
Manuscript accepted on :February 24, 2017
Published online on: --
Plagiarism Check: Yes
Anvar Elyasi1,2, Marzieh Soheili2, Khosro Setayeshi2, Shirin Honarmand1 and Katayoun Derakhshandeh3,4
1Department of Surgery, Faculty of Medicine, Kurdistan University of Medical Sciences, Kurdistan, Iran.
2Department of Surgery, Faculty of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran.
3Department of Pharmaceutics, Faculty of Pharmacy, Hamedan University of Medical Sciences, Hamedan, Iran.
4Department of Pharmaceutics, Faculty of Pharmacy, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Corresponding Author E-mail: Kderakhshandeh@kums.ac.ir
DOI : https://dx.doi.org/10.13005/bpj/1096
Abstract
Peritoneal adhesions are pathological fibrotic bands developing after mesothelial damage which causes different problems in the patients. The aim of this study was to compare the anti-adhesion efficacy of a herbal structure made from Psylium seeds with a commercially available formulation named Pluronic both in the form of hydrogel in a rat cecum abrasion model. The rat model utilized a cecal abrasion and abdominal wall insult surgical protocol. Psylium hydrogel treatment was applied by syringe to coat both the cecal and the abdominal wall insults, while other animals were treated with Pluronic applied to the cecal injury. Control animals did not receive any treatment. Animals were sacrificed after 21 days of laparotomy and adhesion severity was quantitatively graded according to macromorphological characteristics. Histological analysis was also performed for all animals. Psylium treated animals showed significantly lower adhesion scores than other groups (P<0.05), while Pluronic did not demonstrate any noticeable results. In conclusion, Psylium hydrogel showed a significantly decreased adhesion score compared with the Pluronic and control groups. However, Psylium compared with all adhesion formulations and barriers offer natural structure as well as ease of application and ability to conform to complex tissue geometries that could provide surgeons with another prophylactic treatment for preventing abdominal adhesions.
Keywords
Peritoneal adhesion; Psylium hydrogel; herbal formulation
Download this article as:| Copy the following to cite this article: Elyasi A, Soheili M, Setayeshi K, Honarmand S, Derakhshandeh K. Adhesion Prevention by Peritoneal Administration of Herbal Hydrogel. Biomed Pharmacol J 2017;10(1). |
| Copy the following to cite this URL: Elyasi A, Soheili M, Setayeshi K, Honarmand S, Derakhshandeh K. Adhesion Prevention by Peritoneal Administration of Herbal Hydrogel. Biomed Pharmacol J 2017;10(1). Available from: http://biomedpharmajournal.org/?p=14071 |
Introduction
Abdominal adhesions are abnormal bands of tissues between structures and organs in abdomen following injury to the peritoneal surface. The most common cause of intra-abdominal adhesions estimated as high as 80%, is a history of previous abdominal surgery. The formation of intra-abdominal adhesions may result from surgery, trauma, intra-abdominal tissue ischemia or infection [1, 2]. Postsurgical adhesions severely affect the quality of life which can lead to small-bowel obstruction, difficulty in re-operative surgery, chronic abdominal and pelvic pain and female infertility [3]. Several therapeutic approaches have been evaluated to prevent or minimize the occurrence of adhesions. These include improved surgical techniques, using pharmacologic agents and special methods that provide a physical barrier for adhesion formation [4]. In the United States, more than 90% of patients undergoing abdominal surgery suffer from some forms of minimal to extreme adhesions. These adhesions are formed through prolonged inflammation of injured tissues, neovascularization and fibroblast in-growth leading to fibrous tissue formations [5].
The physical barriers for adhesion formation involve many different clinical products.
These products totally are divided into two categories: non-absorbable and absorbable. Preclude membranes are made of non-biodegradable polytetrafluoroethylene. Although they are highly effective in preventing adhesions over a long period after surgery, these membranes must be removed at a later time surgically.
Biodegradable barriers are being used as additional surgery for later removal especially that they can minimize patient discomfort and hospitalization costs. Seprafilm, also was approved for abdominal and gynecological surgeries which is a type of absorbable barrier film composed of un-crosslinked, carboxymethylcellulose/ sodium hyaluronate [6]. It is a kind of sealing barrier among damaged tissue sites for reducing the incidence of adhesion formation while it allows the damaged tissues to be repaired under the barrier. However, they can be used limitedly for open surgical procedures because these films are fragile and difficult to apply as they aggressively adhere to any moisture on the surgeon’s gloves during placement [7]. Barrier devices such as polymer solutions, solid membranes, pre-formed or in situ cross linkable hydrogels have been tested in different forms. Solutions mostly are consisted of viscous polysaccharides which are applied by a variety of methods like spraying or pouring at the end of the surgical procedure [1].
The purpose of this study was a comparative evaluation between the anti-adhesion efficacies of psylium and poloxamer (pluronic F 68), both in the shape of hydrogel in a 21 day, rat cecum abrasion model.
Psyllium is found in the seed of plants of the Plantago genus, which has 200 species widely distributed. The gel-forming properties are critical for the application of Psyllium in different areas being highly related to its health benefits such as cholesterol-lowering, bowel regulating capacity and anti-inflammation capacity. It is also an effective dietary fiber for regulating the function of colon due to the high viscosity of Psyllium maintained in the intestine [8].
Pluronic is a triblock PEO-PPO-PEO copolymer with prominent gelatin properties that are useful as biocompatible materials for biomedical and personal care applications [9, 10]. It is also known under non-proprietary name “Poloxamers” and the trade name “BASF” in different types like Pluronic F127 and F68. These polymers are considerably used in drug delivery systems and polymer-based nanotechnology such as cancer chemotherapy, anti microbial and anti fungal treatments [11].
In this research the comparison between Psylium and Pluronic, allowed us to assess the adhesion prevention quality of these easy appliable hydrogels against the current and proven standards which still have some problems during the procedure of surgery.
Materials and Methods
Animal Preparation
A group of 54 Wistar-Albino rats, weighing 120-180 grams were purchased from Pasteur institute of Iran, keeping under standard laboratory conditions. During the whole time of the study, they were fed by carrot and special foods for rats as well as were supplied water. For the main phase which was different from the pilot phase, they were separated into 5 groups according to treatment. Each group consisted of 12 rats.
Pilot Study
In order to find the best concentration of Psylium and Pluronic hydrogels for performing the initial operation we had the pilot phase. For this step, 7 groups of rats (each group consisiting of 2 rats) were undergone the surgery:
Group 1: Adhesion induction and intraperitoneal administration of 2 ml of placebo.
Group 2: Adhesion induction and intraperitoneal administration of 2 ml of Psylium 1%.
Group 3: Adhesion induction and intraperitoneal administration of 2 ml of Psylium 2%.
Group 4: Adhesion induction and intraperitoneal administration of 2 ml of Psylium 3%.
Group 5: Adhesion induction and intraperitoneal administration of 2 ml of Pluronic 1%.
Group 6: Adhesion induction and intraperitoneal administration of 2 ml of Pluronic 2%
Group 7: Adhesion induction and intraperitoneal administration of 2 ml of Pluronic 3%
It is necessary to mention that the placebo in our study was the same solvent used for preparing hydrogels which was sterile distilled water. Also because of extra adhesiveness of the concentrations more than 3% for both hydrogels, using higher concentrations was not possible. Following this phase, the suitable concentrations involving 2% and 3% of each hydrogels, were selected on the basis of macroscopic and microscopic evaluations. So for following the project, groups 2 and 5 were omitted and the study was performed with the final groups as below:
Group 1: Adhesion induction and intraperitoneal administration of 2 ml of placebo.
Group 2: Adhesion induction and intraperitoneal administration of 2 ml of Psylium 2%.
Group 3: Adhesion induction and intraperitoneal administration of 2 ml of Psylium 3%.
Group 4: Adhesion induction and intraperitoneal administration of 2 ml of Pluronic 2%.
Group 5: Adhesion induction and intraperitoneal administration of 2 ml of Pluronic 3%.
Initial Operation in All Groups
General anesthesia was induced by an intramuscular injection of 40 mg/kg ketamine (Rotexmedica, Trittau, Germany) [12]. Preoperatively, the abdomen was shaved, scrubbed, and draped for sterile surgery. Following laparatomy via a 4 cm midline incision, adhesion formation model demonstrated by Hemadeh et al [13] was used. As described by them, a gauze sponge was rubbed on the serosa of the cecum until the serosal shine was lost and splitting hemorrhages were formed. Then the cecum and bowel were repositioned into the abdominal cavity. An intracutaneous running suture was performed using round chromic 3/0 to close the muscle wall. And cut nylon 3/0 was used to close the skin. In group 1, the abdomen was closed after using 2 cc of placebo. For group 2, 2 cc Psylium 2% and in group 3, 2 cc Psylium 3% was used. In group 4, 2cc Pluronic 2% and for group 5, 2cc Pluronic 3% was applied intraperitonealy. All hydrogels were sterilized in an autoclave before use.
Relaparotomy and Macroscopic Evaluation of Adhesion Formation
After 21 days all animals had to undergo for relaparotomy. Systemic anesthesia was induced through breathing ether. A second laparotomy was performed next to the first one. Adhesion formation was explored and evaluated macroscopically. The adhesions were graded by one of the authors who was blinded to the group assignment. The adhesions were scored using the classification reported by Nair et al [14] (Table 1).
Table 1: Scoring system for intraperitoneal adhesions
| Grade | Description of adhesive bands | Remarks |
| 0 | Complete absence of adhesions | Unsubstantial adhesions |
| 1 | Only one band of adhesions among visceras or between one viscera and the abdominal wall | |
| 2 | Two bands: among visceras or from viscera to abdominal wall | Substantial adhesions |
| 3 | More than two bands: among visceras or from viscera to the abdominal wall or all intestine making a mass without adhesion to the abdominal wall | |
| 4 | Viscera adhered directly to the abdominal wall, independent of the number and the extension of adhesion bands |
Histologic Examination
Adhesion-carrying tissues were excised en-bloc and fixed in formaldehyde solution. Following dehydration and paraffinization, sections with a thickness of 5 mm were stained with hematoxylin–eosin. Then the samples were examined under a light microscope. Inflammation, vascularization and fibrosis in granulation sites were graded in all samples. The histopathological evaluation of the specimens was performed by a pathologist blinded to the groups.
Statistics
Data collected on each of 5 groups in the efficacy study were analyzed using Fisher’s exact test and Chi-squared test (X2). This analysis indicated that one of the treatment means were significantly different
Results and Discussion
All animals were in a good health situation during the follow-up period, except for 4 rats that did not recover and died, before going for relaparotomy without developing small bowel obstruction. One animal from Group 1 died during anesthetic induction, and one animal from Groups 3, 4 and 5 died on the first postoperative day. None of the animals showed any signs of incompatibility or other local or systemic reactions after laparotomy. Psylium and Pluronic gels were well tolerated by all animals in the treatment group. No abnormalities of the liver or spleen were noticed in the rats receiving the treating agents. In macroscopic evaluation, the distribution of animals according to adhesions, mean adhesion scores and standard deviations of the groups are presented in Tables 2, 3 and 4, respectively.
for a particular outcome. P-values<0.05 were considered statistically significant.
Table 2: The distribution of rats according to the adhesion scores
| Adhesion score | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 |
| Control | Psylium 2% | Psylium 3% | Pluronic 2% | Pluronic 3% | |
| 0 | 0 | 3 | 8 | 0 | 0 |
| 1 | 0 | 2 | 2 | 0 | 0 |
| 2 | 0 | 5 | 1 | 5 | 3 |
| 3 | 5 | 2 | 1 | 6 | 7 |
| 4 | 7 | 0 | 0 | 1 | 2 |
Table 3: Adhesion scores of each group (percentage)
| outcome | Total | ||||
|
Polymer |
No adhesion | grade 1 and more | |||
| Psylium 3% | Count | 8 | 4 | 12 | |
| % within polymer | 66.7% | 33.3% | 100.0% | ||
| Psylium 2% | Count | 3 | 9 | 12 | |
| % within polymer | 0.25% | 0.75% | 100.0% | ||
| Pluronic 3% | Count | 0 | 12 | 12 | |
| % within polymer | 0% | 100% | 100.0% | ||
| Pluronic 2% | Count | 0 | 12 | 12 | |
| % within polymer | 0% | 100% | 100.0% | ||
| Control | Count | 0 | 12 | 12 | |
| % within polymer | .0% | 100.0% | 100.0% | ||
| Total | Count | 12 | 48 | 60 | |
| % within polymer | 20% | 80% | 100.0% | ||
Table 4: Adhesion scores of each group (p-value, mean and SD)
| Groups | No adhesion | p-value | Adhesion score (Mean±SD) |
| Psylium 3% | 66.7 | 0.005 | 1.75±0.95 |
| Psylium 2% | 0.25 | 0.046 | 2.00±0.70 |
| Pluronic 3% | 0 | 1.000 | 2.91±0.66 |
| Pluronic 2% | 0 | 1.000 | 2.66±0.65 |
| Control | 0 | 1.000 | 3.57±0.46 |
The adhesion scores of Group 3 were significantly lower compared to the other groups (p-value=0.005) (Fig 1, 2 and 3).
 |
Figure 1: Relaparotomy, Psylium 3%, adhesion score: 0 |
 |
Figure 2: Relaparotomy, Control, adhesion score: 4 |
 |
Figure 3: Relaparotomy, Pluronic 3%, adhesion score: 2 |
In pathologic examination, the specimens of animals which underwent Psylium 3% application, (Groups 3) revealed that neovascularization, inflammation and fibrosis were all significantly lower than the other groups. These findings suggest that in addition to other properties as a herbal therapeutic agent, Psylium can prevent adhesions through inhibition of inflammation and scarring as well as regulation of angiogenesis (fig 4 and 5).
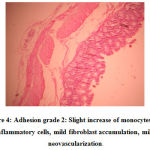 |
Figure 4: Adhesion grade 2: Slight increase of monocytes and inflammatory cells, mild fibroblast accumulation,mild neovascularization. |
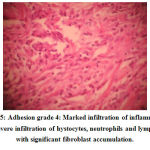 |
Figure 5: Adhesion grade 4: Marked infiltration of inflammatory cells, , severe infiltration of hystocytes, neutrophils and lymphocytes with significant fibroblast accumulation. |
Gomez-Gil et al in 2009 reported that about animals undergoing adhesionlysis, mesh areas covered by adhesions were significantly decreased at each follow-up time and mesothelialization was found in affected areas. During the first 3 days increased transforming growth factor (TGF)-b1 expression was detected. And in the next 7 days greatest TGF-b1 and vascular endothelial growth factor (VEGF) protein expressions were investigated, whereas genetic overexpression was observed at 14 days. The peak of active inflammatory cells was at the 7-day time point. So they concluded that adhesions formed at 3 days which can be considered as a critical time. Therefore an adhesionlysis was effective in preventing reformation of future adhesions [15].
In our research, the rats were sacrificed 21 days after surgery to evaluate the adhesion severity. In many comparable rat cecum abrasion models, the typical range of post-operative time for sacrificing in a solid or hydrogel barrier appliance is 7-14 days [16, 17]. Several studies have established that an adhesion barrier can be effective between 12 and 36 hours after surgery [18]. Since the post-surgical manifestations of adhesions are within the first few days, 5-7 days after surgery, the adhesion fibrosis becomes more organized, vascular and rigid [19, 20]. Any adhesions present in the abdominal cavity after 7 days could persist for several months depending on the effects of remodeling inside the adhesion tissue [19].
The cascade of intra-abdominal adhesion formation begins through an increase in vascular permeability and secretion of fibrin-rich exudates which are stimulated by peritoneal injury. Under normal conditions, the fibrin formation due to these reactions undergoes lysis by the peritoneal mesothelial plasminogen activator. Because of surgical trauma, ischemia or inflammation these physiologic properties of mesothelial cells are impaired. Moreover, the fibroblasts, mesothelial, endothelial and inflammatory cells produce plasminogen-activator inhibitor-1 and 2 which is the result of peritoneal injury. So adhesion formation can be facilitated by further decreasing plasminogen-activator activity (PAA). Normally, fibrinolytic activity occurs and fibroblast proliferation results in remesothelization. But in ischemic conditions like surgical trauma, fibrinolytic activity is suppressed and fibrin remains in the environment. Since PAA in fibroblasts is regulated by oxygen, creation of a hypoxic state markedly attenuates PAA, which leads to adhesion development. Once the fibrin bands are infiltrated with fibroblasts, they become organized into adhesions [21, 22].
The purpose of lots of studies was preventing adhesions by focusing on various steps of this physiopathologic process. Antioxidants, anti-inflammatory agents and biologic physical barriers have been used to overcome these side effects. Sodium citrate, heparin, and other anticoagulants as well as a variety of fibrinolitic agents and salts such as sodium risonilate, and mechanical peritoneal lavage have been used for preventing the accumulation of fibrin from peritoneal exudate. It has been found that increasing the incidence of ileus condition intensifies the adhesion development [23, 24, 25, 26].
Overall, the Psylium hydrogel showed a significant decrease in adhesion comparing to the other animals receiving no hydrogel or pluronic intervention. Approximately eight out of twelve Psylium treated animals displayed adhesions with scores of 0, having no adhered tissue present in the abdomen and 2 of them with grade 1 having filmy adhesions that were easily lysed. Only one animal presented a severe adhesion (grade 3) during the 21 days post treatment period. There are some possible causes explaining this adhesion such as fracture of the hydrogel at or in proximity of the injured surfaces or insufficient coverage over the injured tissues.
Psylium has many characteristics which make it potentially suitable in the prevention of peritoneal adhesions. In our study the animals were sacrificed on day 21 and the histological result of Psylium 3% in integration with the adjoining tissue at the insulted area after these 21 days did not show cellular infiltration into the bulk of the material, suggesting the hydrogel may be degraded through surface erosion. The obvious absence of cellular infiltration suggested that the hydrogel functioned as an effective, occlusive barrier for preventing inflammatory and fibroblast cells from synthesizing aggressive tissue adhesions between the injured cecum and the abdominal wall.
Lang et al in 2009 investigated that adhesion re-formation after relaparotomy decreases significantly through the use of PVA-gel. They also accept ultrasound as a noninvasive technique of adhesion detection is a sufficient and reliable method for detecting adhesion formations [12]. Leach et al in 1990 performed a study on the effect of poloxamer 407 in the rat uterine horn model which is in the early clinical development phase. Twenty-two rats underwent bilateral surgical injury to the uterine horn and the parietal peritoneum. A random side was treated with a 30% solution of poloxamer 407. Twenty-one days later the animals were sacrificed and evaluated for the presence of adhesions. They reported a highly significant reduction in adhesion formation on the treated side [27]. Anyway, both solid and liquid barriers can prevent adhesions. Although they are suitable for adhesion prevention after multifocal trauma, further testing in the everyday clinical situation seems necessary [28]. Dunn et al in a study on a rat model, found that SprayGel can significantly reduce the incidence of adhesions, which formed in 7 of 8 control rats compared with 1 of 8 treated rats. Also on the rabbit model, they showed the role of SprayGel which could significantly reduce both the extent and severity of adhesions. But they expressed further investigation in large animal and clinical settings are warranted [29]. Yeo et al in 2006 studied the efficacy of an in situ cross-linked hyaluronic acid hydrogel (HAX) in preventing post-surgical peritoneal adhesions, in a rabbit cecum abrasion model. Ten out of 12 animals in the untreated control group developed fibrous adhesions in which sharp dissection was required. While only 2 out of 8 animals treated with HAX gel showed such adhesions which occurred in locations that were not covered by the hydrogel. It means that cross-linked HA hydrogels were highly effective to reduce the formation of intraperitoneal adhesions after surgery [30]. In 2005 and 2006, hyaluronate-carboxymethylcellulose (HA-CMC) barrier (Seprafilm) was applied to evaluate its efficacy on the prevention of pelvic adhesion formation in women undergoing radical hysterectomy as well as primary cytoreductive surgery with radical oophorectomy for locally advanced epithelial cancer. Those researches demonstrated that using a HA-CMC barrier led to a significant reduction in the extent and density of pelvic adhesion formation after the surgery [31, 32]. As mentioned before, transforming growth factor beta-1 (TGF-b1) has mitogenic activities for macrophages and fibroblasts. Overexpression of TGF-b1 results in the pathogenesis of several fibrotic disorders. Since Angiotensin II increases the expression of the TGF-b1 in fibroblasts, Bulbuller et al in 2004 evaluated the effects of lisinopril on the adhesion formation in rats following ileocecal anastomosis and investigated that ACE inhibitors in the form of oral use, might be useful for preventing peritoneal adhesions [33]. Kim et al have shown that Sunitinib, a VEGFR-2 antagonist, significantly reduces adhesion formation in a murine model. Antiangiogenic therapy may be an effective strategy for preventing or treating adhesions after intra-abdominal procedures [34]. In another study, some scientists compared the effects of diphenhydramine–HCl and a Na–hyaluronate derivative (seprafilm) on the development of postoperative peritoneal adhesion and tubal obstruction. They presented that both diphenhydramine and Seprafilm can significantly reduce postoperative peritoneal adhesion development allowing the uterine tubes to remain open [35]. About comparing Seprafilm with another agent, it should be mentioned that the intraperitoneal use of atorvastatin is as efficient as Seprafilm in inhibiting the formation of postoperative adhesions in rats. But there might be a great attention to the dose-dependent side effects of statins so that lower doses of atorvastatin should be included in future experiments [36]. Post operative peritoneal adhesion formation intensifies in mice receiving nicotine preoperatively. This study was done in 2006 which was investigative of a direct increase in peritoneal VEGF release and mesenteric endothelial permeability by nicotine. These findings could have important implications for smokers undergoing intra-abdominal surgical procedures [37]. Ignjatovic et al following their study in 2010 believe that a single dose of intraperitoneal bevacizumab can reduce grade and severity of abdominal adhesions in the cecum abrasion rat model. But they have considered findings for further studies on the mechanisms involved in adhesion prevention within the peritoneum [38]. In a study performed in 2014, the researchers tried to investigate the effect of misoprostol in the reduction of adhesion formation after gynecological surgery through a double blind, randomized controlled experimental study. Twenty-one rats were divided into three groups as control, misoprostol and Hyalobarrier groups. The injuries were made to the each uterine horn by cautery. After 14 days from the first surgical procedure, adhesion scores were evaluated. The total adhesion score values of the control group were statistically higher than the values of misoprostol and Hyalobarrier groups. The inflammation score value of misoprostol group was statistically lower than control and Hyalobarrier groups. So they found a new therapeutic potential usage of misoprostol that may be effective to prevent pelvic adhesion and reduce inflammation scores. [39]. In another research done in 2015, the scientists used intra-abdominal Sugammadex on adhesion formation after laparotomy. They observed that sugammadex could reduce adhesions in the rats. However, again a variety of clinical studies are still required for sugammadex to be applied for preventing postoperative peritoneal adhesion in humans [40]. Soluble Phosphatidylcholine as well as Ibuprofen administered intraperitoneally are other two agents which have been reported to be a potent adjunct in postoperative adhesion prevention [41]. As we know, there are some commercially available agents for adhesion prophylaxis. Rajab et al in 2008 compared the most four commonly used adhesion barriers against a control group in a clinically relevant rat model. The experimental lesions were treated with Seprafilm, Adept, Intercoat, Spraygel, or no barrier. The resulting adhesions were examined 14 days postoperatively. The mean area covered by adhesion was 77% in the control group, 68% in animals treated with Spraygel, 55% in animals treated with Intercoat, 54% in animals treated with Adept and 46% in animals treated with Seprafilm. They reported some statistically significant differences between the barriers with regards to the area covered by adhesions and the adhesion-free incidence. Following these results, they believe that a significant adhesion burden remains with all of the tested barriers [42]. In another comparative study, Ryan et al concluded that carboxymethylcellulose sponge was more effective than Interceed in preventing postoperative adhesions [43].
In conclusion this study showed that intraperitoneal Psylium treatment was effective in the prevention of peritoneal adhesion. The herbal structure of this treatment did not create any injurious effect. The technique of some barriers application is critical, which sometimes make the treatment difficult. Intraperitoneal Psylium was equally effective. Easy applicability and herbal nature was its major advantage. The hydrogel is easy to apply using a syringe and has achieved comparable, overall efficacy in adhesion prevention as other barriers. Future studies using larger animal models of abdominal adhesion as well as laparoscopic application of the hydrogel are needed to further establish efficacy in humans prior to clinical evaluation.
Acknowledgement
The authors would like to thank Dr Ahmad Framarzi and Miss Sedigheh Khazaee for their kind assistance with the histological examination. This work was supported financially by the faculty of medicine, University of Medical Sciences, Kermanshah, Iran.
References
- Yeo Y, Kohane D.S. Polymers in the prevention of peritoneal adhesions. Eur J Pharm Biopharm 2008;68:57-66.
- Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL. Peritoneal adhesions: etiology, pathophysiology, and clinical significance. Recent advances in prevention and management. Dig Surg 2001;18:260–73.
- Yetkin G, Uludag M, Citgez B, Karakoc S, Polat N, Kabukcuoglu F. Prevention of peritoneal adhesions by intraperitoneal administration of vitamin E and human amniotic membrane. Int J Surg 2009;7:561-565.
- Cashman J.D, Kennah E, Shuto A, Winternitz Ch, Christopher M. K. Springate Ch. M. K. Fucoidan Film Safely Inhibits Surgical Adhesions in a Rat Model. J Sur Res 2011;171(2):495-503.
- Ar’Rajab A, Mileski W, Sentementes JT, Sikes P, Harris R.B, Dawidson I.J. The role of neutrophils in peritoneal adhesion formation. J Surg Res 1996;61:143.
- Falabella Ch.A, Melendez M.M, Weng L, Chen W. Novel Macromolecular Crosslinking Hydrogel to Reduce Intra-Abdominal Adhesions. J Sur Res 2010;159:772-778.
- Gago LA, Saed GM, Chauhan S, et al. Seprafilm (modified hyaluronic acid and carboxymethylcellulose) acts as a physical barrier. Fertil Steril 2003;80:612.
- Guo Q, Cui S.W, Wang Q, Goff H.D, Alexandra Smith A. Microstructure and rheological properties of psyllium polysaccharide gel. Food Hydrocol 2009;23:1542–1547.
- Rapoport N. Stabilization and activation of Pluronic micelles for tumor-targeted drug delivery. Coll Surf, B: Biointerfaces 1999;16:93-111.
- Newby G.E, Hamley I.W, King S. M, Martin Ch.M, Terrill N.J. Structure, rheology and shear alignment of Pluronic block copolymer mixtures. J Coll Intface Sci 2009;329:54–61.
- Batrakova E.V, Kabanov A.V. Pluronic block copolymers: Evolution of drug delivery concept from inert nanocarriers to biological response modifiers. J Contd Rel 2008;130:98–106.
- Lang R.A, Weisgerber Ch, Grüntzig P.M, Christine Weis Ch, Odermatt E.K, Kirschner M.H. Polyvinyl Alcohol Gel Prevents Adhesion Re-Formation After Adhesiolysis in a Rabbit Model. J Sur 2009;153:12–16.
- Hemadeh O, Chilukuri S, Bonet V, Hussein S, Chaudry IH. Prevention of peritoneal adhesions by administration of sodium carboxymethyl cellulose and oral vitamin E. Surgery 1993;114:907–10.
- Nair SK, Bhat IK, Aurora AL. Role of proteolytic enzyme in the prevention of postoperative intraperitoneal adhesions. Arch Surg 1974;108:849–53.
- Veronica Gomez-Gil V.G, Garcia-Honduvilla N, Pascual G, Rodriguez M, Bujan J, Bellon J.M. Peritoneal adhesion formation and reformation tracked by sequential laparoscopy: Optimizing the time point for adhesiolysis. Surgery 2010;147:378-91.
- Arnold PB, Green CW, Foresman PA, et al. Evaluation of resorbable barriers for preventing surgical adhesions. Fertil Steril 2000;73:157.
- Dunn R, Lyman MD, Edelman PG, et al. Evaluation of the SprayGel adhesion barrier in the rat cecum abrasion and rabbit uterine horn adhesion models. Fertil Steril 2001;75:411.
- diZerega GCJD. Peritoneal repair and post-surgical adhesion formation. Human Reproduction Update 2001;7:547-555.
- Boland GM, Weigel RJ. Formation and prevention of postoperative abdominal adhesions. J Surg Res 2006;132:3.
- Liakakos T, Thomakos N, Fine PM, et al. Peritoneal adhesions: Etiology, pathophysiology, and clinical significance. Recent advances in prevention and management. Dig Surg 2001;18:260.
- Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL. Peritoneal adhesions: etiology, pathophysiology, and clinical significance. Recent advances in prevention and management. Dig Surg 2001;18:260–73.
- Saed Gh.M, Diamond M.P. Modulation of the expression of tissue plasminogen activator and its inhibitor by hypoxia in human peritoneal and adhesion fibroblasts. Fertil Steril 2003;79(1):164-168.
- Ouaissi M, Gaujoux S, Veyrie N, Dene`ve E, Brigand C, Castel B, et al. Post-operative adhesions after digestive surgery: their incidence and prevention: review of the literature. J Visc Surg 2012;149:e104-14.
- Jackson EK. Intraperitoneal administration of adenosine inhibits formation of abdominal adhesions. Dis Colon Rectum 2004;47:1390–6.
- Su SH, Nguyen KT, Satasiya P, Greilich PE, Tang L, Eberhart RC. Curcumin impregnation improves the mechanical properties and reduces the inflammatory response associated with poly(L-lactic acid) fiber. J Biomater Sci Polym Ed 2005;16:353–70.
- Avital S, Bollinger TJ, Wilkinson JD, Marchetti F, Hellinger MD, Sands LR. Preventing intra-abdominal adhesions with polylactic acid film: an animal study. Dis Colon Rectum 2005;48:153–7.
- Leach R.E, Henry R.L. Reduction of postoperative adhesions in the rat uterine horn model with poloxamer 407. Am J Obstet Gynecol 1990 May;162(5):1317-9.
- Wallwiener Cand M, Sara Brucker S, Hierlemann H, Brochhausen Ch, Solomayer E, Wallwiener Cand Ch. Innovative barriers for peritoneal adhesion prevention: liquid or solid? A rat uterine horn model.Ferti Steril 2006;86(4):1266-1276.
- Dunn R, Lyman M.D, Edelman P.G, Campbell P.K. Evaluation of the SprayGel™ adhesion barrier in the rat cecum abrasion and rabbit uterine horn adhesion models. Fertil Steril 2001;75(2):411-416.
- Yeo Y, Highley Ch.B, Bellas E, Ito T, Marini R, Langer R, Kohane D.S. In situ cross linkable hyaluronic acid hydrogels prevent post-operative abdominal adhesions in a rabbit model. Biomaterials 2006;27:4698–4705.
- Bristow R.E, Montz F.J. Prevention of adhesion formation after radical oophorectomy using a sodium hyaluronate-carboxymethylcellulose (HA-CMC) barrier. Gynecol Oncol 2005;99:301 – 308.
- Bristow R.E, Santillan A, Diaz-Montes T.P, Gardner G.J, Giuntoli II R.L, Peeler S.T. Prevention of adhesion formation after radical hysterectomy using a sodium hyaluronate carboxymethylcellulose (HA–CMC) barrier: A cost-effectiveness analysis. Gynecol Oncol 2007;104:739–746.
- Bulbuller N, Ilhan Y.S, Kirkil C, Cetiner M, Gogebakan O, Ilhan N. Can Angiotensin Converting Enzyme Inhibitors Prevent Postoperative Adhesions? J Surg Res 2005;125:94–97.
- Kim S, Lee S, Greene A.K, Arsenault D.A, Le H, Meisel J, Novak K, Flynn E, Heymach J.V, Puder M. Inhibition of Intra-Abdominal Adhesion Formation With the Angiogenesis Inhibitor Sunitinib. J Surg Res 2008;149:115–119.
- Avsar A.F, Avsar F.M, Sahin M,Topaloglu S, Vatansev H, Belviranli M. Diphenhydramine and hyaluronic acid derivatives reduce adnexal adhesions and prevent tubal obstructions in rats. Eur J Obst Gynecol Reproduct Biol 2003;106:50–54.
- Lalountas M.A, Ballas K.D, Skouras Ch, Asteriou Ch, Kontoulis Th, Pissas D, Triantafyllou A, Sakantamis A.K. Preventing intraperitoneal adhesions with atorvastatin and sodium hyaluronate/carboxymethylcellulose: a comparative study in rats. Amr J Surg 2010;200:118–123.
- Condon E.T, Cahill R.A, O’Malley D.B, Aherne N.J, Redmond H.P. Evaluation of Postoperative Peritoneal Adhesion Formation Following Perioperative Nicotine Administration. J Surg Res 2007;140:135–138.
- Ignjatovic D, Aasland K, Pettersen M, Sund S, Chen Y, Spasojevic M, Nesgaard J.M. Intra abdominal administration of bevacizumab diminishes intra-peritoneal adhesions. Amr J Surg 2010;200(2):270-275.
- Kaya C, Sever N, Cengiz H, Yıldız Ş , Ekin M, Yaşa L. A randomized controlled study of the efficacy of misoprostol and hyaluronic acid in preventing adhesion formation after gynecological surgery: a rat uterine horn model. Europ J of Obst & Gyn and Rep Bio 2014;176:44-49.
- Şahin H, Toman H, Kiraz H.A, ŞimŞek T, EbaŞ M, ozkul F, Arik M.K, Hanci V. Effects of sugammadex on the prevention of postoperative peritoneal adhesions. Kaohsiung Journal of Medical Sciences 2015;31:463-467.
- Nishimura K, Nakamur R.M, DiZerega G.S. Ibuprofen inhibition of postsurgical adhesion formation: A time and dose response biochemical evaluation in rabbits. J Surg Res 1984;36(2):115-124.
- Rajab T.K, Wallwiener M, Planck C, Brochhausen Ch, Kraemer B, Wallwiener Ch.W. A Direct Comparison of Seprafilm, Adept, Intercoat, and Spraygel for Adhesion Prophylaxis. J Surg Res 2010;161(2):246-249.
- Ryan Ch.K, Sax H.C. Evaluation of a carboxymethylcellulose sponge for prevention of postoperative adhesions. Amr J Surg 1995;169(1):154-160.

