
Manuscript accepted on :18-09-2025
Published online on: 10-11-2025
Plagiarism Check: Yes
Reviewed by: Dr. Mehdihasan Ijubhai
Second Review by: Dr. Feng Li
Final Approval by: Dr. Prabhishek Singh
Nandala Thippa Reddy Ravi Kumar1* , Lingala Syam Sundar2, Madhuri Desai3 and Hiren Mewada4
, Lingala Syam Sundar2, Madhuri Desai3 and Hiren Mewada4
1Department of CSR, Greenko Energies Foundation, Hyderabad, India.
2Department of Mechanical Engineering, College of Engineering, Prince Mohammad Bin Fahd University, Al-Khobar, Saudi Arabia.
3Department of Community Medicine, Information and Health Decision Sciences (MEDCIDS), Faculty of Medicine of the University of Porto, Porto, Portugal.
4Department of Electrical Engineering, College of Engineering, Prince Mohammad Bin Fahd University, Al-Khobar, Saudi Arabia.
Corresponding Authors E-mail:nandalathippareddyravikumar@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/3286
Abstract
Restorative dentistry has completely changed as a result of dental implants, which have improved the consistency and durability of treatment for edentulism and tooth loss. In order to promote osseointegration and guarantee optimal function and aesthetics, the intrinsic properties of the biomaterials utilized are therefore intrinsically linked to the effectiveness of dental implants. The increasing awareness of oral wellness has led to a great deal of study on dental diagnostic and therapy techniques. Dental biomaterials like polymers, metals, and acrylic resins are crucial for restoring teeth damaged by diseases or accidents as a consequence of several studies in this field. Ceramics provide a unique characteristic in contrast to other biomaterials like metals or polymers. Because of their high intrinsic strength, materials like zirconia and alumina are suitable for biological applications such as artificial joints or dental implants. They also exhibit exceptional biocompatibility, which reduces the likelihood of negative side effects or inflammation. Certain ceramics such as bioactive glasses and hydroxyapatite, even promote tissue regeneration and integration. Furthermore, due to their versatility, they can be carefully created and molded to highlight particular qualities. Although yttria-stabilized tetragonal zirconia has exceptional mechanical and biocompatibility qualities, low-temperature deterioration raises questions about its long-term durability. In order to improve the robustness and dependability of biomedical applications, scientists have created improved oxide-based materials including alumina-zirconia composites and non-oxidic ceramics like silicon nitride. Emphasized the latest developments in ceramic dental implants in this study; detailed examples and uses of several ceramic-based materials, such as zirconia, alumina, and cellulose are given.
Keywords
Abutment teeth; Biomaterial; Ceramic implants; Crown; Extraction; Osseointegration
Download this article as:| Copy the following to cite this article: Kumar N. T. R. R, Sundar L. S, Desai M, Mewada H. Utilization of Biomaterials for Dental Implant Applications: A Comprehensive Review. Biomed Pharmacol J 2025;18(4). |
| Copy the following to cite this URL: Kumar N. T. R. R, Sundar L. S, Desai M, Mewada H. Utilization of Biomaterials for Dental Implant Applications: A Comprehensive Review. Biomed Pharmacol J 2025;18(4). Available from: https://bit.ly/4p4RO0l |
Introduction
Osseointegration was first introduced, dental implant has been changing all the time to improve success and long-term survival rates. It has changed the way oral rehabilitation is done for conditions like periodontal and dental disease, which has led to better performance and quality of life. Periodontal and tooth repair has been done in a number of ways, such as with dental implants, removable dentures, and fixed prostheses. But as the number of people who need dental implants has grown, there have been problems in the center. One thing that can make it more likely for a dental implant to fail is immune-inflammatory reactions like peri-implantitis. It slows down tooth restoration by breaking down peri-implant tissue and causing inflammation of the mucosa.
There have been many attempts to treat peri-implantitis, but none of them have been successful in keeping the problem under control. Because of these problems in the clinic, dental implants need to be made that might be able to kill bacteria. A good tooth implant should be biocompatible, look good, make it harder for plaque to stick to it, and have surfaces that kill bacteria. Furthermore, it should be mechanically stable and not rust or wear down easily.1 Titanium and its alloys are generally thought to be the best materials for dental implants because they are biocompatible and have good mechanical qualities. But the biggest worry about dental implants is that they might release metals ions when they corrode. These ions could cause immune system reactions in the tissue around the implant, which would then raise failure.2
Changed the concept of planting material that don’t use metal, and ceramic dental bio-materials like ZrO2 and Al2O3 have been introduced as a possible option to material. ZrO2 doesn’t allow the plague to grow.3 However, ZrO2 tooth implants can lead to peri-implantitis, and their bioinertness often makes it harder for them to integrate with the body. The biocompatible ceramic could be used to make tooth implants and fake crowns. A lot of works on ceramic materials, but there isn’t a single piece that gathers the most important studies to make a full study on the material’s effects and how it can be used to restore bone and teeth. Because of this, this review paper talks about the most current research on ceramics and cellulose for dental restoration. Our review aims to helps the researchers to understand present state of considering ceramics and cellulose for dental restoration materials. We hope that this will help this field move forward to improve people’s better life who have teeth problems.
The current age, which was characterized by the discovery of titanium’s compatibility with bone, evolved from earlier dental implant attempts that employed crude materials with low success rates. Modern dental implantology produces more long-lasting and visually beautiful results thanks to improved materials, digital planning, and increased success rates. The earliest dental implants date back to the Mayan civilization, about 600 A.D., when archaeologists found sculpted stone and seashell fragments hammered into the jawbone to replace lost teeth. European practitioners experimented with materials like as porcelain, platinum, and gold during the 18th and 19th centuries. The first metal “screw” style implants were made in the early to mid-20th century using iridio-platinum with a soldered gold crown and a cobalt-chromium alloy called Vitallium. The field was revolutionized by the Swedish orthopaedic surgeon Per-Ingvar Brånemark, who discovered osseointegration, which is the process by which titanium can fuse with living bone tissue. Fig. 1 discusses the history of dental implants. Photograph of damaged tooth and the replace tooth with biomaterial is shown in Fig. 2. Various kind of dental implant materials are mentioned in Fig. 3.
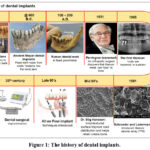 |
Figure 1: The history of dental implants. |
 |
Figure 2: Photograph of damaged tooth and replaced tooth. |
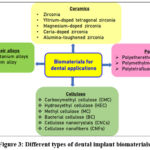 |
Figure 3: Different types of dental implant biomaterials. |
Dental implant specifications
Implant dental was surgical part which put into alveolar bone to hold dental prosthesis, such as a crown, an abutment, or a removable denture. In this case, the way of processing, biocompatibility, and osseointegration are very important. Biocompatibility is made up of two parts: biological (tissue and immune response) and material response (chemical and physical qualities), both of which affect how well the dental implant works. So that the dental implant works, it’s important that the peri-implant tissue and the implant’s surface come into direct touch with each other.4,5 The dental implant and the host tissue have several complex interfaces. These include, (i) the sub-gingival interface between the implant and bone, (ii) the trans-gingival soft tissue interface between the implant neck and the gingiva, and (iii) the supra-gingival and trans-gingival interfaces between the implant abutment, the oral cavity, and saliva.
Features like hydrophilicity, roughness, and topography can speed up osseointegration of dental implants,6 which can affect how stable and successful the implant is in the long run. In this way, the osteogenic potentials are the first and most important step in osseointegration. Different cells under soft tissue contact is necessary for attaching the gums to the teeth and making sure the gums seal tightly.7 Also, bacterial growth was main reasons why peri-implantitis happens. Inflammatory response can stop osseointegration and lead to bone loss, which means the tooth implant doesn’t work. So, the contact needs to be able to stop the formation of biofilm by making it hard for bacteria to stick to it and killing bacteria. If the binding tension is above 30 mN/m, the surface is hydrophilic. If it is below 30 mN/m, the surface is hydrophobic.8 We found that surfaces with a hydrophilicity between 40 and 70 are best because they work well with cells and body fluids. It is known that osseointegration works best with tooth implants that are hydrophilic and have an uneven surface.9 It is possible for the rough surface to improve mechanical coupling and lower the risk of implants. For these two factors to be balanced, surface roughness between 1 and 2 m was said to be important.10 To do this, the tooth implant’s surface should be hydrophilic, have the right amount of roughness, and be able to kill bacteria to help it fuse with the bone and speed up the healing process.
Ceramic based biomaterials for dental implants
In the past thirty years, all-ceramic restorative dentistry equipment has come a long way. This is mostly because more and more people want repairs that don’t use metal. Newer techniques used in traditional dentistry are heat pressing, slip casting, and CAD-CAM. When it comes to rigid structure, all ceramics have a range of 35 to 99 vol%, which is higher than metal ceramics. It makes sense that those materials with more crystallization would have better mechanical qualities, like being harder and less likely to wear down. This faster rate of crystallization has been used in a lot of different ways to make things stronger and harder to wear. Some examples are strain conversion and crystal strengthening. The zirconia ceramic based dental implant materials are provided in Fig. 4.
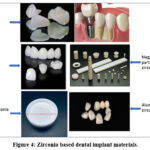 |
Figure 4: Zirconia based dental implant materials. |
Zirconia
Zirconia is now a good material that could someday be used instead of titanium, which is the best material for dental implants. zirconia, also written as ZrO2, has three different solid forms: monoclinic, cubic, and tetragonal. It is thought that the tetragonal and cubic phases are the most stable and are best for use in implants. A tetragonal and cubic phage is made by adding many showing agents, such as yttrium, cerium, calcium, and others. Some of the zirconia ceramics that are utilized in dentistry are yttrium-doped tetragonal zirconia polycrystals (3Y-TZP), partly stabilized zirconia doped with magnesium cation, zirconia-toughened alumina (ZTA), and zirconia doped with cerium. There are many zirconia-containing ceramics systems on the market right now, but many of them are only used for dental implants.
Yttrium-doped tetragonal zirconia
Due to its various advantages, including a reduced requirement for tooth preparation, a decreased risk of chipping, and ease of handling, zirconium dioxide partly stabilized by yttria (Y-PSZ) materials are frequently utilized in dental restoration. Because of its many beneficial qualities, including being stronger, less radioactive, more resistant to wear, more able to withstand damage, and less reactive to chemicals, the three mol% yttria stabilized tetragonal zirconia polycrystal (3Y-TZP) type of Y-PSZ is frequently used to create dental prosthetics.11,12 These characteristics make 3Y-TZP an excellent option for tooth restorations due to its long lifespan. 3% stabilized zirconia contains crystallites with a load of 49.05 N and sizes ranging from 5.8 to 8.0 nm. Its mechanical strength is increased by its fracture toughness, which varies from 4.6 to 6.4 MPa/m1/2 for 3% stabilized. For instance, conventional monolithic Y-PSZ may provide fracture resistance ranges of 3.5 to 4.5 MPa/m1/2 and bending ranges exceeding 1000 MPa. This enables the creation of restorations with thin walls and numerous small components.13
The yttria proportion can be altered to 4%, 5%, 8%, or 16%. This allows you to adjust the grain size, which alters the materials’ mechanical characteristics and enlarges them for various dental applications.14 To determine how dental implants bond with bone in the mouth, Kalinnikova et al.15 conducted an in vivo investigation. Pandoleon et al.16 examined the effects of Y-TZP implant abutment material on the adhesion and survival of human gingival fibroblasts in order to determine whether these materials are biocompatible. Akarsu et al.17 explain the addition of MoCl3 and NiCl2 to three mol% yttria-doped zirconia (3Y-TZP) in their publication. They cultivate l929 fibroblast cell lines on the material’s surface in order to analyse it in a lab. Cell viability and growth tests revealed that none of these specimens exhibited color-related cytotoxicity. Tests using confocal laser scanning microscopy revealed that every model interacted well with laboratory cells. All models exhibited improved cell attachment, adhesion, and proliferation, according to a study conducted with a scanning electron microscope.
Cone beam computed tomography (CBCT) was utilized by Warren et al.18 to examine the metal object composed of ceramic and titanium dental implants. Two human skulls with missing teeth were implanted, and pictures were obtained using low-dose 180 and standard-dose 360 CBCT scans. The metal size object was determined by considering the pixel intensity data. Additionally, a modified Likert scale was employed for quantitative assessment. For titanium implants, the average pixel level was found to be between 123.5 and 507, while for ceramic implants, it was between 500 and 1088.5. According to a qualitative analysis of CBCT images, titanium implants are less likely than ceramic implants to have metallic flaws.
Magnesium-doped zirconia
One possible dopant in the zirconium system is magnesium (MgO). It is regarded as the most interesting dopant because, depending on its history of heat treatment, it can result in remarkable mechanical properties and highly complex microstructures. The most often used composition in the industry to produce magnesium partially stabilized zirconia (Mg-PSZ) is magnesium with equilibrium at 8–10 mol%.19 The grain size of Mg-PSZ is 13.4 μm, and its fracture strength is 6.29 to 0.18 GPa. At 1700 oC, the sintered specimen’s Vickers hardness is 13.5 GPa.20 The current study demonstrates Mg-PSZ’s higher resilience to environmental breakdown when compared to Y-TZP. In orthopaedic implants, particularly total joint arthroplasty, magnesium-PSZ is utilized. Cho et al.21 demonstrated the physical and mechanical characteristics of Mg-PSZ as well as its production using the spark plasma method.
Ceria-doped zirconia
Ceria doped TZP (Ce-TZP) is an alternative material that has better fault tolerance and fracture toughness (more than 10 MPa/m1/2) than Y-TZP. Due to the absence of oxygen gaps, Ce-doped zirconia has the advantage of being resistant to aging at low temperatures, which could make the fabrication of intricately tailored components easier. Because of comparatively low strength (400–600 MPa) caused by substantial grain boundary mobility in normal sintering procedures around 1400 ◦C, which causes huge grain size to surpass several microns, pure Ce-TZP has not been employed very often. When 12% Ce is present, Zr exhibits improved fracture resistance of 11.96–1.31 and 11.43–0.45 MPa/m1/2, as well as greater flexural strengths of 76.06–770.90 and 61.14–601.72 MPa. Coprecipitation, spark plasma sintering, and spark plasma sintering were used to create Ce-doped zirconia. Single-layer silver (Ag) and cerium-stabilized zirconia (Ce-SZ) nanocoating was created on titanium substrates using the co-evaporation technique and the electron beam physical vapor deposition (PVD) method.
Bejugama et al.22 investigated the niobium and Ce-doped zirconia (Nb-CSZ)-based implants’ cytotoxicity, cellular response, and in vitro behaviour. The results showed that Nb-CSZ does not respond negatively, encourages cell adhesion and proliferation, and shows a strong resilience to low-temperature deterioration. Ceria and calcium-doped zirconia’s mechanical characteristics were described by Tovar-Vargas et al.23,24. They get to the conclusion that the change in grain shape and size reduction in 10Ce-1CaO composites and 10Ce-1CaO-5Al2O3 improves their strength and microhardness when compared to 10Ce-TZP. When compared to the average hardness and strength of 10Ce-TZP ceramic (500 MPa and 6 GPa) improvement in the characteristics were seen in compositions, but for 10Ce-1CaO-5Al2O3 (739 MPa and 10.2 GPa). Additionally, none of these composites deteriorate with age.
The preclinical investigation of Ceria-TZP-doped composite dental material in dogs was assessed by Chacun et al.25 Six beagle dogs had their mouths fitted with 24 ceramic and 24 titanium tooth screws that had been etched using sandblasting. Four- and thirteen-weeks following implantation, a histological assessment of the surrounding tissue was conducted. Histological studies revealed that the inflammatory tissue response to titanium implantation was similar to that of ceramic implants (Fig. 5). The ceramic and titanium dental implant groups’ bone to implant contact (BIC) values did not alter.
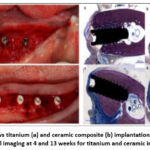 |
Figure 5: Left shows titanium (a) and ceramic composite (b) implantation. Right shows the histological imaging at 4 and 13 weeks for titanium and ceramic implants.25 |
Alumina-toughened zirconia
Tiny alumina particles in a delicate zirconia matrix make up the ceramic composite known as Alumina-toughened zirconia (ATZ). For structural purposes, alumina is a great ceramic material. In a minipig model, Schierano et al.26 assess the ATZ in vivo for use in dentistry. Using histology and mRNA expression, a minipig animal model evaluated bone repair at different points in time (8, 14, 28, and 56 days). According to the histological investigation, the ATZ and titanium subgroups experienced comparable cellular remodeling of bone fragments, with the peak of activity taking place eight days post-implantation. In comparison to titanium dental implants, the 3D study that measured the bone surrounding the implant at 56 days consistently revealed a denser bone matrix across the ATZ, particularly in the medial area. Femtosecond laser micro structuring of alumina-toughened ceramic zirconia for dental implant surfaces improves preosteoclast attachment, MC3T3-E1 cells, according to Carvalho et al.27.
The mechanical characteristics of ceramic zirconia that has been hardened with alumina for dental implants were assessed by Tang et al.28. They evaluated the high sinter ability (99.2%) of monolithic Al2O3 and Al2O3-reinforced 3Y-TZP zirconia composites. According to the linear rule for mixtures, Young’s modulus decreased as the concentration of 3Y-TZP rose. It was discovered that the content of 3Y-TZP increased linearly with hardness due to the compression surface stress field produced by the stress-dependent phase change. ZTA zirconia composite materials produce residual hoop compressive strain, which is probably what gives them their improved strength, fracture toughness, and fissure deflection intensity. The histological and biomechanical characteristics of moderately rough ATZ dental implants in rat femoral bone was assessed by Kohal et al.29. Each group’s histological specimens showed signs of immune cell inflammatory infiltration, according to histological examination. Bone-to-implant contact was noted in each cohort. A rough ATZ surface can be seen under higher magnification to show bone growth coming from the implant surface, including cells, as well as bone development from nearby regions toward the implant surface.
Metal and metal alloy implants
Titanium and titanium alloys
William Gregory made the discovery of titanium, the ninth most plentiful metal, in 1791. In its pure state, it manifests as a silver metal with special physical-chemical properties, including high strength (590 MPa) and low density (4506 g/cm3).30 Rapid reactions between titanium and oxygen result in the oxide layer creation over metals surface, which protects it from corrosion. Usage in sports, jewellery, pigments, marine equipment, aircraft, and medicine are just a few of the many topics for which research is being conducted on this metal. Compared to stainless steel and chromium-cobalt, titanium, and their alloys were recognized as nontoxic and huge biocompatible for the dental sector.31 They also work well with magnetic resonance imaging, and computed tomography. Production of dental implants and prostheses is based on these titanium biomaterials.
Titanium oxide was most frequently considered material in dental implant research because of the various characteristics seen in titanium forms. TiO2 is created when titanium metal reacts with air to form hydroxyl and hydroxide groups, which increases the metal’s resistance to corrosion. Titanium is granted its biocompatibility by this oxide layer. In ambient settings, TiO2 exists in three distinct crystalline forms: rutile, brookite, and anatase. Synthesized metal heat treatment allows for the phase transitions. Although rutile and anatase, which both exhibit octahedral geometry, were easily made, brookite, which is structured in orthorhombic geometry challenging to grab.32
The rutile and anatase phases differ from one another because of aberrations in the octahedral structure that TiO6 forms. These structures can be created using a variety of techniques, including hydrothermal and electrochemical ones. Consequently, one of the desired phases will occur preferentially when the physicochemical parameters of the synthesis are altered. Therefore, the phase has a direct impact on how well its dental applications work. Anatase is most frequently utilized in dental implants since it is frequently linked to applications that call for osseointegration.
Titanium is currently the most often used material in dental implant manufacturing, while other materials, such as ceramics or polymers, are also utilized depending on their chemical makeup. There are currently six varieties of titanium available as biomaterials for implants. Of these, two are titanium alloys (Ti-6Al-4V and Ti-6Al-4V extra low interstitial alloys) and four are grades of commercially pure titanium (CPTi), which ranges from 98 to 99.6% pure titanium (Grades I, II, III, and IV). The ductility, strength, and corrosion resistance of these grades vary.
The material of biocompatible with sufficient strength, toughness, and withstand to corrosion and fracture is suitable for making dental implants. These characteristics typically have to do with the metal’s O2 debris. Grade IV CpTi was frequently utilized form of for implants due to its large O2 availability (0.4%) and, as a result, superior mechanical strength.
Titanium alloys were first developed as a possible metallic material for the biomedical sector with the goal of lowering the cost of manufacturing devices. Alphas stabilizers, which include Al, O2, N2, C, and carbon, and betas stabilizers, which include vanadium, Fe, Ni, and Co, make up the majority of the alloying elements that are added to Ti. Consequently, there are three structural forms of dental titanium alloys: , , or , which is a combination of the two. In dental applications, the most common alloy is Ti-6Al-4V, sometimes known as the combination. It is extremely robust and corrosion-resistant, with 6% Al and 4% vanadium. The Al stabilizes the α-phase. It reduces the alloy’s density and boosts its strength.
Conversely, vanadium stabilizes the -phase.33 Compared to α stabilizers, beta stabilizing components are costlier.34 Therefore, the industry’s current demand is to replace the prevalent β stabilizers with less expensive alternatives. Due to its strength and affordability, iron is the element most frequently utilized in place of the β-stabilizing element in this regard. High temperatures, however, have been shown to encourage the development of inter-metallic product like TiFe or Ti2Fe, adversely affect ductility and mechanical characteristics of alloys. Because it affects how the titanium implant interacts with the bone, its surface is significant. The oxide TiO2 makes up the surface of the primary dental implant materials (CpTi and Ti-6Al-4V), providing excellent corrosion resistance and a clinical victory of 99%.
Despite being the most often utilized and significant α stabilizer, aluminium has been shown to make titanium alloys challenging to work with and machine. According to reports, Ti-6Al-4V has good biological uptake.35 Small amounts of vanadium and aluminium are eventually liberated, though, and this could trigger an inflammatory reaction. Vanadium is cytotoxic and can cause allergic reactions, whereas aluminium prevents bone mineralization, resulting in bone deformity. For this reason, CPTi is used increasingly frequently to make dental implants. Vanadium-free alloys like Ti-6Al-7Nb and Ti-5Al-2.5Fe have been created to avoid these biological issues. Additionally, alloys made of non-toxic elements including Pd, Zr, Ta, and Nb are being developed.
Binary composition of 83-87% of Ti, and 13-17% Zr (Roxolid®, Straumann, Basel, Switzerland) is the basis for a recently created novel dental alloy. In comparison to CpTi and Ti-6Al-4V, were reported to have superior tensile and fatigue strength properties. Following insertion in various animal models, in vivo investigations have demonstrated bone integration of threaded zirconia implants that is equivalent to Ti.36
Ceramic implants were developed for dental implants because titanium is unsightly in the frontal region. In order to enhance osseointegration, it was first applied for covering material for metal implants. Dental implants have been coated with a variety of ceramic materials in recent years. Numerous medical, orthopaedic, and dental applications make extensive use of inert ceramics like zirconium oxide and aluminium oxide, as well as bioactive ceramics like calcium phosphates and bio glasses.
Cobalt chromium alloy
The excellent wear resistance of Co-Cr alloys is a second crucial feature for their application in restorative materials. Furthermore, commonly known that some metals are harmful to human health. Similarly, it is crucial to ascertain and then validate if the low wear characteristics of Co-Cr alloys are associated with a lower level of toxicity to the human body. Numerous investigations have been conducted on Co-Cr alloys used in hip and knee replacements, where exposure levels may be significant.37,38
In order to continuously enhance current alloys and enable their optimization through the inclusion of new metals, wear is still a phenomenon that is extensively researched. However, a recent analysis in the particular field of dentistry combines the key factors related to restorative material wear. Naturally, the toxicity that the discharged particles may later produce is connected to all of these-research on the wear levels of biomedical equipment. Concerns regarding particle size produced by the wear of implants and prostheses made of (Co–Cr) alloys have surfaced more recently. Size of wear particles released by metal-on-metal (MoM) hip implants under normal and edge-loading circumstances was investigated by Kovochich et al.39
Stainless steel
SS316L is frequently used in joint replacement procedures, including hip and knee replacements. For example, because of its strength and resistance to corrosion, SS316L is frequently used in the femoral components (a metal stem) of hip replacements. To support body weight and permit movement, these implants need to be extraordinarily robust. Additionally, SS316L is widely utilized in the production of screws and bone plates, which are necessary for the internal fixation of fractures.40 Metal and metal alloy based dental implants image is provided in Fig. 6.
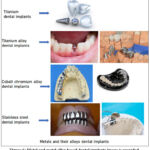 |
Figure 6: Metal and metal alloy based dental implants image is provided. |
Polymers based dental implants
Polyetheretherketone (PEEK)
Polyetheretherketone (PEEK) is a synthetic polymer with many applications owing to its exceptional characteristics that serve human needs. These applications encompass its utilization as a biomaterial for dental implants, prosthetic materials, abutment materials, post and core materials, crowns, and frameworks for detachable partial dentures. Due to its extensive applications, PEEK is regarded as a comprehensive solution for dentistry. Minimizing marginal bone loss during functional loading is essential for the effectiveness of dental implants.
Enamel erosion or tooth attrition resulting from dental prosthetics and restorations is a prevalent phenomenon. The wear caused by any dental restoration must not surpass physiological wear values. Consequently, an appropriate material must be chosen that offers stability and strength, nearly resembling the hardness of enamel, while minimizing excessive abrasion to the enamel structure. Parekh et al.41 analysed the stresses and found PEEK abutments can help to reduce stress on the abutment compared to other materials because of its elastic modulus is closer to that of natural bone than titanium, allowing for better load distribution and less stress transferred to the bone.
Polymethylmethacrylate (PMMA)
Dental implants are among the many uses for the polymer polymethylmethacrylate (PMMA) in dentistry. PMMA is commonly utilized in the production of temporary or provisional crowns, denture bases, and as a material for milled or 3D-printed prototypes for implant-supported restorations, despite not being a direct implant material. Additionally, it is utilized to anchor implants during corrective surgery and in bone cement for orthopaedic and dental applications.
Although materials containing methacrylate polymer are currently in use, the sensitivity of methacrylate materials is starting to become a major concern in dentistry. Compression-molded, heat-cured poly(methyl methacrylate) dental prostheses can be produced economically and sustainably in a microwave. Sun et al.42 prepared the zirconia/PMMA composites for dental applications and found that the mechanical properties of 3Y-TZP/PMMA and 5Y-PSZ/PMMA composites were tuneable to closely match to human enamel, and showed the 3Y-TZP/PMMA and 5Y-PSZ/PMMA composites showed proper machinability for chairside CAD/CAM dental restorations.
Polytetrafluoroethylene (PTFE)
Dental implants use polytetrafluoroethylene (PTFE), also referred to as Teflon, for a number of reasons, chief among them being the protection of implant components, the sealing of screw access holes, and the function as a barrier material. It is prized for its ease of manipulation and removal, biocompatibility, and capacity to stop bacterial leakage. Moráguez, and Belser43 prepared polytetrafluoroethylene (PTFE) tape and used as seal the screw access channel to protect the screw head of the abutment and crown screw in implant-supported restorations.
Carbonell et al.44 review paper explains about the expanded polytetrafluoroethylene (e-PTFE) has been considered as a successful membrane barrier for regeneration procedures. When this material exposed to the oral cavity, its high porosity increases the risk of early infection, which can affect surgical outcomes. Fig. 7 indicates the polymer based dental implants.
 |
Figure 7: Polymer based dental implants. |
Cellulose and its derivatives
The most prevalent natural polymer on Earth, cellulose, is mostly found in plant cell walls. The β-D-glucose units that make up this linear polymer are joined by β(1→4) glycosidic linkages. Cellulose and its derivatives are appropriate for a number of uses, including dentistry, because of their mechanical qualities, biocompatibility, and biodegradability (Zheng et al.45). There are numerous beneficial dental uses for natural cellulose that is made straight from natural sources like cotton and wood (Ye et al.46).
Additionally, there are cellulose derivatives with distinct properties for particular dental applications, such as carboxymethylcellulose (CMC), hydroxide-ethyl cellulose (HEC), methylcellulose (MC), and bacteria cellulose (BC) (Raut et al.47). Cellulose composites and nanomaterials, including cellulose nano crystals (CNCs) and cellulose nanofibers (CNFs), have become significant materials in dentistry due to their enhanced mechanical properties, biocompatibility, and antibacterial activity (Zhuorui et al.48). Overview of the dental applications of cellulose is shown in Fig. 8. The overview of the cellulose for the dental applications are mentioned in Table 1.
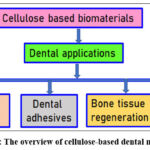 |
Figure 8: The overview of cellulose-based dental materials. |
Table 1: Different cellulose for the dental applications.
| Author | Type | Description | Applications |
| Baranov et al.49 | Carboxymethyl Cellulose (CMC) | Derivative that dissolves in water and is produced by adding carboxymethyl groups to the backbone of cellulose. | Utilized to create hydrogels, films, and coatings for use in medications, dental adhesives, and implant coatings, among other applications. |
| Cui et al.50 | Hydroxyethyl Cellulose (HEC) | A non-ionic, water-soluble form of cellulose that can thicken and stabilize materials. | Utilized in the creation of dental adhesives and as a binder and thickening agent in dental impression materials. |
| Ali et al.51 | Methyl Cellulose (MC) | Cellulose derivative that dissolves in water and gels when heated. | Utilized in dental applications, including scaffolds for tissue engineering and impression materials. |
| Janmohammadiet al.52 | Bacterial Cellulose (BC) | Bacterial extracellular polysaccharide, such Gluconacetobacter xylinus. | Used in dentistry for things like tooth implants, bone regeneration, and building scaffolds for tissue engineering. |
| Hasan et al.53 | Cellulose Nanocrystals (CNCs) | Nanoparticles that look like rods and are made by breaking down cellulose with acid. | Added to tooth composites and adhesives to make them stronger, more biocompatible, and better at killing germs |
| Klemm et al.54 | Cellulose Nanofibers (CNFs) | Fibrillated cellulose products with high aspect ratios that have been separated by chemical or mechanical means. | To make them stronger, more biocompatible, and more bioactive in areas like tooth composites, drug delivery systems, and tissue engineering scaffolds. |
The main consideration for dental implant requirements is not age, but rather the attainment of skeletal maturity in younger patients, as well as the maintenance of sufficient bone density and general health in all age groups. Although there is no upper age limit, older people may have to deal with more medical concerns and may experience delayed recuperation. Waiting until the jawbone is fully matured is essential for people under the age of eighteen in order to avoid problems like shifting implants.
Emergence of different types of dental biomaterials
Growing clinical demands for restorative, regenerative, and aesthetically pleasing therapies have fueled the development of a variety of dental biomaterials, such as polymers, ceramics, composites, and bioactive glasses. Modern dental biomaterials, which are fueled by developments in material science and nanotechnology, provide improved biocompatibility and performance, enabling the creation of long-lasting, aesthetically pleasing restorations and the replacement of lost tissues. These materials include naturally occurring substances like collagen and chitosan as well as robust alloys like titanium and zirconia. Research on tissue engineering and nanomaterial creation is still ongoing.
Metals: For dental implants and restorations, materials with mechanical strength and biocompatibility, such as titanium alloys and other metal alloys, are utilized.
Ceramics: These comprise zirconia and other bioactive ceramics that offer biocompatibility and good aesthetics for restorative applications, crowns, and bridges.
Polymers: Used in fillers, adhesives, and regenerative scaffolds, this large class include resin composites, bioactive polymers, and natural polymers like chitosan.
Composites: These materials, like resin composites that add fillers to improve strength and durability, combine several ingredients to provide a synergistic effect.
Antimicrobial properties of dental implants
The long-term viability of dental implants depends on specialized surfaces that prevent bacterial adhesion and biofilm development; this problem is solved by combining antimicrobial coatings and physical surface modifications. Dental implants have very little intrinsic antibacterial activity. Typical tactics include coatings infused with silver, copper, or zinc, altering the physical and chemical properties of the implant, or developing bacterial-repelling nanostructured surfaces. Through the inhibition of bacterial colonization and biofilm formation, these alterations seek to avoid peri-implantitis, the main cause of implant failure. Bacterial growth is inhibited when bioactive glass is surface treated with different chemical agents or materials. Biocompatibility can be enhanced and bacterial adhesion decreased by putting organic coatings on polymers, antimicrobial peptides, or other biomimetic films.
Conclusion
Dental implants and abutments made of zirconia are becoming more and more popular since they have clear benefits over conventional titanium. Zirconia is a promising substitute due to its superior fracture toughness (11.96 ⁶ 1.31 and 11.43 ⁶ 0.45 MPa/m1/2, Vickers hardness of 13.5 GPa), white color, decreased bacterial adherence, and comparable osseointegration to titanium (fracture toughness 7.07 to 10.10 MPa/m1/2, Vickers hardness of 3.24 GPa). With improvements in hardness of over 13.5 GPa, fracture toughness of over 11.96 MPa/m1/2, osseointegration, and bioactivity, this review highlights the bright future of zirconium and its implants. Dental implants’ bioactivity is strengthened for better in vivo and in vitro results by using bioactive materials (HA, PDA, calcium phosphate) and chemical alterations (acid etching, grit blasting, UV therapy) to improve osseointegration. Even with significant advancements, there are still unanswered questions, especially about the biological reactions of the implants, such as local cytotoxicity, fibrotic tissue response, and immunological rejection. To advance these materials as viable dental implants, more pre-clinical research is required to fully address some of these concerns. It is anticipated that the next generation of zirconia implants will be altered to remove all of the restrictions associated with patient-specific implant integration.
The SS316L stainless steel, which shows how important it is for biomedical uses in changing implant surfaces so that cells stick to them and they don’t grow germs. SS316L is very strong, doesn’t rust, and is better at being compatible with living things. It is a material that is commonly found in many medical implants used in orthopaedics, dentistry, and heart health.
Given improvements in healthcare and the worlds people’s increased life expectancy, biomedical implants have very minor negative influence on host tissues will develop, but those are almost negligible. Despite being widely used and helping with osseointegration, traditional materials such as Ti or its alloys were a number of disadvantages, such as metal ions and debris, metallosis, or darkening of the implant area, and poor visibility and local area stress shielding.
Because of their capacity to strengthen mechanical characteristics, encourage tissue regeneration, and increase osseointegration, biomaterials are becoming more and more important in dental implants. Opportunities include 3D-printed composites with improved biocompatibility, targeted drug administration, and anti-infective qualities, as well as novel bioactive coatings and nanostructured surfaces. By addressing the drawbacks of conventional materials, these advancements hope to increase long-term stability, enhance patient happiness, and lessen problems like peri-implant infections.
Acknowledgement
The authors acknowledge the Prince Mohammad Bin Fahd University.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Authors’ Contribution
- Syam Sundar: Conceptualization, Methodology, Writing – Original Draft.
- Madhuri Desai: Data analysis, Data Collection.
- Hiren Mewada: Analysis, Validation.
- Nandala Thippa Reddy Ravi Kumar: Writing – Review & Editing
References
- Raza SM, Khurshid Z, and Zafar MS, et al. Silicon nitride (SiN): An emerging material for dental implant applications. Dental Implants. 2020; 287–99.
CrossRef - Chaturvedi T. An overview of the corrosion aspect of dental implants (titanium and its alloys). Indian J. Dental Research. 2009; 20(1): 91.
CrossRef - Hashim D, Cionca N, and Courvoisier DS, et al. A systematic review of the clinical survival of zirconia implants. Clinical Oral Investigations. 2016; 20(7): 1403–1417.
CrossRef - Albrektsson T, Brånemark PI, and Hansson HA, et al. Osseointegrated titanium implants: requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthopaedica. 1981; 52(2): 155–170.
CrossRef - Jiang X, Yao Y, and Tang W, et al. Design of dental implants at materials level: an overview. Biomed Material Research. 2020; 108(8): 1634–1661.
CrossRef - Ballo AM, Omar O, and Xia W, et al. Dental implant surfaces-Physicochemical properties, biological performance, and trends. Implant Dentistry-A Rapidly Evolving Practice. 2011; 1: 19–56.
- Rupp F, Liang L, and Geis-Gerstorfer J, et al. Surface characteristics of dental implants: a review. Dental Materials. 2018; 34(1): 40–57.
CrossRef - Gittens RA, Scheideler L, and Rupp F, et al. A review on the wettability of dental implant surfaces II: biological and clinical aspects. Acta Biomaterialia. 2014; 10(7): 2907–2918.
CrossRef - Sawase T, Jimbo R, and Baba K, et al. Photo-induced hydrophilicity enhances initial cell behavior and early bone apposition. Clinical Oral Implants Research. 2008; 19(5): 491–496.
CrossRef - Le Guehennec L, Soueidan A, and Layrolle P, et al. Surface treatments of titanium dental implants for rapid osseointegration. Dental Materials. 2007; 23(7): 844–54.
CrossRef - Ji M, Xu J, Yu D, Chen M, El Mansori M. Influence of sintering temperatures on material properties and corresponding milling machinability of zirconia ceramics. J Manuf Processes. 2021; 68: 646–656.
CrossRef - Ji M, Xu J, and Chen M, et al. Enhanced hydrophilicity and tribological behavior of dental zirconia ceramics based on picosecond laser surface texturing. Ceram International. 2020; 46(6): 7161–7169.
CrossRef - Kengtanyakich S, and Peampring C. An experimental study on hydrothermal degradation of cubic-containing translucent zirconia. Advanced Prosthodontics. 2020; 12(5): 265-272.
CrossRef - Park HW, Cho E, and Zou Y, et al. Synthesis of yttria-stabilized zirconia nanospheres from zirconium based metal-organic frameworks and the dielectric properties. Nanomaterials. 2022; 13(1): 28.
CrossRef - Kalinnikova E, Sadovnikova M, and Rodionov A, et al. Analysis of the osseointegration process of dental implants by electron paramagnetic resonance: An in vivo study. Dentistry Journal. 2022; 10(2): 28.
CrossRef - Pandoleon P, Bakopoulou A, and Papadopoulou L, et al. Evaluation of the biological behaviour of various dental implant abutment materials on attachment and viability of human gingival fibroblasts. Dental Materials. 2019; 35(7): 1053–63.
CrossRef - Akarsu MK, Basar AO, and Sasmazel HT, et al. In vitro evaluation of tooth-colored yttria stabilized zirconia ceramics. Asian Ceramic Society. 2021; 9(4): 1457–65.
CrossRef - Warren EK, Vaddi A, and Tadinada A. A comparative evaluation of the metallic artifact generated by a ceramic dental implant and a titanium dental implant imaged on cone-beam computed tomographic scans: an ex vivo study. JADA Found Science. 2022; 1: 100007.
CrossRef - Yurdakul A, and Balci O. Effects of titanium diboride on the mechanical, tribological, and microstructural properties of alumina toughened co-doped (Y-Mg) stabilized zirconia composites. Advanced Composites and Hybrid Materials. 2021; 4: 415–434.
CrossRef - Soylemez B, Sener E, and Yurdakul A, et al. Fracture toughness enhancement of yttria-stabilized tetragonal zirconia polycrystalline ceramics through magnesia-partially stabilized zirconia addition. Science: Advanced Materials and Devices. 2020; 5(4): 527–34.
CrossRef - Cho J, Yang B, and Shen C, et al. Micromechanical properties and microstructure evolution of magnesia partially stabilized zirconia prepared by spark plasma sintering. European Ceramic Society. 2023; 43(3):1098–107.
CrossRef - Bejugama S, Chameettachal S, and Pati F, et al. In vitro cellular response and hydrothermal aging of two-step sintered Nb2O5 doped ceria stabilized zirconia ceramics. Ceram International. 2021; 47(2): 1594–1601.
CrossRef - Tovar-Vargas D, Roitero E, and Anglada M, et al. Mechanical properties of ceria-calcia stabilized zirconia ceramics with alumina additions. European Ceramic Society. 2021; 41(11): 5602–5612.
CrossRef - Tovar-Vargas D, Ferrari B, and Sanchez-Herencia AJ, et al. Low temperature degradation and mechanical properties of alumina reinforced ceria-zirconia by colloidal processing. European Ceramic Society. 2021; 41(2): 1459–1470.
CrossRef - Chacun D, Lafon A, and Courtois N, et al. Histologic and histomorphometric evaluation of new zirconia-based ceramic dental implants: A preclinical study in dogs. Dental Materials. 2021; 37(9):1377–1389.
CrossRef - Schierano G, Mussano F, and Faga MG, et al. An alumina toughened zirconia composite for dental implant application: in vivo animal results. BioMed Research International. 2015; 2015: 157360.
CrossRef - Carvalho A, Grenho L, and Fernandes MH, et al. Femtosecond laser microstructuring of alumina toughened zirconia for surface functionalization of dental implants. Ceramic International. 2020; 46(2): 1383–1389.
CrossRef - Tang D, Lim HB, and Lee KJ, et al. Evaluation of mechanical reliability of zirconia-toughened alumina composites for dental implants. Ceramic International. 2012; 38(3): 2429–2436.
CrossRef - Kohal RJ, Bachle M, and Renz A, et al. Evaluation of alumina toughened zirconia implants with a sintered, moderately rough surface: An experiment in the rat. Dental Materials. 2016; 32(1): 65–72.
CrossRef - Nicholson JW. Titanium alloys for dental implants: A review. Prosthesis. 2020; 2: 11.
CrossRef - Shi H, Magaye R, and Castranova V, et al. Titanium dioxide nanoparticles: A review of current toxicological data. Particle and Fibre Toxicology. 2013; 10: 15.
CrossRef - Chen X, and Mao SS. Titanium dioxide nanomaterials: Synthesis, properties, modifications, and applications. Chemical Reviews. 2007; 107: 2891–2959.
CrossRef - Kolli RP, and Devaraj A. A review of metastable beta titanium alloys. Metals. 2018; 8: 506.
CrossRef - Fujii H, Fujisawa K, and Ijii M, et al. Development of low-cost high-strength Ti-Fe-O-N alloy series. Nippon Steel Technical Report. 2002; 85: 107–112.
- Ferraris S, Spriano S, and Pan G. Surface modification of Ti-6Al-4V alloy for biomineralization and specific biological response: Part I, inorganic modification. Material Science: Materials in Medicine. 2011; 22: 533–545.
CrossRef - Kohal RJ, Weng D, and Bächle M, et al. Loaded custom-made zirconia and titanium implants show similar osseointegration: An animal experiment. Periodontol. 2004; 75: 1262–1268.
CrossRef - Posada OM, Gilmour D, and Tate RJ, et al. CoCr wear particles generated from CoCr alloy metal-on-metal hip replacements, and cobalt ions stimulate apoptosis and expression of general toxicology-related genes in monocyte-like U937 cells. Toxicology and Applied Pharmacology. 2014; 281: 125–135.
CrossRef - Madl AK, Kovochich M, and Liong M, et al. Toxicology of wear particles of cobalt-chromium alloy metal-on-metal hip implants Part II: Importance of physicochemical properties and dose in animal and in vitro studies as a basis for risk assessment. Nanomedicine 2015; 11: 1285–1298.
CrossRef - Kovochich M, Fung ES, and Donovan E, et al. Characterization of wear debris from metal-on-metal hip implants during normal wear versus edge-loading conditions. Biomedical Material Research Part B Applied Biomaterials. 2018; 106: 986–996.
CrossRef - Benčina M, Kovač J, and Lakota K, et al. Chapter 3- Advancements and biocompatibility of stainless steel: Improved cell membrane adhesion and antibacterial properties. Advances in Biomembranes and Lipid Self-Assembly. 2024; 40: 33-53.
CrossRef - Parekh A, Doifode H, and Patil P, et al. Study on Polyether-ether-ketone (PEEK) dental implant, future alternatives to Titanium. International Conference on Advances in Mechanical Engineering (ICAME-2022). 2022; 1259: 012045.
CrossRef - Sun H, Tabrizian P, and Qambrani A, et al. Bio-inspired nacre-like zirconia/PMMA composites for chairside CAD/CAM dental restorations. Dental Materials. 2024; 40: 307-317.
CrossRef - Moráguez OD, and Belser The use of polytetrafluoroethylene tape for the management of screw access channels in implant-supported prostheses. The Journal of Prosthetic Dentistry. 2010; 103(3): 189-191.
CrossRef - Carbonell JM, SanzMartín I, and Santos A, et al. High-density polytetrafluoroethylene membranes in guided bone and tissue regeneration procedures: A literature review. J. Oral and Maxillofacial Surgery. 2014; 43: 75-84.
CrossRef - Zheng L, Li S, and Luo J, et al. Latest advances on bacterial cellulose-based antibacterial materials as wound dressings. Frontiers in Bioengineering and Biotechnology. 2020; 8: 593768.
CrossRef - Ye S, He S, and Su C, et al. Morphological, release and antibacterial performances of amoxicillin-loaded cellulose aerogels. Molecules. 2018; 23: 2082.
CrossRef - Raut MP, Asare E, and Syed Mohamed SMD, et al. Bacterial cellulose-based blends and composites: versatile biomaterials for tissue engineering applications. J. Molecular Science. 2023; 24(2): 986.
CrossRef - Zhuorui H, Hong Z, Jun-Hu C. Structure modification and property improvement of plant cellulose: based on emerging and sustainable nonthermal processing technologies. Food Research International. 2022; 156: 111300.
CrossRef - Baranov N, Popa M, and Atanase LI, et al. Polysaccharide-based drug delivery systems for the treatment of periodontitis. 2021; 26(9): 2735.
CrossRef - Cui X, Lee JJL, and Chen WN, et al. Eco-friendly and biodegradable cellulose hydrogels produced from low cost okara: Towards non-toxic flexible electronics. Scientific Reports. 2019; 9: 18166.
CrossRef - Ali A, Aziz T, and Zheng J, et al. Modification of cellulose nanocrystals with 2-Carboxyethyl acrylate in the presence of epoxy resin for enhancing its adhesive properties. Frontiers in Bioengineering and Biotechnology. 2022; 9, 797672.
CrossRef - Janmohammadi M, Nazemi Z, and Salehi AOM, et al. Cellulose-based composite scaffolds for bone tissue engineering and localized drug delivery. Bioactive Materials. 2023; 20: 137–163.
CrossRef - Hasan N, Rahman L, and Kim SH, et al., Recent advances of nanocellulose in drug delivery systems. Pharmaceutical Investigation. 2020; 50: 553-572.
CrossRef - Klemm D, Kramer F, and Moritz S, et al. Nanocelluloses: A New Family of Nature-Based Materials. Angewandte Chemie International Edition. 2021; 50(24): 5438–5466.
CrossRef

