
N. Nathiya1, K. Sasikumar2, M. Jagannath3, M. Thangaraj4 and K. Adalarasu5
1Division of Mathematics, School of Advanced Sciences, VIT University, Chennai, Tamilnadu, India.
2School of Electronics Engineering, VIT University, Vellore, Tamilnadu, India.
3School of Electronics Engineering, VIT University, Chennai, Tamilnadu, India.
4Department of Physiotherapy, ITS Paramedical College, Ghaziabad, Uttra Pradesh, India.
5School of Electrical and Electronics Engineering, Sastra University, Thanjavur, Tamilnadu, India.
Corresponding Author E-mail: sasikumar.k@vit.ac.in
DOI : https://dx.doi.org/10.13005/bpj/1182
Abstract
Community physiotherapists are under increasing pressure and managing their time for working with small amount of resources and management skills. This situation is very dangerous and due to the physical discomforts in the workplace the physiotherapists are experiencing the stress. This seems to be that the physiotherapists are in a specific risk themselves from physical work pressure that is the source of the musculoskeletal disorders (MSD). The aim of this study is concentrates the musculoskeletal injury for finding the occupational stress factors over sixty five physiotherapists in top ten hospitals using subjective scale study. Two groups were formed using the participants, i.e., physiotherapists from government hospital (GH) and physiotherapists from private hospital (PH). It is clearly stated that GH physiotherapists were in low risk compared to PH physiotherapists significantly (p < 0.05). This because of the communication between the personal factors and worst environmental factors created by patients strength, which is used to disturb the nature of care and working life.
Keywords
Occupational Stress; Musculoskeletal Disorders; Pain Score; Physiotherapist
Download this article as:| Copy the following to cite this article: Nathiya N, Sasikumar K, Jagannath M, Thangaraj M. Adalarasu K. An Observational Study on Occupational Stress Among Physiotherapists. Biomed Pharmacol J 2017;10(2). |
| Copy the following to cite this URL: Nathiya N, Sasikumar K, Jagannath M, Thangaraj M. Adalarasu K. An Observational Study on Occupational Stress Among Physiotherapists. Biomed Pharmacol J 2017;10(2). Available from: http://biomedpharmajournal.org/?p=15171 |
Introduction
Physiotherapy is seem to be a major health care profession that focuses to recognize the ability of people and also to develop the move and function [1,2]. Nowadays the major challenges in Asian countries are to develop the life quality of people by delivering the common health care. This is because of the greatest population and economic diversity. Medical field is always the emerging trend because of the low man power. For example in India, among the total population of about 1.21 billion the medical supplies, physicians as well as physiotherapists are deficient [3]. This is because the physiotherapists need to work more effectively with small amount of resources and handling ability.
The variety of works in physiotherapy include a lot of physical activity from positions to postures and this is sometimes not be ideal and it is dangerous to physiotherapists could place them in high risk of accidents and injuries. The wide variety of jobs are namely: pushing, pulling, lifting, stretching, reaching, lowering, standing, sitting, sitting, bending, walking and demonstrating. These jobs are seemed to be stressful due to the physical discomforts in the working environments. To some extent hence, the physiotherapists are in the major risk of physical strain that is the source of the musculoskeletal disorders (MSD) [4,5].
The MSD in physiotherapists is normally induced by the activities that are related patients, i.e., lifting combined with patient therapy. Global research proposes that physiotherapists are susceptible to work-related musculoskeletal issue due to the way of their work, which can be tedious and labor-intensive. The physiotherapists are under the age of 30 seem to be at higher risk, especially in the period of initial four or five years of practice, a specific concern in a National Health Service environment where there are maintenance issues among physiotherapists. Most physiotherapists sustaining work-related musculoskeletal disorders (WMSDs) are treated by themselves or taking treatment from a colleague comparatively meet the doctor or from occupational health departments [2].
A wide variety of research shows that the hospital ergonomics have been carried out to analyze which hospital administrators implement the developing ways for physiotherapists work with an adequate workload with great nature of care. The hospitalization ergonomics includes the connection of individual factors, for example fitness, fatigue, age and occurrence and environmental factors, i.e., plan, work institution, hospital layout, work, furniture, therapeutic resources and mental help inside the work group, which associated to lead to believe the nature and working status of life. Investigation of the cooperation of these components lead to strain of care-physical and cognitive and it is fundamental to enhance the occupied state of the physiotherapists [6].
The exercise and traction unit is seemed to be the popular shared workplace in physiotherapy clinics. A large number of various people should accommodate in these workplaces for any given period. The greatest hospitals passed the 60% of the work to young physiotherapists, because they are the one handles the patients and the equipment’s mostly [1,2]. This publicity includes a larger amount of physical workload this is evaluated over the investigation of stance, movement, and progressive load after some time or through the questionnaires that follows the indirect approach: agendas, or records.
Literature Survey
Work-related musculoskeletal disorders are considered as serious concern in health care professionals [7]. Among them, allied health professionals (AHPs) are essential providers of services for individuals who are sick or injured, or have a disability. AHPs include occupational groups, such as physiotherapists, occupational therapists, speech pathologists, prosthetists and orthotists, audiologists, radiologists, exercise physiologists, etc., that have similar job roles, levels of job fulfillment, and issues concerning work life balance and staff retention [8-14]. They carry out a variety of work doings and are exposed to a variety of hazards and risks related with a higher chance of WMSDs development. Factors such as failure to take rest breaks, insufficient staffing levels and a substantial caseload lead to the risk of WMSDs [15,16].
Glover [17] investigated musculoskeletal disorders that are related to neck and upper limb. This is seemed to be a significant obstacle among workers. The physiotherapists are susceptible to work-related musculoskeletal disorders. Cromie et al. [18] found that young physiotherapists at the age of 30 years reported significantly more work-related injury occurrence. Although nursing assistants and other caretakers are affected by the work-related musculoskeletal disorders in the healthcare service, physiotherapists also are affected to many of the occupational risk factors due to work-related musculoskeletal problems, specifically lower back. The incidence of low back pain among physiotherapists has been reported at the range of 57% lifetime occurrence [19,20]. Grobel [21] inspected psychosocial demands influencing salaried physiotherapists and their outcomes. The study found that the objective and enthusiastic requests of work had a tendency to be seen imperative and that occupation fulfillment was appraised as high.
There is only inadequate data available in the literature regarding the hazard factors for WMSDs in physiotherapists [22]. This paper aims at the analysis of occupational stress risk factors for both government hospital (GH) physiotherapists and private hospital (PH) physiotherapists. For this analysis, the interviewer-administered structured questionnaire was used to calculate the discomfort/pain occurred in job hours.
Methods and Materials
Participants
Totally there were 65 participants (45 male, 20 female) with the age group of 29.77±4.4 (years) and mean experience of 5.34±2.58 (years) used for analysis of this study. Among 65, thirty three were junior physiotherapists (JP); twenty four were senior physiotherapists (SP) and eight were therapy managers (TM). Participants were divided into two groups, i.e., Physiotherapists of GH (34) and Physiotherapists of PH (31). The details of the participants and the details of the hospitals were shown in Table I.
Table 1: Details of the Participants and the Name of the Hospitals (GH – Government Hospitals; PH – Private Hospitals; JP – Junior Physiotherapists; SP – Senior Physiotherapists; TM – Therapy Managers)
| Category | Hospitals | JP | SP | TM |
| GH | All India Institute of Medical Sciences, New Delhi | 5 | 3 | 2 |
| Government Vellore Medical College & Hospital, Vellore | 2 | 1 | 0 | |
| GB Pant Hospital, New Delhi | 5 | 4 | 2 | |
| Safdarjang Hospital, New Delhi | 4 | 2 | 0 | |
| Rajaji Government Hospital, Madurai | 2 | 2 | 0 | |
| PH | Vijaya Health Center, Chennai | 2 | 1 | 0 |
| Pushpanjali Crosslay Hospital, Vaishali, Ghaziabad | 3 | 3 | 2 | |
| Meenakchi Mission Hospital & Research Centre, Madurai | 2 | 2 | 0 | |
| Fortis Jessaram Hospital, New Delhi | 4 | 3 | 0 | |
| Max Super-Speciality Hospital, New Delhi | 4 | 3 | 2 |
Experimental Design
Initially the mini-mental state examination (MMSE) was taken. After that, this study is clearly clarified to the participants. All participants undergo a questionnaire study to enumerate the total observed discomfort/pain calculation at various areas of organs such as shoulder, thigh, neck, back, elbow, wrist/hand, knee, leg and ankle/feet (Fig. 1). This study mainly focuses on participants who encountering MSD, i.e., occurred because of their regular jobs itself. Table II shows that the pain-scale criteria and their equivalent grades.
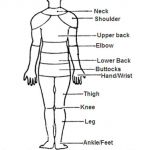 |
Figure 1: Observed discomfort related to work in different parts of the body.
|
Table 2: Criteria For Pain-Score and Their Grades
| Criteria for Pain-score | Grade |
| No pain, feeling perfectly normal | 0 |
| Mild pain, very barely noticeable | 1 |
| Minor pain, discomforting | 2 |
| Very noticeable pain, tolerable | 3 |
| Strong pain, distressing | 4 |
| Piercing pain, very distressing | 5 |
| Intense pain | 6 |
| Very intense pain | 7 |
| Utterly horrible | 8 |
| Excruciating unbearable | 9 |
| Unimaginable unspeakable | 10 |
Results and Discussion
The qualitative measure is observation of pain/discomfort and it is totally subjective. To screen the musculoskeletal disorders the methodologies that are based on the subjective scale tests including questionnaire studies were used.
The result of this study (Fig. 2) represents the PH observed discomfort in the upper extremities of the organ of physiotherapists of PH (shoulder, upper back, elbow and wrist/hand) and it was notably (p < 0.05) high when contrasted with GH physiotherapists. At the same time, observed pain in the regions like thigh, knee and ankle/feet was likewise (p < 0.05) pointedly greater in PH physiotherapists while comparing with GH physiotherapists.
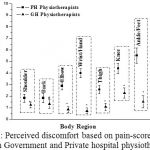 |
Figure 2: Perceived discomfort based on pain-score criteria Between Government and Private hospital physiotherapists.
|
This study focused a wide variety of physical demands for better understanding of various tasks that were carried out in hospitals. Some of the studies have focused the use of electro-goniometers and electromyography among the health care professionals and physiotherapists. For example: the hospital setting, due to the interruption of the work connected with attaching and determining devices seem to be difficult [6]. The questionnaire study that is related to psycho-physiological used for potential analysis is utilized in the hospital setting.
The pain occurred in the neck, shoulders and shoulder joints by raising, dynamic behavior and impact on the lower back [1]. The result stated that the high risk factors are occurred in PH physiotherapists while comparing to GH physiotherapists. Because of the free charge in GH higher amount of patients seek treatment from GH. Shannon et al. [23] propounded a method that examines the difference between the general health and time of occurrence of pain. The result of this method depicted that there is a significance increase in both time with neck and back pain and significant decrease in general health. Finally they conclude the changes that are predicted from these outcomes are work related elements, i.e., work psychological demands, job intervene with family, job influence and working hours [24]. The recent researchers highlighted the difficulties in hand, elbow and wrists. High threat employments include continual, forceful and repetitive actions, for example, with the hyperextension and hyperflexion, which eventually cause musculoskeletal disorders.
Our survey showed physiotherapists main problems in back, leg, heel, ankle, and foot pain due to standing and demonstrating long hours. The knees issues in physiotherapists also associated with the workload in long hours and extreme postures lifting loads.
The above explained problems can be prevented by the well-structured design of job and working place and locating the perfect tools or devices for that work. NIOSH prescribes the following rules for manual handling:
Limit the space between the body and the load
Lift loads from knuckle height
Keep the travel space for the lift to less than 10 feet
Limit twisting
Proper ergonomic design of workstation, and therapeutic equipment
Practicing the lifting and cleaning techniques
The controls in administration like staff handling, assigning more tasks, and giving breaks.
Conclusions
There are multiple musculoskeletal problems occurred in physiotherapists that uniquely affects their daily activities. From this study, we conclude that the PH physiotherapists experienced the majority discomfort/pain when compared to GH physiotherapists. This is due to the fact that the improper workflow of hospital management and the high admission rate of patients, work hours and the equipments mishandling. Practically the acceptance of suitable postures and practices are based on the working area and availability of appropriate tools.. Every hospital should have the plan of extensive ergonomic protocols and the fundamental resources to support the same. These factors can be used to improve the predictive measures of health care risks among physiotherapists.
Acknowledgment
Authors would like to express their special thanks of gratitude to the hospital administration for offering authorization to lead the study. We thank our participants who provided the great assistance and involvement throughout the study.
References
- Cromie, J., Robertson, V., and Best, M., Work-related musculo-skeletal disorders in physical therapists prevalence, severity, risks and responses. Physical Therapy, Vol. 80, 2000, pp. 336–351.
CrossRef - Dalton, M.B., Development of the assessment of physiotherapy practice – A standardized and validated approach to assessment of professional competence in physiotherapy. Doctor of Philosophy Thesis, 2011, Monash University, Melbourne. URL: http://arrow.monash.edu.au/hdl/1959.1/479140.
- Wells, R., Norman, R., Neumann, P., Andrews, D., Frank, J., Shannon, H., and Kerr, M., Assessment of physical work load in epidemiologic studies: common measurement metrics for exposure assessment. Ergonomics, Vol. 40, No. 1, pp. 51–61.
CrossRef - Brown, N.D., and Thomas, N.I., Exploring variables among medical center employees with injuries: developing interventions and strategies. AAOHN J, Vol. 51, No. 11, 2003, pp. 470–481.
- Marras, W.S., Davis, K.G., Kirking, B.C., and Bertsche, P.K., A comprehensive analysis of low-back disorder risk and spinal loading during the transferring and repositioning of patients using different techniques. Ergonomics, Vol. 42, No. 7, 1999, pp. 904–926.
CrossRef - Scholey M., and Hair M., Back pain in physiotherapists involved in back education. Ergonomics, Vol. 32, 1989, pp. 179–190.
CrossRef - Shannon, H.S., Woodward, C.A., Cunningham, C.E., McIntosh, J., Lendrum, B., Brown, J., and Rosenbloom, D., Changes in general health and musculoskeletal outcomes in the workforce of a hospital undergoing rapid change: A longitudinal study. Journal of Occupational Health Psychology, 6, No. 1, 2001, pp. 3–14.
CrossRef - Forde, M.S., Punnett, L. and Wegman, D.H., Pathomechanisms of work-related musculoskeletal disorders: conceptual issues, Ergonomics, Vol. 45, No. 9, 2002, pp. 619–630.
CrossRef - Safe Work Australia Compendium of Workers’ Compensation Statistics 2010–2011, 2013.
- Baldwin, A., Woods, K., and Copeland, M., Simmons Diversity of the allied health workforce: the unmet challenge. J Allied Health, Vol. 34, 2006, pp. 116–120.
- Colins, K., Jones, M., McDonnell, A., Read, S., Jones, R., and Cameron A., Do new roles contribute to job satisfaction and retention of staff in nursing and professions allied to medicine? J Nurs Manag, Vol. 8, 2000, pp. 3–12.
- Dodd, J., Saggers, S., and Wildy, H., Retention in the allied health workforce: boomers, generation X and generation Y. J Allied Health, Vol. 38, 2009, pp. 215–219.
- Lyons, K., Lapin, J., and Young, B., A study of job satisfaction of nursing and allied health graduates from a mid-Atlantic university. J Allied Health, Vol. 32, 2003, pp. 10–17.
- O’Toole, K., Schoo, A., and Hernan, A., Why did they leave and what can they tell us? Allied health professionals leaving rural settings. Aust Health Rev, Vol. 34, 2010, pp. 66–72.
CrossRef - Stagnitti, K., Schoo, A., Dunbar, J., and Reid, C., An exploration of issues of management and intention to stay: allied health professionals in South West Victoria. Australia J Allied Health, Vol. 35, 2006, pp. 226–232.
- Wilson, N., Factors that affect job satisfaction and intention to leave of allied health professionals in a metropolitan hospital. Aust Health Rev, Vol. 39, 2015, pp. 290–294.
CrossRef - Dawson, A.P., McLennan, S.N., Schiller, S.D., Jull, G.A., Hodges, P.W., and Stewart, S., Interventions to prevent back pain and back injury in nurses: a systematic review. Occup Environ Med, 64, 2007, pp. 642–650.
CrossRef - Gropelli, T.M., and Corle, K., Nurses’ and therapists experiences with occupational musculoskeletal injuries. AAOHN J, Vol. 58, 2010, pp. 159–166.
CrossRef - Glover, W., Work-related strain injuries in physiotherapists: Prevalence and prevention of musculoskeletal disorders. Physiotherapy, 88, No. 6, 2002, pp. 364–372.
CrossRef - Cromie, J., Robertson, V., and Best, M., Work-related musculoskeletal disorders in physical therapists prevalence, severity, risks and responses. Physical Therapy, Vol. 80, 2000, pp. 336–351.
CrossRef - Manassa, P., Back pain incidence physiotherapists and nurses: A comparative study. Aust. J. Physiotherapy, Vol. 30, 1984, p. 100.
- Molumphy, M., Unger, B., Jensen, G.M., and Lopopolo, R.B., Incidence of work-related low back pain in physical therapists. Phys. Therapy, Vol. 65, 1985, pp. 482–486.
CrossRef - Grobel, S., (2008) Psychosoziale Belastungen von PhysiotherapeutInnen. Querschnittsstudie zur Arbeitsbelastung mittels des Copenhagen Psychosocial Questionnaire. pt Zeitschrift für Physiotherapeuten, Vol. 60, No. 10, 2008, pp. 1068–1087.
- Snodgrass, S.J., Rivett, D.A., Chiarelli, P., Bates, A.M., and Rowe, L.J., Factors related to thumb pain in physiotherapists. Australian Journal of Physiotherapy, Vol. 49, 2003, pp. 243–250.
CrossRef

