
Manuscript accepted on :25-01-2026
Published online on: 26-02-2026
Plagiarism Check: Yes
Reviewed by: Dr. Dunya Abdal-Malik
Second Review by: Dr. Ahmed Luay Osman Hashim
Final Approval by: Dr. Patorn Piromchai
Hind Haidar Ahmed1* , Israa Elshayeb Ali Mohamed1, Mutaz Fathelrahman Saad1, Samar Mohammed Saeed1, Wafaa Mohammed Abdalla1, Ahmed Bakheet Abd Alla2, May Mohamed Ali3, Tagwa Salah Ahmed2, 4and Mohammed Siddig Abd Elaziz5
, Israa Elshayeb Ali Mohamed1, Mutaz Fathelrahman Saad1, Samar Mohammed Saeed1, Wafaa Mohammed Abdalla1, Ahmed Bakheet Abd Alla2, May Mohamed Ali3, Tagwa Salah Ahmed2, 4and Mohammed Siddig Abd Elaziz5
1Department of Microbiology, College of Medical Laboratory Science , Sudan University of Science and Technology, Khartoum – Sudan.
2Department of Parasitology and Medical Entomology, College of Medical Laboratory Science, Sudan University of Science and Technology, Khartoum – Sudan.
3Department of Hematology and Immunohematology, College of Medical Laboratory Science, Sudan University of Science and Technology, Khartoum, Sudan
4Department of Clinical Laboratory Science, College of Applied Medical Science, Jouf University, Saudi Arabia.
5Department of Histopathology and Cytology, College of Medical Laboratory Science, Sudan University of Science and Technology, Khartoum, Sudan
Corresponding Author E-mail:Hindhaidar011@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/3374
Abstract
Gastritis is one of the most common gastrointestinal issues worldwide. Helicobacter pylori (H. pylori) unequivocally causes both acute and chronic gastritis. The Epstein-Barr virus (EBV) is also one of the most prevalent viruses globally, affecting nearly everyone at some point in their lives. However, the co-infection of EBV and H. pylori remains poorly understood in African countries. This study aimed to investigate the presence of H. pylori and EBV among Sudanese patients with gastritis. One hundred (n=100) gastric biopsy samples were collected from patients undergoing upper gastrointestinal endoscopy at Police Hospital in Khartoum State, Sudan, from January 2019 to February 2020. DNA was extracted using the guanidine chloride method and detected by conventional PCR for EBV (EBNA-4) and H. pylori (16S rRNA) genes. Data analysis was conducted using SPSS version 26. Among gastric patients, 61 (61%) were males, and 39 (39%) were females. The prevalence of EBV was 17% (95% CI: 10.2-26.1%), with a significant association found in males (88.2% vs. 11.8%, p. value= 0.012). The prevalence of H. pylori was 34% (95% CI: 24.9–44.3) with no association with gender (p. value > 0.05). The co-infection rate of EBV and H. pylori was 7% (95% CI: 2.9–13.9), with no statistically significant difference observed (OR = 1.32; p. value = 0.493; 95% CI: 0.48–3.62). The prevalence of EBV and EBV/H. pylori co-infection in patients with gastritis in Sudan is low. EBV is more commonly associated with males. These findings underscore the need for further research on EBV's role in gastritis, particularly in endemic regions, and consideration of sex-stratified approaches.
Keywords
Co-infection , EBV ,Gastritis, H. pylori, PCR, Prevalence, Sudan
Download this article as:| Copy the following to cite this article: Ahmed H. H, Mohamed I. E. A, Saad M. F, Saeed S. M, Abdalla W. M, Alla A. B. A, Ali M. M, Ahmed T. S, Elaziz M. S. A. Molecular Detection of Helicobacter pylori and Epstein-Barr Virus Co-infection among Sudanese Gastritis Patients, Khartoum State- Sudan. Biomed Pharmacol J 2026;19(1). |
| Copy the following to cite this URL: Ahmed H. H, Mohamed I. E. A, Saad M. F, Saeed S. M, Abdalla W. M, Alla A. B. A, Ali M. M, Ahmed T. S, Elaziz M. S. A. Molecular Detection of Helicobacter pylori and Epstein-Barr Virus Co-infection among Sudanese Gastritis Patients, Khartoum State- Sudan. Biomed Pharmacol J 2026;19(1). Available from: https://bit.ly/4tMYlzU |
Introduction
Gastritis is a condition in which the stomach lining mucosa becomes inflamed, swollen, irritated, or eroded. It can develop gradually over time (chronic) or abruptly (acute). 1 It is one of the most common disorders in many cultures. 2 There are several etiological reasons for acute and chronic gastritis, including H. pylori infection, excessive alcohol intake, and others. Although H. pylori infection is common worldwide, its frequency varies significantly between countries and within specific populations within a single country. Despite a large number of people worldwide infected with H. pylori, infection rates can differ considerably within a single city and among various subgroups in a community.3,4 Obesity (those with a high BMI), drug use, smoking, and other risk factors for H. pylori .5
Epstein- Barr Virus (EBV) is one of the most prevalent human viruses, with 90% of cases occurring worldwide. 6, It can enter the body through the oropharyngeal epithelium and primarily spreads through bodily fluids, especially saliva 6, 8, 9
EBV can cause infectious mononucleosis, also known as “kissing sickness,” as well as other disorders. Its infection normally occurs in childhood, and most people experience relatively moderate or no symptoms. Long-term EBV infection may raise the chance of developing certain malignancies in some individuals. 6, 9, 10, 11 This study aims to enhance the understanding of EBV-H. pylori co-infection among Sudanese patients with gastritis, highlighting associated risk factors and potential health implications.
Materials and methods
In this descriptive cross-sectional study, one hundred gastric biopsy samples (n=100) were collected from the Endoscopy Department of Police Hospital in Khartoum State, Sudan, between January 2019 and February 2020. The samples were placed in Brain Heart Infusion Broth (BHIB) culture medium. DNA extraction and conventional polymerase chain reaction (PCR) were performed to detect the presence of H. pylori and EBV genes.
Ethical consideration
The Ethics Committee of Sudan University of Science and Technology’s College of Medical Laboratory Science provided ethical approval (SUST-CML-01-19). The study objectives and the method for collecting stomach biopsy samples were explained to participants before upper endoscopy procedures.
Before participation in the study, informed consent was obtained from all participants. They were fully informed of the study’s objectives, purpose, and possible implications. Participants were informed about the measures taken to ensure their confidentiality (of their personal information and the anonymization of any data collected to protect their identities) during the research.
DNA extraction
DNA was extracted from gastric biopsy material using the guanidine chloride method. After centrifuging each sample container for 15-20 min. at 3000 rpm, the pellet was removed and washed twice with PBS (phosphate-buffered saline). After adding 300 µL of ammonium (NH4) acetate, 10 µL of proteinase K, 1 ml of guanidine chloride, lysis buffer (2 ml ), the pellet was vortexed and incubated for 2 hrs. at 65˚C or overnight at 37˚C. Two ml of refrigerated chloroform was added, vortexed, then centrifuged for 5 min. at 3000 rpm. Once the mixture had cooled to room temperature, 10 ml of cold 100% ethanol were added to the mixture after the upper layer was transferred to another tube. After that, it was agitated and stored at -20°C for 2 hrs. or overnight for 15-20 minutes, the tube was centrifuged at 3000 rpm. After carefully discarding the supernatant, the tube was turned upside down onto tissue paper for 5 min. Four ml of 70% ethanol were used to rinse the pellet before it was centrifuged for 5 min. at 3000 rpm. After the supernatant was drained, the particle was left to dry for 10 min. 12
EBV EBNA-4 gene amplification by Conventional polymerase chain reaction (PCR)
A PCR primer specific to EBV nuclear antigen-4 (EBNA-4) was used for detecting EBV DNA, F: 5′GAGGAGGAAGACAAGAGTGG 3′ and R: 5′ GATTCAGGCGTGGT CCTTGG 3′ (Ahmed et al., 2015). The reaction products were estimated to be 938 bp in size. A PCR was performed using 1.5 µL of genomic DNA template to amplify the EBNA-4 gene of EBV in a total volume of 25 µL. 1 µL of 10 mMdNTP mixture (2.5 dATP, 2.5 mMdGTP, 2.5 mMdCTP, and 2.5 mMdTTP), 1.5 µL of 25 mM MgCl2, 2.5 µL of 10 PCR buffer (10 mMTrisHCl [pH 8.3], 50 mMKCl), 1µL Taq polymerase (about 1 U), 1.5 µL forward primer, and 1.5 µL reverse primer. The volume of each reaction was increased to 25 µL using twice D.W (ddH2O). To amplify the EBV EBNA-4 gene in 30 cycles, the following conditions were used: 5 minutes of initial denaturation at 94°C, 30 seconds of denaturation at 94°C for each cycle, 30 seconds of primers annealing at 55°C, 90 seconds of primers extension at 72°C, and final extension at 72°C for 5 minutes. Electrophoresis on a 1% agarose gel was performed to detect PCR products. 13
H. pylori (16srRNA) gene amplification by Conventional PCR
By selecting a primer that was specific to H. pylori (16s rRNA), H. pylori DNA was identified by PCR. F: 5′ TGGCAATCAGCGTCAGGTAATG3′ and R: 5′GCTAAGA GATCAGCCTAT GTC3′ with product size 522bp. 14
The PCR of H. pylori (16s rRNA) gene was carried out in a 25 µL total volume reaction as follows: 1.5 µL of genomic DNA template, 1 µL of 10 mMdNTP mixture (2.5 dATP, 2.5 mMdGTP, 2.5 mMdCTP, and 2.5 mMdTTP), 1.5 µL of 25 mM MgCl2, 2.5 µL of 10 PCR buffer (10 mMTrisHCl [pH 8.3], 50 mMKCl), 1 µL Taq polymerase (about 1 U), 1.5 µL forward primer, and 1.5 µL reverse primer. The volume of each reaction was completed to 25 µL using twice the D.W (ddH2O). To amplify the H. pylori 16S rRNA gene, the following PCR conditions were employed: an initial denaturation at 94°C for 5 minutes, followed by denaturation at 92°C for 30 seconds in each cycle. This was followed by primer annealing at 55°C for 40 seconds and extension at 72°C for 40 seconds. Finally, a final extension step was performed at 72°C for 5 minutes. The PCR products were then detected using electrophoresis on a 1% agarose gel.
Statistical Analysis
Data were analyzed using SPSS version 26. Chi-square and Fisher’s exact tests were used to compare categorical variables. Quantitative variables are expressed as mean±SD. Statistical significance is defined as a P-value ≤0.05, and 95% confidence intervals are provided.
Results
This study included a total of one hundred gastric biopsies (n=100). The ages of the patients ranged from 10 to 89 years, with a mean age of 42.2 ± 16.8 S.D years. The gender distribution indicated that ; 39 patients (39%) were females, while 61 patients (61%) were males. In patients with gastritis, EBV was detected in 17 patients (17%; 95% CI: 10.2–26.1), while H. pylori was present in 34 patients (34%; 95% CI: 24.9–44.3), as indicated in Figures 1 & 2 and Table 1.
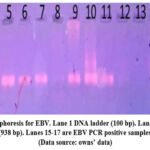 |
Figure 1: Gel electrophoresis for EBV. Lane 1 DNA ladder (100 bp). Lanes 2-14 were negative samples for EBNA-4 (938 bp). Lanes 15-17 are EBV PCR positive samples for EBNA-4 (938 bp) (Data source: owns’ data). |
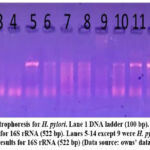 |
Figure 2: Gel electrophoresis for H. pylori. Lane 1 DNA ladder (100 bp). Lanes 2, 3, 4 were negative samples for 16S rRNA (522 bp). Lanes 5-14 except 9 were H. pylori PCR positive results for 16S rRNA (522 bp) (Data source: owns’ data). |
Table 1: Prevalence of EBV and H. pylori among gastritis patients
| PCR results | EBV | H. pylori |
| Positive | 17(17%) | 34(34%) |
| Negative | 83(83%) | 66(66%) |
| Total | 100(100%) | 100(100%) |
(Data source: owns’ data)
The analysis revealed a significant association between EBV and gender, with a p-value =0.012. Among the patients who tested positive for EBV, 15/17 (88.2%) were males, while 2 patients (11.8%) were females. In contrast, the association between EBV and age was insignificant (p-value = 0.961), as shown in Table 2.
Among the 34 patients who tested positive, 20 (58.8%) were males, and 14 (41.2%) were females, indicating a statistically insignificant difference in H. pylori infection rates between genders (p.value = 0.749). Additionally, there was no statistically significant association between H. pylori infection and age, as indicated by a p. value of 0.537, as shown in Table 2.
Additionally, there was no statistically significant association between H. pylori infection and age, as indicated by a p. value of 0.537, as shown in Table 2.
Table 2: The association between EBV and H. pylori and demographic data
| Variable | Total (n=100) | EBV+ ve* (n=17) | H. pylori +ve (n=34) |
| Male | 61 | 15 (88.2%) | 21 (61.8%) |
| Female | 39 | 2 (11.8%) | 13 (38.2%) |
| p-value | 0.012 | 0.749 | |
| Age/years (mean ±SD) | 42.2±16.8 | 44.1±15.2 | 41.3±17.5 |
| p.value | 0.961 | 0.537 | |
* EBV: χ²=6.31
(Data source: own data)
According to the study’s findings, 7 (7%) of gastric biopsies were positive for both H. pylori DNA and EBV. The co-infection (7/100 (7.0%; 95%) of both pathogens (95% CI: 2.9–13.9). However, this co-infection did not demonstrate a significant association (OR=1.32; p. value =0.493; 95% CI: 0.48–3.62) as illustrated in Table 3.
Table 3: Co-infection of EBV and H. pylori among gastritis patients.
| EBV DNA | H. pylori DNA | Total | p. value | |
| Positive | Negative | |||
| Positive | 7(7%) | 10(10%) | 17(17%) |
0.493 |
| Negative | 27(27%) | 56(56%) | 83(83%) | |
| Total | 34(34%) | 66(66%) | 100(100%) | |
(Data source: own data)
Discussion
Gastritis is a common gastrointestinal condition that affects people worldwide. 15 In 2013, there were approximately 90 million new cases, and the disease became more prevalent with age.16 This study provides the first evidence of EBV infection among Sudanese gastritis patients, indicating significant epidemiological differences from global data. The EBV prevalence among patients with gastritis in this study was 17/100 (17.0%). Compared to earlier research, this rate is lower. For instance, Hirano et al. in Japan detected EBV DNA in 23/35 (65.7%) gastric biopsy specimens, while Cárdenas-Mondragón et al. 18 in Mexico, it was 214/333 (64.3%) and higher than that of the Turkish study of Dursun et al. 19, 14/147 (9%), and 14.1% in the Peruvian study by Castaneda et al. 20 suggesting regional variations that may reflect the genetics unique to African populations, socioeconomic, cultural and environmental factors.
This study found that 15 out of 17 (88.2%) males and 2 out of 17 (11.8%) females tested positive for EBV. The likelihood of contracting EBV infection increased with gender, indicating that males are more susceptible (p-value = 0.012). these findings are consistent with research conducted by De Souza et al.21 in Brazil, which reported that only 2 out of 25 positive EBV cases were males, accounting for just 8% of the cases, while no females tested positive. This also aligns with the findings of Al-Humaidan et al. 22 in Saudi Arabia. On the other hand, a Sudanese study by Musa and Ahmed 9 conducted on gastric carcinomas showed a higher prevalence of EBV among males compared to females ( 8 (72.7%) in males vs. 3(27.2%) in females), indicating that the prevalence of EBV in gastric disorders in Sudanese patients is much higher in males than in females. The outcomes of Del Moral-Hernández et al. 23 study in Mexico was inconsistent with the current research findings. Out of the 106 positive samples analyzed, 43.4% were males and 56.6% were females. The results showed no significant association between EBV infection and gender, with a p-value of 0.730. . In this study, EBV-positive males outnumber females, suggesting gender-related susceptibility, possibly due to behavioral, hormonal, or genetic factors. This is consistent with some global studies but differs from others, emphasizing the complexity of EBV’s gender association.
In this study, the prevalence of H. pylori infection among patients with gastritis was found to be 34%. This finding contrasts with the research by Bravo et al.24 in Colombia, which estimated that the prevalence of H. pylori infection among 8,652 gastric biopsies was 69.1%. Additionally, a study published by De Souza et al.21 in Brazil also supports this contrast. The variances in sample sizes , socioeconomic status, sanitation, and access to healthcare. and the research population’s cleanliness may be the cause of the discrepancies in the results.
In the current study, H. pylori was positive in 20/34 (58.8%) of males, while 14/34 (41.2%) of females, with no significant association between H. pylori infection and gender (p. value =0.749), which was consistent with De Souza et al 21 in Brazil, which revealed that 60% of positive cases were males, while 57.6% were females. According to the findings of this study, age is not significantly associated with H. pylori infection (p. value = 0.537).
In the present study, 7 (7%) of gastric biopsies showed co-infection with both EBV and H. pylori. However, no significant association was found between the co-infection of EBV and H. pylori (p. value = 0.493). This finding was similar to the results of Cárdenas-Mondragón et al. in Mexico,18 where 10 (9.4%) of gastric biopsies tested positive for both EBV and H. pylori DNA. Their study differed from ours in that they reported a significant association between EBV and H. pylori, with a p-value of 0.003. Similarly, Castaneda et al. 20 observed a strong association between EBV and H. pylori in Peru, with a p-value of 0.001. The variations could be differences in population genetics, environmental cofactors, or synergistic pathogenic mechanisms that vary by region.
Conclusion
The results of this study concluded that the prevalence of EBV infection is low among gastritis patients in Sudan, and is more common in men than in women. In patients with gastritis, infection with H. pylori is more common than EBV infection, and no association was observed between gender and infection rates and gender or age. These findings underscore the need for further research on EBV’s role in gastritis, particularly in endemic regions, and consideration of sex-stratified approaches.
Acknowledgment
The authors would like to express their gratitude for the collaboration and support of the medical personnel at the Police Hospital. Special thanks are extended to the hospital management for providing access to clinical resources and infrastructure.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
Before participation in the study, informed consent was obtained from all participants. They were fully informed of the study’s objectives, purpose, and possible implications. Participants were informed about the measures taken to ensure their confidentiality during the research. It also ensured the security of their personal information and the anonymization of any data collected to protect their identities.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other source
Not Applicable
Author Contributions
- Hind Haidar Ahmed =Supervised the study, data analysis, conceptualized, visualized, designed, interpreted the results, and wrote the draft paper.
- Israa Elshayeb Ali Mohamed = Principal investigator, wrote the draft paper
- Mutaz F. Saad = Methodology
- Samar Mohammed Saeed= Data analysis
- Wafaa Mohammed Abdalla= Methodology
- Ahmed Bakheet Abd Alla= wrote the draft paper
- May Mohamed Ali = interpretation of the results
- Tagwa Salah Ahmed= editing the manuscript
- Mohammed Siddig Abd Elaziz = editing the manuscript
References
- Kayaçetin S, Güreşçi S. What is gastritis? What is gastropathy? How is it classified? TURK J GASTROENTEROL. 2014; 25(3): 233-247.
CrossRef - Nisa S. Gastritis (Warm-e-meda): A review with Unani approach. j. adv. sci. res. 2018; 3 (3): 43-45.
- Kebede T, Ashenafi H. The Burden and Risk Factors of Helicobacter Pylori Infection Among Government Employees Who Clinically Complain of Indigestion but Allergic Diseases in Southeastern Ethiopia: A Multi-Institution Cross-Sectional Study. Res Rep Trop Med. 2024;15:25-49
CrossRef - World Gastroenterology Organisation. Guideline. Vol. 2021. Milwaukee, USA: World Gastroenterology Organisation; 2021. doi:10.2169/naika.91.547
CrossRef - Rana R, Wang SL, Li J, Wang YX, Rao QW, Yang CQ. Helicobacter pylori infection: A recent approach to diagnosis and management. Biomed. Sci. 2017; 2: 45-56.
CrossRef - Kimura H, Kawada JI, Ito Y. Epstein-Barr virus-associated lymphoid malignancies: the expanding spectrum of hematopoietic neoplasms. Nagoya J. Med. Sci. 2013: 75(3-4): 169.
- Catinean A, Motocu R, Fetica B, Mezei A. Epstein-Barr virus-associated gastric ulcer mimicking gastric neoplasia: a case report. Ultrason. 2019:21(1): 96-98.
CrossRef - Huang W, Bai L, Tang H. Epstein-Barr virus infection: the micro and macro worlds. Virol J. 2023.:20(1): 220
CrossRef - Musa HH, Ahmed M. Association of Epstein-barr virus with gastric carcinoma among Sudanese patients. 2016; 1(1), 46-53.
CrossRef - Traylen C, Ramasubramanyan S, Zuo J. et al. Identification of Epstein-Barr virus replication proteins in Burkitt’s lymphoma cells. 2015; 4(4): 739-751.
CrossRef - Centers for Disease Control and Prevention (CDC). About Epstein-Barr virus (EBV). 2018 Available from: https://www.cdc.gov/epstein-barr/about-ebv.html . (Accessed: 26th August 2019/ 9.42 PM/ Monday).
- Abd Al Rahem S A, Elhag WI. Molecular detection of Helicobacter pylori in drinking water in Khartoum State (Sudan). J. Med. Sci. 2018; 3(5).
- Ahmed HG, Suliman RSAG, El Aziz MSA, Alshammari FD. Molecular screening for Epstein Barr virus (EBV) among Sudanese patients with nasopharyngeal carcinoma (NPC) Agents Cancer, 2015; 10(1): 6.
CrossRef - M Abu-Almaali H, A Al-Khatabi H, A Nasr-Allah H, M Al-Khafaji Z. Duplex PCR primers for detection of Helicobacter pylori DNA directly from gastric biopsy samples. Kerbala J. Pharm. Sci. 2012; 3(3):201-212.
- Mohammed QH. Assessment of Patients Knowledge about Gastritis at General Kirkuk Hospital in Kirkuk City. READ WRIT. 2015; 6:12.
CrossRef - Vos T, Barber RM, Bell B, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the global burden of disease study 2013. LANCET. 2015; 386(9995): 743-800.
CrossRef - Hirano A, Yanai H, Shimizu N, Okamoto T, Matsubara Y, Yamamoto K, Okita K. Evaluation of epstein-barr virus DNA load in gastric mucosa with chronic atrophic gastritis using a real-time quantitative PCR assay. Int J Gastrointest Cancer. 2003. 34(2): 87-94.
CrossRef - Cárdenas-Mondragón MG, Carreon-Talavera R, Camorlinga-Ponce M, Gomez-Delgado A, Torres J, Fuentes-Panana EM. Epstein Barr virus and Helicobacter pylori co-infection are positively associated with severe gastritis in pediatric patients. PLoS One. 2013; 8(4):e62850.
CrossRef - Dursun N, Hacıhasanoğlu E, Okçu O, Paşaoğlu E, Leblebici C. Epstein–Barr virus infection in patients with chronic gastritis without Helicobacter pyloriTurk J Gastroenterol. 2020; 31(3): 205.
- Castaneda CA, Castillo M, Chavez I. et al. Prevalence of Helicobacter pylori Infection, Its Virulent Genotypes, and Epstein-Barr Virus in Peruvian Patients With Chronic Gastritis and Gastric Cancer. J Glob Oncol. 2019; 5:1-9
CrossRef - de Souza CR, de Oliveira KS, Ferraz JJ. et al. Occurrence of Helicobacter pylori and Epstein-Barr virus infection in endoscopic and gastric cancer patients from Northern Brazil. BMC Gastroenterol. 2014;14:179.
CrossRef - Al-Humaidan AY, Al-Khattaf AS, Al-Turaiki IM. et al. Epstein-Barr virus and Helicobacter pylori co-infection in gastric biopsies from Saudi patients. Saudi Med J. 2016; 37(10):1109-1114.
- Del Moral-Hernández O, Castañón-Sánchez CA, Reyes-Navarrete S. el al. Multiple infections by EBV, HCMV and Helicobacter pylori are highly frequent in patients with chronic gastritis and gastric cancer from Southwest Mexico: An observational study. Medicine (Baltimore). 2019 ;98(3):e14124.
CrossRef - Bravo LE, Cortés A, Carrascal E. et al. Helicobacter pylori: patología y prevalencia en biopsias gástricas en Colombia. COLOMB MEDICA, 2003;34(3): 124-131.
CrossRef
Abbreviations List
H. pylori: Helicobacter pylori;
EBV: Epstein-Barr Virus

