are not significantly different from each other. Previous studies have shown that spinal anesthesia with bupivacaine causes a drop in blood pressure and to control the situation requires injecting large volumes of saline or vasopressor drugs (8-11).
The results of our study were different from a pilot study conducted in 2012 by Jain and colleagues (12). They used low doses of bupivacaine (7.5 mg) compared with a dose of 10 mg, which reduces the number of people with drop in blood pressure. In their study they did not study average blood pressure that may be the cause of differences in our results.
Ramanathan and his colleagues in their study in 2001 reported that the use of low-dose bupivacaine with epidural anesthesia when needed can create ideal conditions for cesarean surgery (7). We had drop of blood pressure in both groups in this study but despite a significant decrease; there was no clinically significant difference. The results of our study are consistent with part of the results of a study conducted by Visalyaputra et al. in 2005, in which they studied epidural and spinal anesthesia in patients with severe pre-eclampsia. They noted that at the beginning and end of surgery between mean of arterial blood pressure there was no difference in both methods(8).
The results Nikseresht and colleagues in 2016 has shown that local anesthesia using low dose bupivacaine takes place with low risk drop in blood pressure in patients with severe pre-eclampsia (13). Previous studies have also shown that the use of vasopressor drugs in patients with preeclampsia is less compared to normal patients (14). In the above studies only Visalyaputra and his colleagues compared the numerical value of average blood pressure over time, but they used t-test to do the comparison while we used repeated measure statistical method in this study. In this method the changes of the measured parameters within the group and between groups are examined and offer us more accurate results. Also in other listed studies the number of episodes of decreased blood pressure has been investigated further.
Conclusion
The findings of this study showed that low dose of bupivacaine(7.5mg) is suitable for cesarean section in severe preeclampsia. However incidence of hemodynamic change hadn‘t significant difference versus conventional dose(12.5mg)
Acknowledgements
The authors would like to thank, the Department of Research and Technology Arak University of Medical Science for his spiritual and material aid.
References
- Aya AG, Mangin R, Vialles N, Ferrer J-M, Robert C, Ripart J, et al. Patients with severe preeclampsia experience less hypotension during spinal anesthesia for elective cesarean delivery than healthy parturients: a prospective cohort comparison. Anesthesia & Analgesia. 2003;97(3):867-72.
CrossRef - Chumpathong S, Sirithanetbhol S, Salakij B, Visalyaputra S, Parakkamodom S, Wataganara T. Maternal and neonatal outcomes in women with severe pre-eclampsia undergoing cesarean section: a 10-year retrospective study from a single tertiary care center: anesthetic point of view. The Journal of Maternal-Fetal & Neonatal Medicine. 2016:1-5.
CrossRef - Pournajafian A, Rokhtabnak F, Kholdbarin A, Ghodrati M, Ghavam S. Comparison of remifentanil and fentanyl regarding hemodynamic changes due to endotracheal intubation in preeclamptic parturient candidate for cesarean delivery. Anesthesiology and pain medicine. 2012;2(2):90-3.
CrossRef - Riley ET, Cohen SE, Macario A, Desai JB, Ratner EF. Spinal versus epidural anesthesia for cesarean section: a comparison of time efficiency, costs, charges, and complications. Anesthesia & Analgesia. 1995;80(4):709-12.
- Sibai BM, Mabie BC, Harvey CJ, Gonzalez AR. Pulmonary edema in severe preeclampsia-eclampsia: analysis of thirty-seven consecutive cases. American journal of obstetrics and gynecology. 1987;156(5):1174-9.
CrossRef - Wright JP. Anesthetic Considerations in Preeclampsia-Eclampsia. Anesthesia & Analgesia. 1983;62(6):590-601.
CrossRef - Ramanathan J, Vaddadi AK, Arheart KL. Combined spinal and epidural anesthesia with low doses of intrathecal bupivacaine in women with severe preeclampsia: a preliminary report. Regional anesthesia and pain medicine. 2001;26(1):46-51.
- Visalyaputra S, Rodanant O, Somboonviboon W, Tantivitayatan K, Thienthong S, Saengchote W. Spinal versus epidural anesthesia for cesarean delivery in severe preeclampsia: a prospective randomized, multicenter study. Anesthesia & Analgesia. 2005;101(3):862-8.
CrossRef - Ankichetty SP, Chin KJ, Chan VW, Sahajanandan R, Tan H, Grewal A, et al. Regional anesthesia in patients with pregnancy induced hypertension. Journal of Anaesthesiology Clinical Pharmacology. 2013;29(4):435.
CrossRef - Hood DD, Curry R. Spinal versus epidural anesthesia for cesarean section in severely preeclamptic patients a retrospective survey. The Journal of the American Society of Anesthesiologists. 1999;90(5):1276-82.
- Santos AC, Birnbach DJ. Spinal anesthesia for cesarean delivery in severely preeclamptic women: don’t throw out the baby with the bathwater! Anesthesia & Analgesia. 2005;101(3):859-61.
CrossRef - Jain K, Makkar J, Yadanappudi S, Anbarasan I, Gander S. Two doses of spinal bupivacaine for caesarean delivery in severe preeclampsia: A pilot study. International journal of obstetric anesthesia. 2012;21(2):195-6.
CrossRef - Nikooseresht M, Rabiei MAS, Hajian P, Dastaran R, Alipour N. Comparing the Hemodynamic Effects of Spinal Anesthesia in Preeclamptic and Healthy Parturients During Cesarean Section. Anesthesiology and Pain Medicine. 2016(In Press).
CrossRef - Saha D, Ghosh S, Bhattacharyya S, Mallik S, Pal R, Niyogi M, et al. Comparison of hemodynamic response and vasopressor requirement following spinal anaesthesia between normotensive and severe preeclamptic women undergoing caesarean section: A prospective study. Journal of Obstetric Anaesthesia and Critical Care. 2013;3(1):23.
CrossRef

