
Kajaria Divya, Tripathi J. S. and Tiwari S. K.
Department of Kayachikitsa, Faculty of Ayurveda, Institute of Medical Sciences, B.H.U.- 221005, Varanasi, India.
Corresponding Author E-mail: divyakajaria@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1169
Abstract
The present study aims to search a drug that acts on platelet aggregation to validate the fact that preventing platelet aggregation is helpful in successful management of bronchial asthma in addition with the effect on previously proved mechanism. With this aim it was planned to search the effect of a polyherbal drug - Shirishadi on platelet aggregation. It is worthy here to mention that this drug (Shirishadi) is chosen on the basis of clinical evidence suggesting its potent anti-asthmatic effect. Anti-platelet property of Shirishadi polyherbal compound was evaluated using thrombin induced platelet aggregation isolated from human blood (collected from healthy volunteers) by differential centrifugation. Under in vitro conditions, 15 min pre-incubation with the Shirishadi polyherbal compound (200µg/ml) significantly (p< 0.001) inhibit thrombin- induced platelet aggregation. These findings suggest that Shirishadi, a polyherbal formulation possesses potent anti-platelet aggregation activity in the experimental models of in vitro platelet aggregation.
Keywords
Bronchial asthma; Shirishadi polyherbal compound Unhinged platelet aggregation;
Download this article as:| Copy the following to cite this article: Divya K, Tripathi J. S, Tiwari S. K. Anti-Platelet Aggregating Activity of A Polyherbal Compound- Shirishadi- In Vitro Study. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Divya K, Tripathi J. S, Tiwari S. K. Anti-Platelet Aggregating Activity of A Polyherbal Compound- Shirishadi- In Vitro Study. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=14813 |
Introduction
Recent researches have shown that alteration in blood flow or airway perfusion modifies smooth muscle contraction. Bronchial muscle contractility is much more influence by the vascular component rather than allergen specific chemical spasmogens as was earlier believed. Even a slight change in airway perfusion (mild diastolic hypertension) can markedly alter the bronchial smooth muscle response. A study conducted by Csete et. al. for assessing the effect of airway blood flow on smooth muscle contraction response challenged by allergens by measuring the clearance of locally released spasmogens.1 The study concluded that antigen induced airway smooth muscle contraction occurs due to alterations in airway perfusion rather than airway smooth muscle response to chemical mediators. This study suggests that the amount of chemical mediators reaches to the circulation is relatively small and therefore generating lesser potential to elicit response in comparison to potent vascular response. Previous studies have also shown that vascular endothelium growth factor (VGEF), plays a vital role in airway remodelling as it is responsible for fibrosis associated with neovascularisation resulting in thickening of basement membrane.2 In asthma, airway remodelling is due to inflammation caused by permanent lesion in the endothelium layer that control vascular homeostasis. Another important factor that is found to have regulatory function in maintaining vascular integrity and quiescence is angiopoietin (Ang)- Tie ligand – receptor system.3 This system is responsible for angiogenesis and also for maintaining the resting/ quiescent state of the endothelium. Disturbance in this system (Ang-1- mediated Tie 2 activation) causes expression of various surface receptors like Intercellular Adhesion Molecule (ICAM-1), Platelet Endothelial Cell Adhesion Molecule (PECAM-1) and E selectin, which in turn causes recruitment of inflammatory cell and thrombus formation. Role of platelet in the development of inflammation is often decisive and vital to some extent. There may be several mechanisms by which platelets participate in the inflammatory response; it may act as sentinel cells checking the microbial invasion, regulating leukocyte recruitment, or may act as innate inflammatory cells causing damage and influencing repair process. Research studies have shown that allergens induced chemicals increases platelet activation which in turn disturbs platelet aggregation and finally produces bronchial hyper-responsiveness.4 The mechanism of platelet activation by allergen induced anaphylaxis is distinct from the normal aggregating stimuli like arachidonic acid (AA) and adenosine diphosphate (ADP).Non steroidal inflammatory drugs (NSAIDs) that are anti-inflammatory and anti-platelet aggregating agent are supposed to block platelet aggregation (eg. aspirin) through arachidonic acid pathway but do not hamper platelet – leukocyte interaction.5,6 This fact gives a clue about probable mechanism of platelet activation during inflammation caused by allergen induced chemical/ inflammatory mediators. Thus, it is very clear that disturb platelet function secondary to inflammation caused by allergens leads to airways remodelling and bronchial hyper responsiveness. Keeping this fact into focus it was decided to evaluate the anti-platelet aggregating activity of a polyherbal drug Shirishadi that is extensively use for the management of bronchial asthma and other allergic conditions like allergic rhinitis, urticaria etc. Shirishadi compound consist of three herbs namely Shirisha (Albizia lebbeck), Nagarmotha (Cyperus rotandus) and Kantakari (Solanum xanthocarpum). In Ayurvedic system of medicine, Shirisha (Albizzia lebbeck) is mainly use for treating allergic disorder and is consider as anti-toxin agent. Previous researches showed that it has potent anti-allergic properties7,8; it helps in process of desensitization and reduces the antigen-antibody interation.9,10,11 According to Ayurveda the root cause of every disease is indigested food. The indigested food acts as toxin.12,13 In research studies it is found that if, small dose of toxin administered in cell, the IgG produce in its response is sufficient enough to countermand the hypersensitivity response of IgE.14 Thus endogenous toxins (indigested food) act as allergen provoking allergic response.15,16 Action of Shirisha (Albizzia lebbeck) in reducing IgE is well documented. Nagarmotha (Cyprus rotandus) is reported to have potent antioxidant and free radicals scavenging effect17 thus suppose to be effective in oxidative stress induced diseases like allergy,asthma,COPD,autoimmune disorders etc. According to Ayurveda, Nagarmotha is said to be best for digestive tract diseases as it helps in digestion of food toxins. Kantakari (Solanum xanthocarpum)is found to be very effective in respiratory tract diseases like Bronchial Asthma, COPD, allergic rhinitis etc. Salasodin, Apigenin,Stigmasterol, Carpesterol & Diosegenin are the main chemical component of Solnum xanthocarpum. It is reported to have bronchodilator, anti-allergic & anti-inflammatory properties.18 The combination of these three herbs is found to be very effective in allergic disorders and abundantly use in treatment of Bronchial asthma. The present study aims to screen the anti-allergic and anticoagulant activity of drug and reviewing the molecular machinery and inflammatory pathway induced by platelet aggregation in allergic asthma.
Materials and Methods
Plant Material
The plants Albizzia lebbeck, Cyprus rotandus and Solanum xanthocarpum were collected from local market of Varanasi. The identification of the drugs was done by Prof.A.N. Singh, Department of Dravyaguna, S.S.U, Varanasi (Identification number DG/ AKS / 604).
Extraction of the Plant Material and Sample Preparation
Hydroalcoholic extraction (Distilled water: Ethanol = 2:1) of drug was carried out by hot percolation method through soxhlet apparatus. Thereafter extract was dried using rotatory evaporator and dried extract was put to the process of standardization. The percentage yield was noted.
Preparation of Platelets
Platelets were isolated from fresh human blood (collected from healthy volunteers) by the process of differential centrifugation. The fresh blood drawn from the healthy volunteers was put in citrate- phosphate- dextrose adenine and centrifuged at 180x g for 10min. PRP (platelet- rich plasma) was incubated with 1mM acetylsalicylic acid for 15min at 370C. After addition of EDTA (ethylenediaminetetraacetic acid)(5mM), platelets were sediment by centrifugation at 800x g for 15min. Cells were washed in buffer A (20mM hepes,138mM NaCl, 2.9mM KCl, 1mM MgCl2 0.36 mM Na H2 PO4 ,1 mM EGTA (ethylene glycol tetraacetic acid), supplemented with 5mM glucose and 0.6 ADPase units of apyrase/ml,pH 6.2). Platelets were finally resuspended in buffer B (ph 7.4), which was the same as buffer A, but without EGTA and apyrase. The final cell count was adjusted to 0.5-0.8x 109/ml. All steps were carried out under sterile conditions and precautions were taken to maintain the cells in resting condition.
Platelet Aggregation
Platelets were stirred (1200 rpm) at 370C for 2min in a Chronolog Whole Blood/Optical Lumi-Aggregometer (model 700-2) prior to the addition of agonists. Wherever indicated, cells were stimulated stirring to prevent aggregation. Aggregation was induced with the agonist thrombin (1U/ml). Aggregation was measured as percent change in light transmission, where 100% refers to transmittance through blank sample.
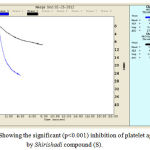 |
Figure 1: Showing the significant (p<0.001) inhibition of platelet aggregation by Shirishadi compound (S).
|
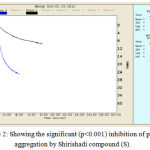 |
Figure 2: Showing the significant (p<0.001) inhibition of platelet aggregation by Shirishadi compound (S).
|
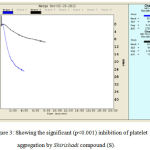 |
Figure 3: Showing the significant (p<0.001) inhibition of platelet aggregation by Shirishadi compound (S).
|
Result and Discussion
Shirishadi compound is an indigenous drug used from decades in Ayurvedic system of medicine for the treatment of allergic conditions like bronchial asthma. Recent advancement shows that asthma is a multifactorial complex disease involving many factors like inflammation, allergy and various inflammatory mediators like histamine, interlukines, cytokines and more recently and most concern factor i.e. Platelet activating factor. Role of platelet in the pathogenesis of asthma draw attention of scientist and medical professionals to search advancement in the treatment strategy. In recent year’s there is considerable increase in the need for understanding the critical role of platelets, coagulation, anticoagulant pathways and the fibronolytic system in the pathogenesis of asthma. In asthma, there exist perpetual impaired activities of the anticoagulant protein C system and fibrinolysis associated with a procoagulant state in bronchoalveolar space. In asthma, along with the disturbance in coagulation, there is additional disturbance exist between the balance of protease and antiprotease. Allergic response including leukocyte activation and mast cell activation significantly increases the load of protease in airways. Thus, protease activated receptors are consider as molecular link between inflammation due to allergic response and coagulation.19 In asthma liberation of various inflammatory mediators causes vascular congestion and platelet aggregation (eg. PAF induced platelet aggregation). Platelet aggregation further causes platelet activation and abrupt release of inflammatory and mutagenic substances into the microenvironment of airway vessels. These inflammatory mediators further trigger autocrine and paracrine activation causing recruitment of leukocyte into the vascular wall, altering the quiescence state of endothelium and produces damage to the intimal layer. The damaged endothelium expresses VGEF and causes airways remodelling, thus a vicious cycle set-up resulting in persistent airway inflammation. Evaluation of Shirishadi compound as anti platelet aggravating agent showed that it significantly inhibit the platelet aggregation (p<0.001) induced by thrombin. Thrombin- induced platelet aggregation was inhibited by 15 min pre-incubation with the Shirishadi extract at a concentration of 200µg/ml. Metabolomic study of hydroethanolic extract of Shirishadi polyherbal compound showed presence of forty bio-active constituents. The prevailing compounds Catechin, l-(+)-Ascorbic acid ,2, 6-dihexadecanoate and Alpha-cyperone contribute the anti-asthmatic, anti-oxidant and anti-platelet aggregating properties of the compound. GC- MS analysis of polyherbal compound showed that it contains principally the active component of Albizia lebbeck (Shirisha) i.e. Catechin followed by Dimethyl sulfone and glycerin. Active component of Cyperus rotandus, α Cyperone is contributed anti-platelet aggregating activity of the compound.
 |
Scheme 1
|
Previous studies showed that α-Cyperone, isolated from the rhizomes of Cyperus rotundus, through downregulation of NFκB signaling in RAW 264.7 (cell line murine macrophage from blood), inhibits lipopolysacchride (LPS) induced cyclooxygenase- 2 expression and prostaglandin (PGE2) production.20 Ethanolic extract of C. rotundus is found to inhibit both nitric oxide (NO) and prostaglandin (PGE2) production in cell line murine macrophage. In addition to this, α-cyperone is reported to downregulate the mRNA expression and production in response to inflammatory cytokine IL-6. Genomic studies showed that α-cyperone suppress the nuclear translocation of the p65 NFκB subunit and transcriptional activity of NFκB in RAW 264.7 cell line. Experimental studies showed that drug has potent anti-inflammatory property. The drug at the dose of 500mg/Kg bwt causes 81% inhibition in rat paw oedema at the end of 4h.21 The result confirms that drug is COX-2 inhibitor and subsequent inhibitor of PGE2. Thus it can be concluded that there is defective platelet function in asthmatic that cause deranged function of endothelium and expression of various surface receptors and VEGF producing inflammation and airways remodelling.
Conclusion
The study affirms that there is definite role of defective platelet function in the pathogenesis of bronchial asthma. Drugs having role in modulating the platelet response and thereby normalizing the functioning of endothelium should have promising result in the management of bronchial asthma. Shirishadi compound significantly inhibit the thrombin induced platelet aggregation cause healing of inflamed endothelium and prevent airways remodelling.
Acknowledgement
Authors extend their sincere thanks to Prof. D. Dash, Prof.& Head, Department of Biochemistry, IMS,BHU for his valuable support, kind guidance and providing the essential facilities for carrying out experimental study.
References
- Chetta A., Zanini A., Foresi A., D’Ippolito R., Tipa A., Castagnaro A., et al. Vascular endothelial growth factor up-regulation and bronchial wall remodeling in asthma. Clin Exp Allergy. 2005; 35(11):1437-42.
- Csete M. E., Chediak A. D., Abraham W. M., et al. Airway blood flow modifies allergic airway smooth muscle contraction. Am Rev Respir Dis. 1991;144(1):59-63.
- Fiedler U., Hellmut G., Augustin. Angiopoietins a link between angiogenesis and inflammation. Trends in Immunology. 2006;27(12)552-558.
- Gresele P., Dottorini M., Selli M. L., Iannacci L., Canino S., Todisco T., et al. Altered platelet function associated with the bronchial hyperresponsiveness accompanying nocturnal asthma. Journal of Allergy and Clinical Immunology. 1993;91:894-902.
- Li N., Hu H., Hjemdahl P. Aspirin treatment does not attenuate platelet or leukocyte activation as monitored by whole blood flow cytometry. Thromb Res. 2003;111:165–170.
- Storey R. F., Wilcox R. G., Heptinstall S. Comparison of the pharmacodynamic effects of the platelet ADP receptor antagonists clopidogrel and AR-C69931MX in patients with ischaemic heart disease. Platelets. 2002;13:407–413.
- Barua C. C., Gupta P. P., Patnaik G. K., Kulsrestha D. K., Dhavan B. K. Antianaphylactic and mast cell stabilizing activity of Shirish. Indian Vet Med.J. 1997;21;127-132.
- Tripathi S. N., Shukla P. Effect of histamine and lebbeck Benth on guinea pigs adrenal gland. Indian Journal of Experimental Biology. 1979;17:915-917.
- Tripathi P., Tripathi Y. B., Dey P. K et al. Release of catecholamines from the adrenal medulla by histamine and its prevention by Albizzia lebbek in guinea pigs. Indian Journal of Physiology and Pharmacology. 1983;27(2):176-178.
- Sharma O. D. Clinical and experimental studies on bronchial asthma (Tamaka shvasa) with special reference to its management with Albizzia lebbeck.
- Tripathi E. M., Sen P. C., Dus P. K. Studies on the mechanism of action of Albizzia lebbeck, an Indian indigenous drug used in the treatment of atopic allergy. Journal of Ethnopharmacology. 1979;1:385-396.
- Ring J., Kramer U., Beherendt H. Why are allergies increasing? Current Opinion in Immunol. 2001;13:701-708.
- Kambayashi T., Koretzky G. A. Proximal signalling events in FC,RI mediated mast cell activation. J. Allergy and Clinical Immunol. 2007;119:544-552.
- Wershil K., Wang Z. S., Gordon J. R., Galli S. J. Recruitment of neutrophils during IgE- dependent cutaneous late phase reactions in the mouse is mast cell-dependent. Partial inhibition of the reaction with antiserum against tumour necrosis factor-alpha. The J. Clinical Investigation. 199;87:446-453.
- Okayama Y., Ra C., Saito. Role of mast cells in airway remodelling. Current Opinion in Immunol. 2007;19:687-693.
- Ennis M.,Pearce F. L.,Weston M. Some studies on the release of histamine from mast cells stimulated with polylysine. British J. Pharmacol. 1980;70:329-334.
- Yazdanparast R & Ardestani A. In vitro antioxidant and free radical scavenging activity of Cyperus rotundus. J Med Food. 2007;10(4):667-74.
- Govindan S., Viswanathan S., Vijayasekaran V., Alagappan R. Further studies on the clinical efficacy of Solanum xanthocarpum and Solanum trilobatum in bronchial asthma. Phytother Res. 2004;18(10):805-9.
- de Boer D.,Christof J. Majoor, Cornelis van ‘t Veer, Elisabeth H.D. Bel, Tom van der Poll. Asthma and coagulation. Jornal of American Society; Blood.18 January. 2012;119:3236-3244.
- Jung S. H.,Kim S. J., Jun B. G., Lee K. T., Hong S. P., Oh M. S., Jang D. S., Choi J. H. α-Cyperone, isolated from the rhizomes of Cyperus rotundus, inhibits LPS-induced COX-2 expression and PGE2 production through the negative regulation of NFκB signalling in RAW 264.7 cells. J Ethnopharmacol. 2013;147(1):208-14.
CrossRef - Divya K., Tripathi J. S., Tiwari S. K., Pandey B. L. The analgesic and anti-inflammatory activities of the hydroalcholic extract of “Shirishadi compound” in animal model. Journal of Applied Pharmaceutical Science. 2011:01(10);98-101.

