
Manuscript accepted on :14-11-2025
Published online on: 10-12-2025
Plagiarism Check: Yes
Reviewed by: Dr. Manju Jakhar and Dr. Soujania Singh
Second Review by: Dr. Sonam Bhutia
Final Approval by: Dr. Patorn Piromchai
Muhammad Irfan Siddique1 , Shakeel Ahmad2and Abida khan3*
, Shakeel Ahmad2and Abida khan3*
1Department of Pharmaceutics, College of Pharmacy, Northern Border University, Rafha, Saudi Arabia.
2Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Lahore University of Biological and Applied Sciences: Lahore, Punjab, Pakistan
3Center for Health Research, Northern Border University, Arar, Saudi Arabia.
Corresponding Author E-mail:abeda.mohammed@nbu.edu.sa
DOI : https://dx.doi.org/10.13005/bpj/3273
Abstract
The use of antipsychotic drugs has expanded beyond their approved indications for schizophrenia and bipolar disorder to include conditions such as insomnia, anxiety, dementia-related behavioral disorders, and pediatric behavioral issues. This review examines prescribing trends, clinical motivations, and ethical concerns surrounding the use of antipsychotic medications across different populations. Second-generation agents—such as risperidone, quetiapine, olanzapine, and aripiprazole—are preferred for off-label use due to their favorable side-effect profiles and reduced risk of extrapyramidal symptoms. However, off-label prescriptions often lack robust supporting evidence, increasing the risk of metabolic syndrome, cardiovascular complications, cognitive decline, and higher mortality among vulnerable patients. Drivers of off-label use include limited approved options, physician practice patterns, and pharmaceutical promotion. Ethical prescribing requires evidence-based justification, informed consent, and vigilant monitoring. This review underscores the need for stricter regulatory guidelines, stronger evidence, and a patient-centered approach to safeguard responsible off-label use of antipsychotic medications.
Keywords
Antipsychotics; Dementia; Ethical considerations; Metabolic side effects; Off-label prescribing; Pediatric psychiatry; Second-generation antipsychotics
Download this article as:| Copy the following to cite this article: Siddique M. I, Ahmad S, Khan A. Trends in the Use of Antipsychotics for Off-Label Indications: Clinical and Ethical Considerations. Biomed Pharmacol J 2025;18(4). |
| Copy the following to cite this URL: Siddique M. I, Ahmad S, Khan A. Trends in the Use of Antipsychotics for Off-Label Indications: Clinical and Ethical Considerations. Biomed Pharmacol J 2025;18(4). Available from: https://bit.ly/4pYiW1x |
Introduction
Antipsychotic medications were originally developed to manage severe psychiatric disorders such as schizophrenia and bipolar disorder. In recent years, however, their use has expanded to a wider range of psychiatric and behavioral conditions, including anxiety, insomnia, post-traumatic stress disorder (PTSD), personality disorders, and behavioral disturbances in dementia and pediatric populations.1 This growing off-label use has sparked ongoing discussion about its clinical justification and ethical implications.
Second-generation antipsychotics (SGAs)—including risperidone, quetiapine, olanzapine, and aripiprazole—are now more frequently prescribed due to their broader therapeutic profiles and reduced risk of neurological side effects compared with first-generation agents.2 Despite their perceived tolerability, these medications are often used in contexts where strong clinical evidence is lacking. This practice raises important concerns about safety, informed consent, and the long-term impact of such treatments on patient well-being.3,4 In pediatric populations, the off-label use of antipsychotics has risen significantly despite limited evidence and the absence of large-scale, long-term studies.5 The exclusion of children from many clinical trials, coupled with restrictive licensing, has contributed to reliance on off-label prescribing.6,7 This trend highlights the need for cautious, evidence-based approaches and careful ethical oversight when treating younger patients. 8 Overall, real-world prescribing practices often diverge from established guidelines.9 Documented adverse effects such as metabolic disturbances, extrapyramidal symptoms, and increased mortality among elderly patients underscore the need for more responsible, evidence-driven use.10,11 This review aims to examine global trends and clinical motivations behind off-label antipsychotic use and to explore the associated risks and ethical challenges in different populations.
Understanding Off-Label Prescribing and Antipsychotics
Off-label prescribing refers to the use of an approved medication for purposes not specified in its official labeling—such as a different indication, dose, patient group, or route of administration.12 Regulatory authorities, such as the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA), permit such prescribing when supported by sound clinical judgment, though manufacturers are prohibited from promoting these uses.13 While legal, this practice raises important ethical and safety considerations, particularly when applied to vulnerable populations such as children or the elderly.14 Off-label use often arises due to limited approved treatment options, emerging or anecdotal evidence, and the need for individualized care when standard therapies fail to achieve adequate results. Clinicians may rely on their experience and patient-specific factors to make these decisions, underscoring the balance between therapeutic innovation and patient safety.
Antipsychotic medications are broadly categorized into two groups based on their pharmacological action. First-generation (typical) antipsychotics primarily block dopamine D₂ receptors, while second-generation (atypical) agents act on both dopamine and serotonin receptors. This dual mechanism gives atypical antipsychotics a broader therapeutic range and contributes to their widespread use in off-label contexts.15 Although such prescribing offers flexibility in treatment, it also highlights the need for robust evidence and careful monitoring to ensure that patient welfare remains the primary consideration.16
Patterns of Off-Label Antipsychotic Use across Populations
Off-label prescribing of antipsychotics spans all age groups, though the indications, prescribing patterns, and associated concerns differ considerably based on age. Across the lifespan, the use of these medications outside of approved indications raises important clinical and ethical questions, particularly regarding efficacy, safety, and long-term outcomes. 17
In children and adolescents, off-label use of antipsychotics has increased significantly over the past two decades. Prevalence rates range from 36% to 93.2%, with risperidone and aripiprazole being the most commonly prescribed agents. These medications are often used to address behavioral symptoms such as aggression, irritability, and impulsivity in conditions like ADHD, autism spectrum disorder, and mood disorders, despite limited long-term safety data and concerns about their impact on neurodevelopment.4 The shift toward second-generation antipsychotics (SGAs) in pediatric populations reflects efforts to reduce extrapyramidal side effects, yet these agents are associated with significant metabolic risks, including weight gain, insulin resistance, and dyslipidemia 11
In adults, off-label prescribing is both widespread and diverse, with estimates suggesting that 40% to 75% of antipsychotic prescriptions fall into this category.18 Quetiapine is frequently used at low doses for conditions such as insomnia, generalized anxiety disorder, and as an adjunct in depression. While its sedative and anxiolytic properties may provide symptomatic relief, the strength of evidence supporting such use is generally low to moderate, and concerns about overuse persist. Commonly prescribed antipsychotics for off-label adult use include quetiapine, olanzapine, and risperidone, though associated risks such as sedation, metabolic syndrome, and extrapyramidal symptoms necessitate careful monitoring and justification.19
Among elderly individuals, particularly those with dementia, antipsychotics are frequently used off-label to manage behavioral and psychological symptoms such as agitation and aggression. Despite FDA black box warnings highlighting increased risks of cerebrovascular events and mortality in this population, studies report off-label use rates ranging from 22% to 86%.20 Haloperidol, risperidone, and olanzapine are among the most commonly prescribed agents, although evidence for their efficacy in dementia-related agitation remains limited.21
Off-label use is most prominent among vulnerable groups, including older adults, children, and women. Elderly patients, particularly those in long-term care, are often prescribed antipsychotics for behavioral disturbances linked to dementia, despite heightened risks such as stroke and death.22 Children and adolescents are frequently treated with SGAs for ADHD, conduct disorders, and autism-related symptoms. However, safety data for long-term use in pediatric populations remain limited. Women may be disproportionately affected by certain antipsychotic side effects, such as hormonal and metabolic changes.23
Common Off-Label Indications for Antipsychotics
Behavioral and Psychological Symptoms of Dementia (BPSD)
Behavioral and psychological symptoms of dementia (BPSD)—including agitation, aggression, delusions, hallucinations, and mood disturbances—affect up to 90% of individuals with Alzheimer’s disease and other forms of dementia. These symptoms greatly impair patients’ quality of life, place heavy emotional and physical burdens on caregivers, and often lead to increased off-label prescribing of antipsychotic medications.24
Clinicians frequently resort to antipsychotics despite only modest and inconsistent evidence of their effectiveness for BPSD. Randomized controlled trials have reported variable outcomes, and overall efficacy remains uncertain when weighed against the substantial risks involved. These risks—such as cerebrovascular events, increased fall risk, accelerated cognitive decline, and heightened mortality—are particularly concerning in elderly populations.25
In recognition of these dangers, the U.S. Food and Drug Administration (FDA) issued a black box warning in 2005 highlighting increased mortality associated with atypical antipsychotic use in dementia patients. Current guidelines recommend reserving antipsychotics as a last-line option, only after non-pharmacological interventions such as behavioral strategies, caregiver training, and environmental modifications have been exhausted. The use of these medications in dementia care raises major ethical concerns, especially regarding informed consent and the principle of non-maleficence.26
In Japan, some older agents such as thioridazine and vegetamin remain approved for geriatric psychosis; however, second-generation antipsychotics are now preferred due to their lower risk of extrapyramidal symptoms, though they still carry serious metabolic and cardiovascular risks.27
Mood and Anxiety Disorders
Mood disorders—including major depressive disorder (MDD)—and anxiety disorders such as generalized anxiety disorder (GAD) and obsessive-compulsive disorder (OCD) are among the most common off-label indications for antipsychotic use.28 While atypical antipsychotics may provide symptom relief in resistant cases, their long-term use poses significant risks, including weight gain, metabolic dysregulation, and extrapyramidal side effects.
Insomnia
Quetiapine and olanzapine are increasingly prescribed off-label for insomnia due to their sedative properties mediated by antihistaminergic and serotonergic receptor blockade. This trend has grown particularly when conventional treatments—such as hypnotic agents or cognitive behavioral therapy for insomnia (CBT-I)—have failed.29
However, these drugs are not approved as sleep aids, and evidence does not show superior efficacy compared with standard hypnotics. Even at low doses, they carry serious risks such as weight gain, dyslipidemia, glucose intolerance, and residual next-day sedation. Current clinical guidelines emphasize extreme caution, advising that antipsychotics should be considered for insomnia only after all other options have failed and under strict monitoring.30
Treatment-Resistant Depression
In cases of treatment-resistant depression—defined as inadequate response to at least two antidepressant trials—second-generation antipsychotics (SGAs) such as aripiprazole, quetiapine, and olanzapine (often in combination with fluoxetine) are frequently used as augmentation therapy. Although some evidence supports their short-term efficacy, these regimens require careful risk–benefit evaluation due to potential metabolic and neurological side effects.31
Pediatric and Adolescent Psychiatric Disorders
Off-label antipsychotic use has grown substantially in children and adolescents for conditions such as attention-deficit/hyperactivity disorder (ADHD), anxiety, and mood disorders. This trend raises significant safety and ethical concerns, given the ongoing brain development in this population and their increased vulnerability to adverse effects. Rigorous long-term studies are needed to clarify efficacy and ensure safe prescribing practices in youth.32
Eating Disorders
Antipsychotic medications, particularly olanzapine, have been evaluated for the treatment of anorexia nervosa and, to a lesser extent, bulimia nervosa. In anorexia nervosa, olanzapine may help reduce anxiety and cognitive rigidity related to weight and food, and may modestly aid weight restoration. However, findings remain inconsistent, and patient acceptability is variable. Evidence for efficacy in bulimia nervosa is limited, with little effect observed on binge–purge behavior. Consequently, antipsychotics should be used only as adjunctive therapy alongside evidence-based psychotherapies. Further research is essential to determine their role in these disorders.33
Other Off-Label Applications
Antipsychotics are also prescribed off-label for several additional conditions, including personality disorders, post-traumatic stress disorder (PTSD), substance use disorders, chronic pain syndromes, and some somatic conditions such as irritable bowel syndrome (IBS) and benign paroxysmal positional vertigo (BPPV). In borderline personality disorder, low-dose SGAs may reduce impulsivity and affective instability, though the supporting evidence is limited. Similarly, in PTSD and substance dependence, antipsychotics may be used to alleviate associated symptoms like insomnia or aggression, but their risks often outweigh potential benefits.34 Some observational studies and clinical anecdotes report antipsychotic use for chronic pain or somatic symptoms, likely due to their sedative and central nervous system-modulating properties. Nonetheless, such use should be considered experimental and requires further investigation.
Commonly Used Antipsychotics in Off-Label Practice
Quetiapine is frequently prescribed off-label, particularly for the management of anxiety and insomnia.35 Although approved for schizophrenia and bipolar disorder, its sedative properties—primarily mediated through antagonism of histaminergic and serotonergic receptors—have contributed to its popularity for off-label use. The drug’s perceived tolerability and calming effects make it an appealing option when standard treatments are ineffective or poorly tolerated. However, this widespread use raises concerns about insufficient supporting evidence and the potential for adverse effects.36
The growing prescription of low-dose quetiapine for non-psychotic symptoms such as anxiety and insomnia has emerged as a significant public health concern. Even at lower doses, quetiapine is associated with weight gain, dyslipidemia, glucose intolerance, and cardiovascular complications. Limited data on its long-term safety raises additional worries regarding tolerance, dependence, and cumulative side effects.37 Moreover, this trend may contribute to the underutilization of evidence-based interventions—such as cognitive behavioral therapy for insomnia (CBT-I) and selective serotonin reuptake inhibitors (SSRIs) for anxiety. Observational studies further indicate that quetiapine is the most commonly prescribed antipsychotic among individuals without diagnoses typically warranting antipsychotic treatment, suggesting it is often used more for its sedative than antipsychotic properties.38
Risperidone and aripiprazole are also widely used off-label, particularly in pediatric and adolescent populations for conditions such as attention-deficit/hyperactivity disorder (ADHD), anxiety disorders, and mood dysregulation. These agents are often prescribed to manage behavioral symptoms, including aggression, impulsivity, and agitation. However, their off-label use in developing individuals presents both ethical and clinical challenges due to potential long-term neurodevelopmental effects and an increased risk of metabolic disturbances. Careful monitoring and adherence to evidence-based guidelines are therefore essential when considering their use in children and adolescents.39
Olanzapine, while approved for schizophrenia and bipolar disorder, is also used off-label to treat anxiety, agitation, and insomnia. Despite its clinical effectiveness, it carries a high risk of metabolic side effects, including substantial weight gain, insulin resistance, and lipid abnormalities. The commonly used antipsychotics and their key concern are described in Table 1. These risks necessitate cautious and closely monitored prescribing, particularly when olanzapine is used for non-psychotic conditions. Global prescribing data indicate that olanzapine remains among the most frequently utilized antipsychotics, highlighting the importance of balancing therapeutic benefits with potential long-term health consequences.40
Table 1: Key concerns regarding commonly used Antipsychotics
| Indication | Commonly Used Antipsychotics | Evidence Strength | Key Concerns |
| Insomnia | Quetiapine | Low | Sedation, metabolic syndrome |
| Generalized Anxiety Disorder | Olanzapina, Quetiapine, Risperidone | Moderate | Weight gain, extrapyramidal symptoms (EPS) |
| PTSD | Risperidone, Quetiapine | Low to Moderate | Mixed efficacy, sedation |
| Dementia-related Agitation | Haloperidol, Risperidone, Olanzapine | Low | Increased mortality, cerebrovascular risks |
| ADHD (Children) | Risperidone, Aripiprazole | Low to Moderate | Long-term safety concerns, metabolic complications |
| Borderline Personality Disorder | Olanzapine, Aripiprazole | Moderate | Limited consensus, adverse effects |
Factors Influencing Off-Label Prescribing
One of the primary drivers of off-label prescribing is the absence of approved pharmacological treatments for certain conditions. In many clinical scenarios—particularly those involving rare, complex, or newly defined disorders—clinicians are left with few or no formally approved options. This therapeutic gap often prompts the use of existing medications in unapproved ways in hopes of alleviating patient symptoms or preventing clinical deterioration. While such decisions arise from necessity, they do not exempt prescribers from the responsibility to ensure that these interventions are supported by at least some degree of scientific rationale and safety data.41
A pertinent example is the treatment of disruptive mood dysregulation disorder (DMDD), a relatively recent diagnosis in child and adolescent psychiatry. Characterized by chronic irritability and severe temper outbursts, DMDD lacks any FDA-approved pharmacotherapy. As a result, clinicians frequently turn to off-label use of antipsychotics, antidepressants, and mood stabilizers.42 However, given the limited evidence supporting these strategies—and the developmental sensitivity of this population—such practice raises ethical questions about potential harm, informed consent, and the need for more rigorous research into safer alternatives.43
In other cases, off-label prescribing becomes a last resort after conventional treatments have failed due to inefficacy or intolerable side effects. While these decisions may reflect a genuine desire to relieve suffering when options are limited, they should be guided by careful consideration of risks and benefits and, ideally, be accompanied by shared decision-making with the patient and caregivers.44 Prescribing behavior is also influenced by a physician’s clinical experience, personal treatment observations, and perception of therapeutic outcomes. Although experiential knowledge can enhance decision-making in complex cases, it may also introduce bias—especially when decisions are based more on anecdotal success than on scientific evidence. Physicians who observe perceived improvements in patients receiving off-label antipsychotics may be more inclined to repeat those prescriptions, sometimes overestimating efficacy or downplaying potential adverse effects.45
Furthermore, when approved treatments fail or are poorly tolerated, clinicians often feel a moral obligation to explore all possible options—even when those options are not rigorously validated. This sense of duty to alleviate suffering can drive continued off-label use, particularly in areas where standard guidelines provide limited direction.46
The preference for second-generation (atypical) antipsychotics over older, typical agents is often rooted in ethical considerations related to patient safety rather than economic motivations. Atypical agents tend to have a more favorable side-effect profile regarding extrapyramidal symptoms, which supports their use in vulnerable populations.15 However, this does not absolve clinicians of the responsibility to evaluate each case individually and to ensure that the patient or guardian is adequately informed about potential risks. Clinical judgment should remain central to prescribing decisions but must operate within an ethical and evidence-based framework.
Another influential factor in off-label prescribing is pharmaceutical marketing. Although regulations prohibit companies from explicitly promoting off-label uses, subtle marketing strategies often blur these boundaries.10 Sponsored continuing medical education (CME) events, paid speaker programs, and the distribution of literature emphasizing a drug’s secondary benefits can indirectly encourage off-label prescribing. Such materials, while presented as educational, may understate risks and overstate therapeutic benefits.47
Physicians—particularly those working in high-pressure environments with limited time—may unintentionally adopt these promotional narratives, especially when they resonate with personal clinical experiences or fill a perceived treatment void. This process can normalize off-label prescribing even in the absence of robust evidence, ultimately shaping systemic prescribing trends.48 Promoting transparency in research, strengthening regulatory oversight, and encouraging reliance on independent, peer-reviewed evidence are essential to counteract excessive industry influence. In addition, incorporating education on pharmaceutical ethics and critical appraisal skills into medical training can empower clinicians to make informed, autonomous decisions that prioritize patient welfare over promotional messaging.49,50
Risks and Adverse Effects of Off-Label Antipsychotic Use
Antipsychotics—particularly second-generation agents—are associated with significant metabolic and cardiovascular complications, including weight gain, dyslipidemia, diabetes, and QT interval prolongation.2 These effects can result in serious long-term health consequences, especially among vulnerable populations. First-generation drugs carry higher risks of extrapyramidal symptoms (EPS) and tardive dyskinesia (TD), whereas second-generation agents require vigilant monitoring for metabolic syndrome. Regular assessment of body weight, glucose levels, and lipid profiles is essential to detect and manage these adverse outcomes early. 51
Cardiovascular side effects, particularly QT interval prolongation, can elevate the risk of life-threatening arrhythmias such as torsades de pointes and sudden cardiac death. Patients with pre-existing heart disease, concurrent QT-prolonging medications, or advanced age are especially susceptible and should undergo periodic ECG monitoring and cardiac risk evaluation.52, 53
Neurological adverse effects, including EPS and TD, occur more frequently with first-generation antipsychotics (FGAs) but can also appear with second-generation agents (SGAs), particularly at higher doses or in predisposed individuals.54 EPS includes akathisia, dystonia, Parkinsonism, and acute dystonic reactions, whereas TD is characterized by chronic, involuntary movements. Both require close clinical observation for early recognition and intervention. 55, 56
Long-term antipsychotic therapy may also impair cognitive function and cause excessive sedation, negatively affecting daily functioning and quality of life. These risks are especially pronounced in elderly patients who already face cognitive decline and an increased likelihood of falls or cerebrovascular events.57 Evidence further indicates that the benefits of antipsychotic use for behavioral and psychological symptoms of dementia (BPSD) are limited, while the potential harms—particularly in frail older adults—remain substantial.58
Children, adolescents, and individuals with intellectual disabilities represent another high-risk group due to ongoing brain development and difficulties in recognizing or reporting adverse effects.59 Prescribing for these populations should be approached with heightened caution, supported by careful monitoring and preference for non-pharmacological interventions whenever feasible.60 The figure 1 illustrates the balance clinicians must maintain between maximizing clinical benefit, minimizing risks, and upholding ethical duty — with responsible off-label prescribing positioned at the intersection.
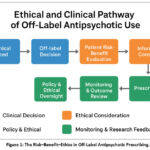 |
Figure 1: The Risk–Benefit–Ethics in Off-Label Antipsychotic Prescribing. |
Ethical Considerations in Off-Label Prescribing
Responsible off-label prescribing of antipsychotic medications requires a multifaceted approach grounded in ethical principles, clinical prudence, and ongoing evaluation. A central tenet of this practice is evidence-based decision-making.61 Prescribers should rely on high-quality clinical evidence—such as systematic reviews, meta-analyses, and updated treatment guidelines—when considering off-label use.62 Clinical judgments must be informed not only by published data but also by a critical appraisal of the strength, limitations, and applicability of that evidence.63
Before initiating treatment, a comprehensive patient assessment is essential. This includes a full diagnostic evaluation and consideration of both pharmacological and non-pharmacological options. In pediatric and geriatric populations, especially, non-drug approaches—such as behavioral therapy, environmental modifications, and psychoeducation—should be prioritized when appropriate.64 Pharmacological intervention should be considered only when these strategies prove inadequate or ineffective.
Informed consent is a cornerstone of ethical off-label prescribing. Given the unique risks associated with antipsychotic medications, patients or their legal guardians must be clearly informed that the drug is not approved for the intended indication. Discussion should include potential risks, anticipated benefits, and available alternative treatments. Transparent communication fosters patient autonomy, strengthens the therapeutic alliance, and enhances trust in clinical care.10 Once treatment is initiated, ongoing monitoring is imperative. Regular follow-up visits should assess both therapeutic outcomes and adverse effects. Parameters such as weight, glucose levels, lipid profiles, and extrapyramidal symptoms should be routinely evaluated. If the risks begin to outweigh the benefits, dose adjustment or discontinuation should be considered.65
Institutional or national guidelines further supports ethical prescribing by providing structured protocols for specific scenarios. The development and implementation of such frameworks standardize care, improve clinician confidence, and reduce practice variability. These protocols should be tailored to common off-label indications—such as behavioral disturbances in dementia or aggression in youth with developmental disorders.14
To guide future practice, more robust research is needed. Well-designed clinical and observational studies should evaluate the safety and effectiveness of off-label antipsychotic use in real-world settings. The use of electronic health records and post-marketing surveillance systems can enhance data collection, allowing clinicians to make better-informed, evidence-based decisions.66
Conclusion
The off-label use of antipsychotic medications has become increasingly prevalent across a wide range of clinical contexts, involving diverse patient populations and psychiatric conditions. This review highlights evolving prescribing trends, particularly among vulnerable groups such as children, the elderly, and those with treatment-resistant disorders. Although second-generation antipsychotics are often preferred for their broader receptor profiles and perceived tolerability, evidence supporting many of their off-label uses remains limited. Ethical concerns—particularly regarding informed consent, risk disclosure, and long-term safety—emphasize the need for cautious and evidence-based prescribing.
Ultimately, the ethical and responsible use of antipsychotics in off-label scenarios requires a balanced approach—one that weighs potential benefits against the risk of harm while respecting patient autonomy and ensuring continuous monitoring. As psychiatry continues to evolve, so too must standards for off-label prescribing. A steadfast commitment to evidence-based practice, transparency, and ethical integrity is essential to protect patients and uphold public trust in psychiatric care.
Acknowledgement
The authors extend their appreciation to Northern Border University, Saudi Arabia, for supporting this work through project number (NBU-CRP-2025-2042).
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not Applicable.
Author Contributions
- Muhammad Irfan Siddique was responsible for the conceptualization, methodology and final approval of the manuscript;
- Shakeel was responsible for the methodology, analysis whereas,
- Abida Khan was responsible for data collection, analysis and writing.
References
- Pesiou S, Barcelo R, Papazisis G, Torres F, Pontes C. Prevalence of use of on-label and off-label psychotropics in the Greek pediatric population. Front Pharmacol. 2024; 15: 1348887.
CrossRef - Stogios N, Smith E, Bowden S, et al. Metabolic adverse effects of off-label use of second-generation antipsychotics in the adult population: a systematic review and meta-analysis. Neuropsychopharmacology, 2022; 47(3): 664-672.
CrossRef - Braüner JV, Johansen LM, Roesbjerg T, Pagsberg AK. Off-Label Prescription of Psychopharmacological Drugs in Child and Adolescent Psychiatry. J Clin Psychopharmacol. 2016; 36(5): 500-507.
CrossRef - Zhaojian W, Meizhu J, Jun H, et al. Trends and off-label utilization of antipsychotics in children and adolescents from 2016 to 2021 in China: a real-world study. Child Adolesc Psychiatry Ment Health, 2024; 18(1): 77.
CrossRef - Zito JM, Safer DJ, Berg LT, et al. A three-country comparison of psychotropic medication prevalence in youth. Child Adolesc Psychiatry Ment Health, 2008; 2(1): 26.
CrossRef - Malik M, Ghani MU, Mazhar W, Munir N. Changing trends in antipsychotic prescription pattern in Pakistan. Pak J Med Sci. 2019; 35(3): 653-657.
CrossRef - Mahmood S, Hussain S, Ur Rehman T, Barbui C, Kurdi AB, Godman B. Trends in the prescribing of antipsychotic medicines in Pakistan: implications for the future. Curr Med Res Opin. 2019; 35(1): 51-61.
CrossRef - Bastaki K, El Anbari M, Ghuloum S, Jithesh PV. Prescription Pattern and Off-Label Use of Antipsychotics in a Middle Eastern Population. Front Pharmacol. 2021; 12: 753845.
CrossRef - Vijay, A., J.E. Becker, and J.S. Ross. Patterns and predictors of off-label prescription of psychiatric drugs. PLOS ONE, 2018. 13(7): p. e0198363.
CrossRef - Van Norman GA. Off-Label Use vs Off-Label Marketing of Drugs: Part 1: Off-Label Use-Patient Harms and Prescriber Responsibilities. JACC Basic Transl Sci. 2023; 8(2): 224-233.
CrossRef - Lee H, Zhang C, Rose R. Pediatric Off-label Antipsychotic Use for Attention-Deficit/Hyperactivity Disorder. Clin Ther. 2022; 44(9): e83-e90.
CrossRef - Dennis JA, Gittner LS, Payne JD, Nugent K. Characteristics of U.S. adults taking prescription antipsychotic medications, National Health and Nutrition Examination Survey 2013–2018. BMC Psychiatry, 2020; 20(1): 483.
CrossRef - Weda M, Hoebert J, Vervloet M, et al. Study on off-label use of medicinal products in the European Union. Publications Office of the European Union; 2019.
- Day RO. Ongoing challenges of off-label prescribing. Australian Prescriber. 2023; 46(4): 86-89.
CrossRef - Devlin AM, Panagiotopoulos C. Metabolic side effects and pharmacogenetics of second-generation antipsychotics in children. Pharmacogenomics, 2015; 16(9): 981-996.
CrossRef - Aguglia A, Serafini G, Nebbia J, et al. Off-Label Use of Second-Generation Antipsychotics in Borderline Personality Disorder: A Survey of Italian Psychiatrists. J Pers Disord. 2021; 35(3): 321-335.
CrossRef - Leucht S, Priller J, Davis JM. Antipsychotic drugs: a concise review of history, classification, indications, mechanism, efficacy, side effects, dosing, and clinical application. Am J Psychiatry, 2024; 181(10): 865-878.
CrossRef - Arranz MJ, Salazar J, Hernández MH. Pharmacogenetics of antipsychotics: Clinical utility and implementation. Behav Brain Res. 2021; 401: 113058.
CrossRef - Costales B, Slama NE, Penfold RB, et al. On-and off-label atypical antipsychotic prescription trends across a nine-year period among adolescents pre-to post-COVID-19. Acad Pediatr. 2024; 24(6): 995-1000.
CrossRef - Giurin MS, Trojniak MP, Arbo A, et al. Safety of Off-Label Pharmacological Treatment in Pediatric Neuropsychiatric Disorders: A Global Perspective From an Observational Study at an Italian Third Level Children’s Hospital. Front Pharmacol. 2022; 13: 837692.
CrossRef - Aichhorn W, Whitworth AB, Weiss EM, Hinterhuber H, Marksteiner J. Differences between men and women in side effects of second-generation antipsychotics. Nervenarzt. 2007; 78(1): 45-52.
CrossRef - de Bartolomeis A, Barone A, Begni V, Riva MA. Present and future antipsychotic drugs: A systematic review of the putative mechanisms of action for efficacy and a critical appraisal under a translational perspective. Pharmacol Res. 2022; 176: 106078.
CrossRef - Jensen-Dahm C, Christensen AN, Gasse C, Waldemar G. The use of opioids and antipsychotics in elderly with dementia–have opioids replaced antipsychotics in treating behavioral symptoms in dementia? J Alzheimers Dis. 2020; 73(1): 259-267.
CrossRef - Petkova V, Georgieva D, Dimitrov M, Nikolova I. Off-label prescribing in pediatric population – Literature review for 2012–2022. Pharmaceutics, 2023; 15(12): 2652.
CrossRef - Krishnan RPR, Harrison C, Buckley N, Raubenheimer JE. On- and off-label utilisation of antipsychotics in Australia (2000–2021): Retrospective analysis of two medication datasets. Aus N Z J Psychiatry, 2024; 58(4): 320-333.
CrossRef - Zhang Y, Letuchy EM, Carnahan RM. Where Are Antipsychotics Prescribed in Nursing Homes Initiated? J Am Geriatr Soc. 2018; 66(6): 1082-1088.
CrossRef - Hunt-Grubbe H. Ethical Issues Arising from the Prescription of Antipsychotic Medication in Clinical Forensic Settings. In: Igoumenou, A. (eds) Ethical Issues in Clinical Forensic Psychiatry. 2020; 99-114.
CrossRef - Oguchi Y, Miyake N, Ando K. Barriers to long-acting injectable atypical antipsychotic use in Japan: Insights from a comparative psychiatrist survey. Neuropsychopharmacol Rep. 2024; 44(2): 417-423.
CrossRef - Bains N, Abdijadid S. Major Depressive Disorder. In StatPearls. StatPearls Publishing LLC, Treasure Island (FL); 2025.
- Khaledi-Paveh B, Maazinezhad S, Rezaie L, Khazaie H. Treatment of chronic insomnia with atypical antipsychotics: results from a follow-up study. Sleep Sci. 2021; 14(1): 27-32.
- Makary S, Abd El Moez K, Elsayed M, Hassan H. Second-generation antipsychotic medications and metabolic disturbance in children and adolescents. Egypt J Neurol Psychiatry Neurosurg. 2023; 59(1): 14.
CrossRef - Han R, Bian Q, Chen H. Effectiveness of olanzapine in the treatment of anorexia nervosa: A systematic review and meta-analysis. Brain Behav. 2022; 12(2): e2498.
CrossRef - Wang J, Jiang F, Yang Y, et al. Off-label use of antipsychotic medications in psychiatric inpatients in China: a national real-world survey. BMC Psychiatry, 2021; 21(1): 375.
CrossRef - Seidel S, Aigner M, Ossege M, Pernicka E, Wildner B, Sycha T. Antipsychotics for Acute and Chronic Pain in Adults. J Pain Symptom Manage. 2010; 39: 768-778.
CrossRef - Lin CY, Chiang CH, Tseng MC, Tam KW, Loh EW. Effects of quetiapine on sleep: A systematic review and meta-analysis of clinical trials. Eur Neuropsychopharmacol. 2023; 67: 22-36.
CrossRef - Brett J. Concerns about quetiapine. Aust Prescr. 2015; 38(3): 95-97.
CrossRef - Taipale H, Mittendorfer-Rutz E, Alexanderson K, et al. Antipsychotics and mortality in a nationwide cohort of 29,823 patients with schizophrenia. Schizophr Res. 2018; 197: 274-280.
CrossRef - Rafaniello C, Sullo MG, Carnovale C, et al. We really need clear guidelines and recommendations for safer and proper use of aripiprazole and risperidone in a pediatric population: real-world analysis of EudraVigilance database. Front Psychiatry, 2020; 11: 550201.
CrossRef - Coughlin M. Improving Metabolic Monitoring and Promoting Safe Use of Second-Generation Antipsychotics in Children and Adolescents. PhD dissertation. Queen’s University, Kingston; 2017.
CrossRef - Libowitz MR, Nurmi EL. The Burden of Antipsychotic-Induced Weight Gain and Metabolic Syndrome in Children. Front Psychiatry, 2021; 12: 623681.
CrossRef - Balan S, Hassali MAAA, Mak VS. Two decades of off-label prescribing in children: a literature review. World J Pediatr. 2018; 14: 528-540.
CrossRef - Shakeel S, Nesar S, Rehman H, et al. Patterns and predictors of off-label drug prescribing in psychiatric practice: a qualitative study. Pharmacy, 2021; 9(4): 203.
CrossRef - Mathews B. Adolescent capacity to consent to participate in research: a review and analysis informed by law, human rights, ethics, and developmental science. Laws, 2022; 12(1): 2.
CrossRef - Jansen RM. Off-Label Use of Medication, in Legal and Forensic Medicine, R.G. Beran, Editor. Springer Berlin Heidelberg, Berlin, Heidelberg, 2013; 1601-1615.
CrossRef - Pirhonen E, Haapea M, Rautio N, et al. Characteristics and predictors of off-label use of antipsychotics in general population sample. Acta Psychiatr Scand. 2022; 146(3): 227-239.
CrossRef - Gazarian M, Horton DB, Carleton B, Kinlaw AC. Optimizing therapeutic decision‐making for off‐label medicines use: A scoping review and consensus recommendations for improving practice and research. Pharmacoepidemiol Drug Saf. 2023; 32(11): 1200-1222.
CrossRef - Thippaiah SM, Fargason RE, Birur B. Switching antipsychotics: A guide to dose equivalents. Curr Psychiatry. 2021; 20(4): 13-14.
CrossRef - Landwehr C, Richardson J, Bint L, Parsons R, Sunderland B, Czarniak P. Cross-sectional survey of off-label and unlicensed prescribing for inpatients at a paediatric teaching hospital in Western Australia. PloS One. 2019; 14(1): e0210237.
CrossRef - Dresser R, Frader J. Off-Label Prescribing: A Call for Heightened Professional and Government Oversight. J Law, Med Ethics, 2009; 37(3): 476–486.
CrossRef - Pratico AD, Longo L, Mansueto S, et al. Off-label use of drugs and adverse drug reactions in pediatric units: a prospective, multicenter study. Curr Drug Saf. 2018; 13(3): 200-207.
CrossRef - van der Zanden TM, Mooij MG, Vet NJ, et al. Benefit‐risk assessment of off‐label drug use in children: the bravo framework. Clin Pharmacol Ther. 2021; 110(4): 952-965.
CrossRef - Gładysz A, Zamorski M, Stebel A, Ligoda J, Machaj R, Mach F. Antipsychotic drugs and their possible cardiovascular adverse effects–literature review. Current Prob Psychiatry, 2024; 25: 215-225.
CrossRef - Poojari PG, Mey A, Khan SA, et al. Consumers’ and practitioners’ perspectives on the antipsychotic induced metabolic syndrome and challenges in metabolic monitoring to patient prescribed second generation antipsychotics in severe mental illness. J Health Psychol. 2025: 13591053251315263.
CrossRef - Ali RA, Jalal Z, Paudyal V. Barriers to monitoring and management of cardiovascular and metabolic health of patients prescribed antipsychotic drugs: a systematic review. BMC psychiatry, 2020; 20: 1-15.
CrossRef - Carbon M, Kane JM, Leucht S, Correll CU. Tardive dyskinesia risk with first‐and second‐generation antipsychotics in comparative randomized controlled trials: a meta‐analysis. World Psychiatry, 2018; 17(3): 330-340.
CrossRef - Dilks S, Xavier RM, Kelly C, Johnson J. Implications of antipsychotic use: antipsychotic-induced movement disorders, with a focus on tardive dyskinesia. Nurs Clin North Am. 2019; 54(4): 595-608.
CrossRef - MacKenzie NE, Kowalchuk C, Agarwal SM, et al. Antipsychotics, Metabolic Adverse Effects, and Cognitive Function in Schizophrenia. Front Psychiatry. 2018; 9: 622.
CrossRef - Carlo YEV, Saracco-Alvarez RA, Valencia Carlo VA, et al. Adverse effects of antipsychotics on sleep in patients with schizophrenia. Systematic review and meta-analysis. Front Psychiatry. 2023; 14: 1189768.
CrossRef - Rogowska M, Thornton M, Creese B, et al. Implications of Adverse Outcomes Associated with Antipsychotics in Older Patients with Dementia: A 2011-2022 Update. Drugs Aging, 2023; 40(1): 21-32.
CrossRef - Garcia-Amador M, Merchán-Naranjo J, Tapia C, et al. Neurological Adverse Effects of Antipsychotics in Children and Adolescents. J Clin Psychopharmacol. 2015; 35(6): 686-93.
CrossRef - Lunsky Y, Khuu W, Tadrous M, Vigod S, Cobigo V, Gomes T. Antipsychotic Use With and Without Comorbid Psychiatric Diagnosis Among Adults with Intellectual and Developmental Disabilities. Can J Psychiatry, 2018; 63(6): 361-369.
CrossRef - de Kuijper GM, Lenderink AW. Antipsychotic Drug Prescription and Behavioral Problems in Individuals with Intellectual Disability, in NeuroPsychopharmacotherapy. Riederer P, et al., Editors. Springer International Publishing, 2020; 1-21.
CrossRef - Verdoux H, Antipsychotic off-label use in the 21st century: An enduring public health concern. Dialogues Clin Neurosci. 2025; 27(1): 1-12.
CrossRef - Sampogna G, Di Vincenzo M, Giuliani L, et al. A Systematic Review on the Effectiveness of Antipsychotic Drugs on the Quality of Life of Patients with Schizophrenia. Brain Sci. 2023; 3(11): 1577.
CrossRef - Nazeer A, Calles J. Management of Adverse Effects from Atypical Antipsychotics. Curr Psychopharmacol. 2018;7(1): 22-35.
CrossRef
- D’Agostino A, Aguglia A, Barbui C, et al. Off-label long acting injectable antipsychotics in real-world clinical practice: a cross-sectional analysis of prescriptive patterns from the STAR Network DEPOT study. BMC Psychiatry, 2022; 22(1): 442.
CrossRef

