
Roya Fallahian, Mojgan Kalantary, Elham Keshavarz and Kobra Mohammadi
Department of Radiology, Mahdieh Hospital, Shahid Beheshti University of Medical Science, Tehran, Iran.
Corresponding Author E-mail: Mojgankalantary@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1178
Abstract
Echogenic intracardiac focus (EIF) is in fact a bright echogenic region in the heart of fetus. There are conflicting reports concerning the existence of EIF and affliction of fetus with major trisomies. Thus, the present research seeks to evaluate and assess the prevalence of EIF in the second trimester ultrasound screening and their postpartum follow-up. Based on the sample volume of this research, 1000 pregnant women resorting to Mahdiye Hospital for the second trimester ultrasound screening from 2014 to 2015 were selected for this descriptive research and studied for presence of EIF. The postpartum information of neonatals in terms of affliction with major trisomies was also studied and recorded. Finally, the prevalence of EIF and its correlation with major trisomies was taken into consideration. The mothers taking part in our study aged 24 to 36 years old with an average of 29.05 ± 3.56 years. The results showed existence of EIF in 3.8% of all fetuses. The prevalence of down syndrome among the population studied was 0.4% with all having EIF. All these cases belonged to mothers younger than 35 years. Positive predictive value (PPV), false predictive rate (FPR), sensitivity and exclusiveness of EIF for diagnosis of affliction with trisomy 21 in the population studied was 10, 3.4, 100, and 96.6% respectively. The results pointed to the fact that gender of fetus shows no such significant difference in the rate of affliction with down syndrome (P-value > 0.5). It also turned out that the number of EIF discovered in people with down syndrome showed a statistically significant difference compared to normal fetuses (P-value < 0.5). Based on the results achieved in this research, it is concluded that diagnosing EIF through ultrasound screening is correlated with the higher possibility of affliction with down syndrome. Presence of EIF can also act as a strong marker to predict existence of major trisomic abnormalities.
Keywords
EIF; Down Syndrome Major Chromosomal Abnormalities;Ultrasound Screening;
Download this article as:| Copy the following to cite this article: Fallahian R, Kalantary M, Keshavarz E, Mohammadi K. Assessing the Prevalence of EIF in Second Trimester Ultrasound Screening in the Fetuses of Mothers Resorting to Mahdiyeh Medical Center of Tehran from 2014 To 2016 and their Follow Up. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Fallahian R, Kalantary M, Keshavarz E, Mohammadi K. Assessing the Prevalence of EIF in Second Trimester Ultrasound Screening in the Fetuses of Mothers Resorting to Mahdiyeh Medical Center of Tehran from 2014 To 2016 and their Follow Up. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=15007 |
Introduction
One of the sonographic markers studied during second trimester fetus sonography is echogenic intracardiac focus (EIF). EIF a sonographic finding consisting of a bright echogenic area in the heart of fetus with a brightness similar to a bone1 that moves synchronically towards atrioventricular valves.2 This Echogenicity is probably a symptom of microcalcification of papillary muscles or chordae tendineae.3 EIF sonographic finding was first reported in midwifery sonographies in late 1980s.4 In second trimester of ultrasound screening, EIF is observed in 0.17 to 20% of all pregnancies and it is more prevalent among Asian race. It is generally observed in 5.6% of natural fetuses5,6 and 25 to 30% of fetuses afflicted with trisomy 21. There may be 1 to several echogenic areas in the heart mostly observed in the left ventricle.7 The correlation between EIF and Aneuploidy was not yet clear until mid-1990s.8 Although more cases of EIF are observed among fetuses with trisomy 21 than those without trisomy 21, only 11 to 15 cases of each 100 fetuses with isolated EIF are afflicted with trisomy 21.9,10 The important point to be taken into consideration is that prevalence of EIF in various scientific texts differs significantly.11 These changes and variations depend on so many factors including (but not limited to) technical and racial factors.12 Smith-Bindman conducted a meta-analysis on the studies finding a correlationship between EIF and trisomy 21. This analysis showed if we fail to diagnose EIF, the risk of trisomy 21 will rise 2.8 times (9). Based upon recent larg-scale meta-analysis, the possibility of affliction with trisomy 21 will increase 5.4 to 6.2 folds if there is an isolated EIF in ultrasound screening.13 Down syndrome is one of the most common chromosomal disorders in humans whose prevalence (according to WHO) ranges from 1 in 1000 to 1 in 1100 live births in the world.14 Various risk factors have been proposed for this syndrome, but the most important one seems to be old age of pregnancy, while other chromosomal disorders and blood affinity of parents are not considered risk factors.15 Further to the problems caused for their families, a kid suffering from down syndrome or other major aneuploidies costs a high price for health and treatment system.16 As a result, diagnosis of down syndrome and legal abortion is of significant importance. The majority of information is obtained from western countries, as a result, it is crucial to study other societies as well. On the other hand, discrepancies between the reports concerning the correlation between EIF and down syndrome highlights the importance of such researches. The present research seeks to determine the prevalence of EIF in the second trimester ultrasound screening of fetuses of mothers resorting to Mahdiyeh Medical Center of Tehran from 2014 to 2015 and their postpartum follow up in terms of major trisomies.
Materials and Method
This is a descriptive research conducted which lasted from 2014 to mid-2016. The participants included all pregnant women resorting to Mahdiye Hospital of Tehran for the second trimester ultrasonic analysis. With due observation of medical ethics principles and after gaining their consent, the patients took part in the research voluntarily. Based upon previous studies and with due observation of inclusion criteria, as many as 1000 participants were chosen for each group. These mothers were examined for EIF in the heart of fetus through the second trimester ultrasound screening. In the postpartum period, the information was recorded in terms of fetal normality or affliction with major trisomies. IBM SPSS Statistics v.21 was used to analyze the data. Further to determining the rate of frequency, EIF finding was used as a diagonal marker to predict the occurrence of chromosomal disorders and diagonal parameters such as sensitivity and exclusiveness of FPR, PPV, NPV, and ACC indicators were calculated. Non-parametric Chi-square test was used for data analysis and the levels of significance (P-Value < 0.05) were also studied.
Results
Mothers with fetuses with EIF aged 24 to 36 with an average age of 29.05 ± 3.564. Of the whole 38 fetuses with EIF in this research, 24 (63%) were female while 14 (37%) were male. The fetuses also aged 15.86 to 23.57 weeks with an average age of 19.195 ± 1.444. Out of 38 neonatals with EIF in postpartum period, 4 (10.5%) had trisomy 21 syndrome chromosomal disorder and the rest (89.5%) were healthy. A review of the prevalence of chromosomal disorders in terms of fetuses’ gender with EIF showed that of the whole 14 male fetuses with EIF, 12 (85.7%) were normal in postpartum period while 2 (14.3%) were suffering from trisomy 21. As for female fetuses, there were 22 (91.6%) normal neonatals and 2 (8.3%) afflicted with trisomy 21. As a result, the ratio of affliction with trisomy 21 abnormality among males with EIF was 1.75 times more than what was observed among female fetuses (chart 1).
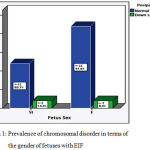 |
Graph 1: Prevalence of chromosomal disorder in terms of the gender of fetuses with EIF |
Then mothers diagnosed with fetuses with EIF were divided into two groups in terms of their age: those younger than or as old as 35 and those older than 35. 32 of those mothers younger than 35 whose fetuses were diagnosed with EIF had healthy kids after birth, while 4 mothers with the same age condition and sonographic results had given birth to neonatals with trisomy 21 genetic disorders. Among those participants older than 35, 2 mothers whose fetuses were diagnosed with EIF had healthy kids after delivery (chart 2).
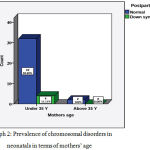 |
Graph 2: Prevalence of chromosomal disorders in neonatals in terms of mothers’ age
|
The present research has taken into consideration the correlation between two variables of EIF and down syndrome disorder (table 1). Analyses have pointed to a statistically significant correlation between presence of EIF and affliction with down syndrome disorder (P-value < 0.05). In the group diagnosed with EIF, 4 neonatals were afflicted with down syndrome but none of those neonatals without EIF were suffering from down syndrome or other major chromosomal disorders.
Table 1: Distribution and assessment of the correlation between EIF and down syndrome disorder
| EIF | Total | P-value | |||
| Yes | No | ||||
| Postpartum status of neonatal | Down syndrome | 4 | 0 | 4 | 0.001 |
| Normal | 34 | 962 | 996 | ||
The result of the analysis of the correlation between gender of fetuses with EIF and affliction with postpartum down syndrome abnormalities showed no statistically significant correlation between fetuses’ gender and occurrence of chromosomal disorders (P-value > 0.05). The prevalence of down syndrome disorder among the population studied was 0.4% (with a certainty interval of 95% from 0.001 to 0.01). All neonatals with down syndrome were diagnosed with EIF during their prenatal period. The prevalence of fetuses with EIF was calculated to be around 3.8% (95% confidence interval, 0.0278-0.0517). considering the number of those with down syndrome disorder in postpartum period, the sensitivity (TPR) and exclusiveness (TNR) of EIF marker were calculated as markers which could diagnose postpartum chromosomal disorders. The sensitivity and exclusiveness of EIF to diagnose down syndrome disorder were 100% and 96.6%.
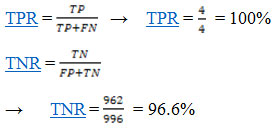
False positive rate (FPR) for fetuses with EIF for affliction with down syndrome disorders in postpartum period was 3.4%. In this research, positive predictive value (PPV) which shows the possibility of having someone with positive test results was calculated 10%.
Discussion
Echogenic intracardiac focus is the result of calcification in papillary muscles and fibrosis first described by Schechter et al in 1987.17 Although this is considered a normal status, some researchers use it as a sonographic marker for chromosomal disorders and cardiac complications, particularly for pregnant mothers.6 As invasive tests to diagnose fetal disorders usually have a high risk of abortion, finding reliable and authorized markers to diagnose such disorders is of significant importance. Contradictory findings about the correlation between EIF and major trisomies and its prevalence rate have made it impossible to draw and open and clear picture of the potential and effectiveness of this marker. The present research was designed to measure the prevalence of EIF and its correlation with major trisomies in Iranian race. As previous researches have confirmed that there is no correlation between EIF and cardiac anomaly,18,19 this research didn’t use complementary examinations such as postpartum echo. The results showed a prevalence rate of 3.8% and 0.4% for EIF and down syndrome in the population studied. All kids with down syndrome were diagnosed with EIF during the prenatal period. In other words, out of 38 neonatals with EIF after birth, 4 (10.5%) had trisomy 21 syndrome chromosomal disorders while the rest (89.5%) were healthy. An analysis of the researches conducted in this field and the prevalence rate reported by them, an agreement with the results achieved in the present research was observed; however, some discrepancies also exist. For example, Bromley et al reported a prevalence rate of 4.9% for EIF and 18% for down syndrome with EIF. Although this research has reported and EIF prevalence rate quite close to our results, a high 21 trisomy prevalence rate is reported. At the end of their research, they arrived at the conclusion that a fetus with EIF is exposed to the significant and increased danger of down syndrome.8 In the research by Huggon et al on 6904 cases of pregnancy, the prevalence of EIF was reported to be 13.1% which was much higher than the rate observed in our research. They also arrived at the conclusion that the prevalence of fetal EIF in fetuses with trisomy 21 is 2.93 times more than what was observed in normal fetuses; however, our research failed to find any cases of trisomy 21 in fetuses without EIF finding.20 In another example, we may point to the research by Anderson et al (2003). Out of 12373 cases of pregnancy studied, they reported 267 cases of EIF (2.1%) and 38 cases of trisomy 21 disorder (0.31%).21 Although the prevalence rate reported in this research is close to the values reported in our research, the values are lower. In 2010, Gupta et al estimated the prevalence of fetal EIF around 6.3% and reported the prevalence of down syndrome with EIF about 23%. Finally, they arrived at the conclusion that the mere presence of EIF in fetus has no negative effect on neonatal’s status. The prevalence of EIF in this research is in a timespan close to that of ours, but a higher rate of prevalence was reported for greater abnormalities.22 In a research by Mirza et al (2015), the prevalence of EIF was reported to be around 2.5% and they concluded that there is no correlation between EIF and trisomy 21.11 Researchers have not yet achieved an agreement on existence of a correlation between EIF and occurrence of genetic syndrome. As it was pointed in researchers’ conclusion, some believe in such a correlation, while others deny it. According to the results achieved in our research, a statistically significant correlation existed between existence of EIF and affliction with down syndrome abnormalities and all neonatals with down syndrome were born to mothers younger than 35. This part of the research contradicts some other studies. For instance, in the research conducted by Anderson et al, finding EIF in the fetuses of women younger than 35 was equal to 2.1%, while this value among those mothers older than 35 was 3.4% with no unnatural or trisomy 21 case among women aging 18 to 34. This is not in line with our research.21 In our research, sensitivity (TPR), exclusiveness (TNR), false positive rate (FPR), and positive predictive value (PPV) of EIF marker as a predictive and diagonal marker of chromosomal disorder were 100, 96.6, 3.4, and 10%, respectively. A comparison of the results of this part of research with those of other researches points to significant differences some of which are discusses here. For instance, in the research by Bromely et al, sensitivity, exclusiveness, and positive predictive value reported for using presence of an EIF to diagnose a fetus afflicted with down syndrome was 18.2, 95.3, and 6.1% respectively. Another example is the research by Thomas et al. where the positive predictive value of EIF for affliction with trisomy 21 in the population studied was 9.8%, while values of 30% and 95% were reported for sensitivity and exclusiveness respectively.23 Although there are differences between there results, the results of studies show that EIF has a high degree of exclusiveness for diagnosing down syndrome. A general review of the topic shows that statistical parameters concerning EIF reported in the scientific texts have significant differences with one another. These differences can be attributed to factors such as sample volume, technical and racial factors, etc.
Conclusion
Based on the results of this research, we may conclude that the prevalence rate of EIF and down syndrome calculated in this research is a moderate rate close to its global value. The results also pointed to a statistically significant correlation between the existence of EIF and affliction with down syndrome. As a result, it can be used as a useful and high potential marker to predict occurrence of at least this postpartum genetic disorder. Another observation made in this research is that fetus’s gender plays no role in affliction with down syndrome, but the number female fetuses with EIF is more than male ones.
References
- Perles Z., Nir A., Gavri S., Golender J., Rein A. J. Intracardiac echogenic foci have no hemodynamic significance in the fetus. Pediatr Cardiol. 2010;31(1):7-10.
CrossRef - Facio M. C., Hervias-Vivancos B., Broullon J. R., Avila J., Fajardo-Exposito M. A., Bartha J. L. Cardiac biometry and function in euploid fetuses with intracardiac echogenic foci. Prenat Diagn. 2012;32(2):113-6.
CrossRef - Hamdan M. A., El Zoabi B. A., Al Shamsi A., Bekdache G. N., Chedid F. Fetal echogenic cardiac foci: prospective postnatal electrocardiographic follow-up. J Perinatol. 2013;33(4):268-70.
CrossRef - Schechter A. G., Fakhry J., Shapiro L. R., Gewitz M. H. The left ventricular echogenic focus. AJR Am J Roentgenol. 1988;150(6):1445-6.
CrossRef - Shipp T., Bromley B., Lieberman E., Benacerraf B. The frequency of the detection of fetal echogenic intracardiac foci with respect to maternal race. Ultrasound in Obstetrics and Gynecology. 2000;15(6):460-2.
CrossRef - Shakoor S., Ismail H., Munim S. Intracardiac echogenic focus and fetal outcome–review of cases from a tertiary care centre in Karachi, Pakistan. The Journal of Maternal-Fetal & Neonatal Medicine. 2013;26(1):2-4.
CrossRef - Kurtulmus S., Mese T., Taner C. E., Oztekin D. C., Okyay D., Uysal A., et al. Evaluation of tissue Doppler-derived myocardial performance index in fetuses with intracardiac echogenic focus. J Matern Fetal Neonatal Med. 2013;26(16):1662-6.
CrossRef - Bromley B., Lieberman E., Laboda L., Benacerraf B. R. Echogenic intracardiac focus: a sonographic sign for fetal Down syndrome. Obstetrics and gynecology. 1995;86(6):998-1001.
CrossRef - Smith-Bindman R., Hosmer W., Feldstein V. A., Deeks J. J., Goldberg J. D. Second-trimester ultrasound to detect fetuses with Down syndrome: a meta-analysis. JAMA. 2001;285(8):1044-55.
CrossRef - Wax J. R., Donnelly J., Carpenter M., Chard R., Pinette M. G., Blackstone J., et al. Childhood cardiac function after prenatal diagnosis of intracardiac echogenic foci. J Ultrasound Med. 2003;22(8):783-7.
CrossRef - Mirza F. G., Ghulmiyyah L., Tamim H., Hamdan F. B., Breidy J., Geagea S., et al. Echogenic intracardiac focus on second trimester ultrasound: prevalence and significance in a Middle Eastern population. J Matern Fetal Neonatal Med. 2016;29(14):2293-6.
- Tran S. H., Caughey A. B., Norton M. E. Ethnic variation in the prevalence of echogenic intracardiac foci and the association with Down syndrome. Ultrasound Obstet Gynecol. 2005;26(2):158-61.
CrossRef - Agathokleous M., Chaveeva P., Poon L. C., Kosinski P., Nicolaides K. H. Meta-analysis of second-trimester markers for trisomy 21. Ultrasound Obstet Gynecol. 2013;41(3):247-61.
CrossRef - http://www.who.int/genomics/public/geneticdiseases/en/index1.html.
- Qi G., Yi J., Han B., Liu H., Guo W., Shi C., et al. Noninvasive prenatal testing in routine clinical practice for a high-risk population: Experience from a center. Medicine (Baltimore). 2016;95(41):e5126.
CrossRef - Kazemi M., Salehi M., Kheirollahi M. Down Syndrome: Current Status, Challenges and Future Perspectives. International Journal of Molecular and Cellular Medicine. 2016;5(3):125-33.
- Schechter A., Fakhry J., Shapiro L., Gewitz M. In utero thickening of the chordae tendinae. A cause of intracardiac echogenic foci. Journal of ultrasound in medicine. 1987;6(12):691-5.
CrossRef - Arda S., Sayın N. C., Varol F. G., Süt N. Isolated fetal intracardiac hyperechogenic focus associated with neonatal outcome and triple test results. Arch Gynecol Obstet. 2007;276(5):481-5.
CrossRef - Bethune M. Management options for echogenic intracardiac focus and choroid plexus cysts a review including Australian Association of Obstetrical and Gynaecological Ultrasonologists consensus statement. Australas Radiol. 2007;51(4):324-9.
CrossRef - Huggon I., Cook A., Simpson J., Smeeton N., Sharland G. Isolated echogenic foci in the fetal heart as marker of chromosomal abnormality. Ultrasound in Obstetrics & Gynecology. 2001;17(1):11-6.
CrossRef - Anderson N., Jyoti R. Relationship of isolated fetal intracardiac echogenic focus to trisomy 21 at the mid-trimester sonogram in women younger than 35 years. Ultrasound in obstetrics & gynecology:the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2003;21(4):354-8.
CrossRef - Gupta G., Aggarwal S., Phadke S. R. Intracardiac echogenic focus and fetal outcome. Journal of Clinical Ultrasound. 2010;38(9):466-9.
CrossRef - Winter T. C., Anderson A. M., Cheng E. Y., Komarniski C. A., Souter V. L., Uhrich S. B., et al. Echogenic Intracardiac Focus in 2nd-Trimester Fetuses with Trisomy 21. Usefulness as a US Marker 1. Radiology. 2000;216(2):450-6.
CrossRef

