
Manuscript accepted on :17-09-2025
Published online on: 30-09-2025
Plagiarism Check: Yes
Reviewed by: Dr. Surendra K Swarnkar
Second Review by: Dr. Rahul Sable
Final Approval by: Dr. Anton R Kiselev
Umesh Laddha , Gayatri Kotwal, Akshada Jadhav, Devyani Patil and Gangadhar Magar*
, Gayatri Kotwal, Akshada Jadhav, Devyani Patil and Gangadhar Magar*
Department of Pharm D, MET’s Institute of Pharmacy, Affiliated to Savitribai Phule Pune University, Bhujbal Knowledge City, Adgaon, Nasik, Maharashtra, India
Corresponding Author E-mail: magargangadhar18@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/3232
Abstract
Oral contraceptives (OCs), commonly utilized for contraception, exert considerable influence on cardiovascular health, especially in the regulation of blood pressure. This research examines the correlation between oral contraceptives, particularly those comprising estrogen and progestin, and their effect on blood pressure. Studies indicate that combination hormonal contraceptives, especially those with high-dose estrogen, raise both systolic and diastolic blood pressure, with risks amplifying according to extended usage, elevated BMI, age, and pre-existing hypertension. Conversely, progestin-only pills (POPs) have negligible effects on blood pressure, rendering them a safer option for women with cardiovascular risk. The fundamental mechanisms encompass estrogen-induced stimulation of the renin-angiotensin-aldosterone system (RAAS) and salt retention, whereas progestin influences mineralocorticoid receptors, resulting in fluid retention and vascular alterations. Meta-analyses demonstrate modest yet significant elevations in blood pressure among oral contraceptive users. Clinicians must meticulously evaluate patient profiles, monitor blood pressure, and contemplate personalized contraceptive options to mitigate cardiovascular risks. Additional randomized controlled trials (RCTs) and longitudinal studies are necessary to improve our comprehension of the effects of oral contraceptives on blood pressure in various populations, highlighting the significance of individualized contraceptive counseling.
Keywords
Blood pressure regulation; Cardiovascular risk; Estrogen; Hypertension; Individualized contraceptive counseling; Oral contraceptives; Progestin
Download this article as:| Copy the following to cite this article: Laddha U, Kotwal G, Jadhav A, Patil D, Magar G. Oral Contraceptives and Hypertension Risk: Implications for Cardiovascular Health and Clinical Management. Biomed Pharmacol J 2025;18(3). |
| Copy the following to cite this URL: Laddha U, Kotwal G, Jadhav A, Patil D, Magar G. Oral Contraceptives and Hypertension Risk: Implications for Cardiovascular Health and Clinical Management. Biomed Pharmacol J 2025;18(3). Available from: https://bit.ly/3J9Z8bG |
Introduction
One of the most popular and successful ways to avoid unwanted pregnancies is through the use of oral contraceptives (OCs), also referred to as birth control tablets. Since their launch in the 1960’s, OCs have revolutionised reproductive health by offering safe and effective birth control and empowering people to make informed reproductive decisions.1 Developments in gender roles, public health outcomes, and society dynamics have all been profoundly impacted by the creation and use of these drugs. Combination hormonal contraceptives (CHCs) and progestin-only pills (POPs) are the two primary categories of oral contraceptives.2
The contraceptive action involves blocking the pituitary gland from releasing luteinizing hormone (LH) and follicle stimulating hormone (FSH), modifying cervical mucus to limit sperm migration, and changing tubal ciliary cells to hinder ovum transport.3 Progesterone inhibits follicle growth and ovulation, which helps prevent pregnancy. It functions by inhibiting the hypothalamus’s production of hormones, which lowers levels of LH and FSH and delays follicle maturation.4 Furthermore, oestrogen slows the anterior pituitary’s negative feedback loop, which in turn prevents follicular growth and decreases FSH release. Progesterone also modifies cervical mucus and the endometrium to decrease the likelihood of implantation, which keeps sperm from entering the cervix and upper reproductive canal.5 Progestin and oestrogen in combination hormonal contraceptive affect cervical mucus, suppress ovulation, and alter the endometrial lining, reducing the risk of pregnancy. As the name implies, progestin alone is the only ingredient in these pills. For people who are contraindicated for oestrogen use or who cannot take it, these pills are especially helpful.
The effectiveness of oral contraceptives has been well-established; a failure rate of roughly 7% is yielded by average use, and less than 1% is produced with perfect use. This high degree of efficacy is attained by blocking ovulation and making the environment unfavourable for sperm and implantation.6 For many, OCs are the favoured option due to their great efficacy and ease of daily administration. OCs are widely used because they provide a number of non-contraceptive advantages in addition to contraception. These advantages include regulating the menstrual cycle, reducing cramps, treating endometriosis and polycystic ovarian syndrome, and improving acne. To further increase its appeal, using OCs has been linked to a lower risk of endometrial and ovarian malignancies.7 The use of oral contraceptives is not without its drawbacks, despite their benefits. Nausea, weight gain, mood swings, and an elevated risk of thromboembolic events are possible adverse effects, especially in smokers and people with specific medical problems.
OCs must be carefully considered based on health profiles and lifestyle factors and monitored by healthcare professional to ensure safety and efficacy.8 The introduction of newer formulations and advancements in oral contraceptive technology continue to improve user experience and safety. Contemporary research focuses on reducing side effects, enhancing effectiveness, and expanding the range of therapeutic benefits. The changing landscape of reproductive health and rights emphasises the need for comprehensive education and OCs access to help people make educated decisions that meet their personal and health needs.
Evaluating the overall safety and effectiveness of OCs requires an understanding of the cardiovascular consequences, especially those pertaining to blood pressure.9 Extensive research is necessary to fully understand the potential effects of OCs, especially those that include progestin and oestrogen, on cardiovascular health. There is evidence that these hormonal agents interact with a number of physiological mechanisms involved in blood pressure regulation. Oestrogen in combination hormonal contraceptives causes fluid retention and changes the renin-angiotensin-aldosterone pathway, which raises blood pressure. Furthermore, oestrogen may affect vascular tone and endothelial function, which may alter systemic vascular resistance and arterial stiffness. Although its effects are often less evident than those of oestrogen, progestin, the other primary hormone in combined OCs, can also affect blood pressure. Fluid balance and vascular tone can be affected by progestin’s interaction with mineralocorticoid receptors, which in turn affects blood pressure.10
The risk factors associated with the use of OCs vary depending on whether they influence the venous or arterial components of the cardiovascular system. Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is the main category of venous events. Ischemic or haemorrhagic stroke and myocardial infarction (MI), on the other hand, are examples of arterial events.11 According to study, there may be a difference in the relative influence of common cardiovascular disease risk factors such as obesity, diabetes, hypertension, and smoking on the two kinds of occurrences. According to major WHO studies, smoking, hypertension, and diabetes increase arterial events including MI and stroke but not venous events. However, a risk factor for venous as well as arterial incidents is obesity.12
The objective of the meta-analysis is to compile information from multiple trials in order to measure the total impact of OCs on blood pressure. Combining the findings of several research projects, the meta-analysis examines how OCs, particularly combination hormonal contraceptive (CHCs) and progestin-only pills (POPs), affects blood pressure.13 To ascertain the average effect size, spot potential variances among various populations, and assess the consistency of findings, statistical analysis of the data is required. This kind of analysis offers a more comprehensive view of the effects in various study settings and aids in determining the level of risk connected with OC usage.
This study focusses on how OCs affect blood pressure, is essential in combining information from different studies to offer a thorough evaluation of these effects. The findings can spot patterns and disparities in blood pressure changes linked to OC usage by methodically examining and evaluating data from several research projects. This analysis sheds light on whether OCs cause clinically significant increases in blood pressure and, if so, what circumstances or demographics are most affected. All of these goals work together to give a thorough assessment of how OCs impact blood pressure, educating medical professionals and directing clinical judgements to improve patient safety and maximise contraceptive treatment.
Materials and Methods
A thorough and methodical search strategy was utilized to assess the correlation between blood pressure, cardiovascular risk, and the usage of oral contraceptives. To guarantee the incorporation of all pertinent studies, many databases were examined, each providing a distinct and valuable assemblage of biological literature. PubMed was employed for its comprehensive collection of clinical research papers, systematic reviews, and meta-analyses concerning oral contraceptives and cardiovascular health. Embase, recognized for its emphasis on pharmacological research and extensive indexing of European and global journals, was incorporated to guarantee a wide range of pertinent publications. The Cochrane Library was also searched for high-quality systematic reviews and clinical trials that offer robust data about the effects of oral contraceptives on blood pressure and cardiovascular risk.
Rigorous inclusion and exclusion criteria were implemented to uphold the relevance and quality of the studies included. The inclusion criteria comprised randomized controlled trials (RCTs), cohort studies, case-control studies, and systematic reviews or meta-analyses, as these methodologies yield substantial evidence. The target demographic comprised women utilizing oral contraceptives, irrespective of age or health condition, with an emphasis on research that documented blood pressure readings and cardiovascular risk. Outcome measures needed to encompass the impact of oral contraceptives on blood pressure and related cardiovascular diseases, including hypertension and other cardiovascular events. To guarantee that the study incorporated the most recent evidence and therapeutic practices, only articles published in the past 20 years were considered. Moreover, the research was restricted to those published in English to ensure clarity and accessibility of information.
Studies were omitted if they did not pertain to primary research or systematic reviews. This encompassed editorials, opinion articles, and conference abstracts, as these sources lack unique scientific data. Research concentrating solely on non-human subjects or failing to directly evaluate the effects of oral contraceptives on blood pressure and cardiovascular risk was likewise eliminated. Furthermore, studies that did not provide explicit data on blood pressure or cardiovascular outcomes, or in which oral contraceptive use was not a principal variable of inquiry, were excluded. The study sought to provide a thorough and evidence-based assessment of the impact of oral contraceptives on blood pressure and cardiovascular health using a stringent selection procedure.
Overview of Included Studies
A significant study that tracked women taking OCs for ten years to evaluate blood pressure variations and cardiovascular events was carried out in the United States (n = 13,000).14 Long-term OCs users of a different cohort research conducted in Europe (n = 17,032) showed a rather larger increase in blood pressure than non-users.15 A cross-sectional study conducted in South Asia (n = 1,500) also revealed geographical differences; women who used OCs for more than two years had notably higher systolic and diastolic blood pressure than their non-using peers.16
Different formulations resulting from the hormone mix and OCP route of delivery affect hormone balance, menstruation, and individual appropriateness differently. Continuous cycle pills, extended cycle pills, progestin-only pills (POPs), and combined oral contraceptive pills (COCs) are four main groups into which all OCs fall. Every category offers special advantages and particular applications (Fig.1).
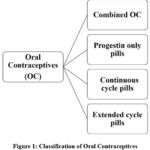 |
Figure 1: Classification of Oral ContraceptivesClick here to view Figure |
Combined Oral Contraceptive Pills (COCs)
Most often given OCs are COCs, which mix oestrogen with progestin. Monophasic and multiphasic COCs are the two primary forms they fall into. Following a 7-day pill-free interval, monophasic COCs offer a continuous hormone dosage throughout the 21-day cycle, therefore inducing a withdrawal bleed.17 This easy schedule guarantees constant hormone exposure. In contrast, multiphasic COCs mimic normal fluctuations to reduce mood swings and bloating. Notwithstanding these changes, a study written in the Journal of Hypertension claims that the cardiovascular hazards are nevertheless comparable to those of monophasic pills. Particularly in women over 35 or those inclined to hypertension, both monophasic and multiphasic COCs have been demonstrated to increase blood pressure. Advise regular blood pressure monitoring even if recent low-dose COCs (with oestrogen levels less than 50 mcg) have greatly lower this risk.18
Progestin-Only Pills (POPs)
POPs, also known as mini-pills, are oestroge-free and provide a steady daily dose of progestin. They are suitable for women with coagulation issues, migraines, hypertension, or nursing mothers. POPs weaken the uterine lining and thickening cervical mucus thereby inhibiting fertilisation. POPs unlike COCs lack a pill-free period, so they usually cause regular menstruation not unlike COCs. Studies have revealed that POPs are linked with a reduced cardiovascular risk than COCs. Since POPs lack oestrogen, which is known to affect blood pressure and raise thromboembolic risk.19
Continuous-Cycle and Extended-Cycle Pills
Continuous-cycle and Extended-cycle pills are options for women who want to minimize the frequency of menstrual cycles. Extended-cycle tablets are taken for 12 straight weeks, then a 7-day break yields just four periods annually.20 Women who have severe premenstrual syndrome (PMS), significant monthly bleeding, or period-related migraines will find this schedule helpful. Extended-cycle tablets clearly lower menstruation symptoms and have the same contraceptive efficacy as conventional 21-day regimens, according a review in the Contraception Journal.
Continuous-cycle tablets erase menstruation when used daily for a year. Women who prefer convenience or have medical issues like endometriosis where menstruation worsens symptoms are using this alternative more. Though long-term data is still being gathered, studies show that consistent use is safe and does not negatively affect cardiovascular health.21
Health Considerations and Choice of Pills
OCs choice usually relies on personal lifestyle preferences, health issues, and goals for menstruation control. Although COCs are usually effective, especially in older women or those who smoke, they may raise blood clot and hypertension risk. POPs provide a safer substitute for those having cardiovascular risk factors. Concurrent with this, continuous- and extended-cycle tablets offer more choices for controlling menstruation and improving general convenience as shown in Table 1.22
Table 1: Comparison of Oral Contraceptive Pill Types
| Type of Pill | Hormones | Cycle Length | MenstruationImpact | Target Population |
| Monophasic COCs | Estrogen + Progestin | 21 days on, 7 days off | Regular withdrawal bleed | General users |
| Multiphasic COCs | Varying Estrogen + Progestin | 21 days on, 7 days off | Regular withdrawal bleed | Users seeking fewer side effects |
| Progestin-Only Pills (POPs) | Progestin only | Daily, no breaks | Irregular or no menstruation | Breastfeeding, cardiovascular risk |
| Extended-Cycle Pills | Estrogen + Progestin | 12 weeks on, 7 days off | Fewer periods (4/year) | Heavy menstruation, migraines |
| Continuous-Cycle Pills | Estrogen + Progestin | Daily, no breaks | No menstruation | Endometriosis, convenience |
Oral contraceptive effects on blood pressure
The use of OCs has been linked to an increased risk of hypertension, particularly with long-term use. Numerous studies suggest that the hormonal components of OCs, specifically estrogen and progestin, can modulate blood pressure through various physiological pathways.23 One prominent study, the Tabari Cohort, reported that women who had used OCs had a 23% higher risk of hypertension compared to those who had never used them (adjusted odds ratio 1.23). Additionally, prolonged use significantly increases the risk. Women who used OCs for more than 120 months had a 47% higher chance of developing hypertension compared to non-users.24
Mechanisms of Blood Pressure Elevation
OCs affect hypertension by means of several physiological processes that finally raise blood pressure. The renin-angiotensin-aldosterone system (RAAS) is one of the main processes as it is so important for control of blood pressure and fluid balance (Fig.2)25. Activating RAAS causes sodium and water retention, which helps to explain higher blood volume and hence higher blood pressure. Key hormonal components of OCs, oestrogen and progesterone, also have major effects on blood pressure control. Oestrogen has been linked to the RAAS pathway activation and fluid retention, therefore aggravating hypertension. Furthermore, interacting with the mineralocorticoid receptor, progesterone could cause salt retention and raised blood pressure. These hormonal influences help to explain a general change in cardiovascular performance.26 OCs also affect arterial stiffness, which is another way they impact hypertension. Reduced flexibility of blood arteries resulting from increased arterial stiffness makes it more difficult for the circulatory system to adjust for changes in blood pressure. This change in vascular tone causes reduced vasodilation, which also helps to explain variances in blood pressure. Inappropriate dilating of blood arteries can lead to persistent hypertension, hence raising the risk of cardiovascular problems.27
OCPs affect hypertension generally in a complex manner with hormonal effects on fluid retention, vascular stiffness, and changed blood pressure control.28 Particularly in those prone to hypertension, evaluating the cardiovascular risks linked with OCP usage depends on an awareness of these processes. By means of appropriate blood pressure monitoring and evaluation, women taking OCPs can help to reduce possible hypertension effects and guarantee safer contraceptive choices for at-risk groups.
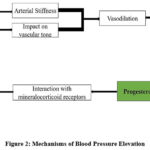 |
Figure 2: Mechanisms of Blood Pressure ElevationClick here to view Figure |
Results
Blood Pressure Elevation Due to Oral Contraceptives
The utilisation of OCs results in a statistically significant elevation in blood pressure relative to non-users. The increase in systolic blood pressure (2-4 mmHg) and diastolic blood pressure (1-3 mmHg) is mostly ascribed to estrogen-induced stimulation of the RAAS, which facilitates sodium retention and fluid overload (Table 2). This indicates that even slight elevations in blood pressure among oral contraceptive users may elevate the long-term risk of hypertension, especially in vulnerable individuals (Fig.3).29,30
Table 2: Blood Pressure Elevation Due to Oral Contraceptives29,30
| Parameter | Effect in OC Users | Effect in Non-Users | Statistical Significance |
| Systolic BP (SBP) | ↑ 2-4 mmHg | No significant change | p < 0.05 |
| Diastolic BP (DBP) | ↑ 1-3 mmHg | No significant change | p < 0.05 |
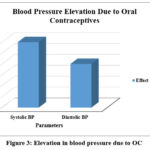 |
Figure 3: Elevation in blood pressure due to OCClick here to view Figure |
Hypertension Risk Based on Duration of OC Use
Prolonged usage of OCs is associated with an escalating risk of hypertension. Studies indicate a 15% increase in risk for users under 5 years and up to 47% increased risk in users exceeding 10 years (Table 3). This substantiates the notion that extended exposure to synthetic oestrogen and progestin may provoke vascular alterations and elevate blood pressure, highlighting the necessity for routine blood pressure monitoring in long-term users (Fig.4).31,32
Table 3: Hypertension Risk Based on Duration of OC Use31,32
| Duration of OC Use | Relative Risk (RR) of Hypertension | Odds Ratio (OR) | 95% Confidence Interval (CI) |
| < 5 years | 1.15 | 1.12 | (1.05 – 1.21) |
| 5 – 10 years | 1.30 | 1.25 | (1.15 – 1.38) |
| > 10 years | 1.47 | 1.40 | (1.27 – 1.55) |
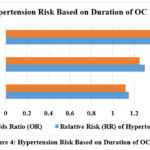 |
Figure 4: Hypertension Risk Based on Duration of OC UseClick here to view Figure |
OC Formulation and Blood Pressure Variability
Higher-dose estrogen-containing OCs are significantly correlated with increased blood pressure, but progestin-only pills exhibit negligible effects on blood pressure. This indicates that for women susceptible to hypertension, low-dose OCs or progestin-only formulations may represent a safer option (Table 4).22,33
Table 4: OC Formulation and Blood Pressure Variability22,33
| OC Type | Systolic BP Increase | Diastolic BP Increase | Recommendation |
| High-Dose Combined Pills (≥50 μg estrogen) | +4 mmHg | +2 mmHg | Avoid in hypertensive women |
| Low-Dose Combined Pills (<50 μg estrogen) | +2 mmHg | +1 mmHg | Consider safer, but monitor BP |
| Progestin-Only Pills (POPs) | Minimal change | Minimal change | Preferred for hypertensive women |
| Extended/Continuous-Cycle Pills | Gradual BP increase over time | Gradual BP increase over time | Monitor BP in long-term users |
Age, BMI, and Lifestyle Factors in OC-Induced Hypertension
Older women and individuals with elevated BMI have a more pronounced increase in blood pressure due to diminished arterial flexibility and the buildup of oestrogen in adipose tissue (Table 5). Smoking intensifies hypertension and cardiovascular risk, rendering OCs use especially alarming in these populations.22,34,35
Table 5: Age, BMI, and Lifestyle Factors in OC-Induced Hypertension22,34,35
| Risk Factor | Effect on BP | Increased Risk |
| Age > 45 years | Increased BP due to reduced vascular elasticity | 3.5 mmHg higher SBP vs. younger users |
| BMI > 30 | Higher estrogen levels, RAAS activation | 35% increased risk of hypertension |
| Smoking | Vasoconstriction, increased clot risk | 4-5x increased thromboembolic risk |
Meta-Analysis of BP Trends in OC Users
Older women show higher blood pressure rises than younger women, which supports age-specific contraceptive prescriptions. Meta-analysis studies repeatedly linked long-term OC usage to rises in both systolic and diastolic blood pressure (Table 6 & Fig.5).36-37
Table 6: Meta-Analysis of BP Trends in OC Users36-37
| Study Population | Systolic BP Change (mmHg) | Diastolic BP Change (mmHg) |
| Women aged 35-45 years | +3.5 mmHg | +2.0 mmHg |
| Women aged <35 years | +1.5 mmHg | +1.0 mmHg |
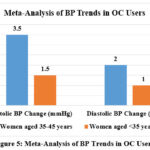 |
Figure 5: Meta-Analysis of BP Trends in OC UsersClick here to view Figure |
Clinical Recommendations Based on Results
Hypertensive women should steer clear of combination estrogen-progestin OCs and think about non-hormonal or progestin-only contraception. Early hypertension can be detected by regular blood pressure monitoring; if BP rises above 10 mmHg, cessation should be taken under consideration.38-42
Table 7: Clinical Recommendations Based on Results38-42
| Recommendation | Target Group |
| Use progestin-only or non-hormonal OCs | Women with hypertension |
| Monitor BP every 6 months after starting OCs | All OC users, especially older women |
| Discontinue OCs if BP rises >10 mmHg above baseline | High-riskindividuals |
Discussion
Healthcare providers must weigh the risks and advantages of OCs, especially for women with high blood pressure or a higher risk of cardiovascular disease. The link between OCs and blood pressure is well established, showing that particular formulations might cause raised blood pressure in sensitive persons with the possible mechanism as described in figure 6.43 To reduce possible risk, physicians should undertake complete health evaluations for each patient, taking into account age, body mass index (BMI), smoking status, and pre-existing medical disorders44. This allows them to identify women who may be at a higher risk for unfavourable cardiovascular events associated with OC usage. For patients with hypertension or other cardiovascular risk factors, progestin-only pills or non-hormonal solutions may be safer and more appropriate.45
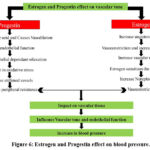 |
Figure 6: Estrogen and Progestin effect on blood pressure.Click here to view Figure |
In addition to careful prescription, frequent blood pressure monitoring is necessary for women using OCs, particularly those who are at increased risk of hypertension. A study reported by Cameron et al. 2023 showed elevated blood pressure after continuous use of OCs. Out of 68297 participants (aged 25-42 years) form United states, reported increased SBP and DBP by 0.7 mmHg (95% CI, 0.4–1 mmHg) and 0.4 mmHg (95% CI, 0.4–0.6mmHg) respectively where age, existing CVD, smoking and family history were the additional contributing factors. Furthermore; 4 years’ follow-up showed the more risk of hypertension (1.2 times more) in post OCs user. Moreover; similar risk was reported by the survey performed in England, Germany, and Korea. The SBP and DBP for the users of OCs was found to be higher by 2.6 to 5.8 mmHg and 1.8 to 3.6 mmHg than non-users. Available evidences clearly reflect the risk of increased hypertension among the OCs users in comparison to non-users.22 Henceforth; healthcare professions may recommend regular blood pressure checks, especially in the first several months of OCs use, when side effects may be more obvious and after two years of treatment.46 The American College of Obstetricians and Gynaecologists (ACOG) recommends that healthcare providers measure blood pressure at least once a year for women taking combined hormonal contraceptives;22 however, more frequent monitoring may be required for patients with elevated baseline blood pressure or other cardiovascular risk factors.47 Patient should also be educated to detect hypertension symptoms and encouraged to report any severe health changes immediately. This proactive blood pressure monitoring technique identifies potential issues early, allowing for risk reduction.
The necessity of tailored contraceptive alternatives and medicine is critical in improving the health outcomes of women who use OCs. Because each woman’s health profile is unique, the efficacy and safety of OCs might differ depending on individual characteristics like as age, weight, and overall health.8,9 Personalised contraceptive counselling allows healthcare practitioners to personalise suggestions to their patients’ unique needs and preferences.48 Women with higher cardiovascular risk, for example, may benefit from low-dose oestrogen or progestin formulations, but others may prefer non-hormonal techniques entirely.49 Furthermore, incorporating shared decision-making into the contraceptive counselling process enables patients to communicate their concerns and desires about contraceptive techniques.50 This strategy improves patient satisfaction and adherence, allowing women to make more educated decisions regarding their reproductive health.
Limitations and Future Directions
The current data exploring how oral contraceptives (OCs) influence blood pressure (BP) faces significant challenges, primarily due to its reliance on observational studies. These studies often analyse data retrospectively, making it difficult to isolate the direct impact of OCs from confounding factors such as lifestyle, pre-existing health conditions, and genetic predispositions. Such limitations can lead to misinterpretations, potentially skewing clinical recommendations and patient care.
The Need for Randomized Controlled Trials (RCTs)
Randomized controlled trails (RCTs) are essential to overcome these constraints. RCTs reduce confounding variables by randomly assigning subjects to either an OCs or a placebo, providing more reliable proof of OC-BP causality. Long-term RCTs are crucial for assessing OCs long-term effects on BP and identifying prolonged use concerns.
Inclusion of Diverse Populations
Future study should involve participants of various ages, nationalities, and health situations. This method will reveal how OCs affects different populations, enabling the development of patient-specific contraceptives.
Mechanistic Studies and Therapeutic Approaches
Investigating the mechanisms through which OCs influence BP such as their effects on the RAAS could pave the way for targeted therapies. Lifestyle adjustment or RAAS inhibitors may reduce BP effects in vulnerable people.
Implications for Clinical Practice and Policy
Future study results will have far-reaching ramifications for healthcare practice. Healthcare providers can better administer OCs with individualised instruction, especially for women at risk of hypertension or cardiovascular disease. Policymakers might also use this evidence to expand contraceptive alternatives and education, empowering women to make educated reproductive health.
Direct Comparison of OC Preparations
Comparative studies evaluating the BP effects of different OC formulations are essential. These studies will help identify safer alternatives for women at risk, ensuring that contraceptive solutions align with individual health profiles.
Conclusion
Oral contraceptives, especially those comprising estrogen and progestin, significantly influence blood pressure, resulting in elevated systolic and diastolic measurements. The risk increases with extended use, high-dose estrogen formulations, and in women with predisposed factors including elevated BMI, advanced age, and pre-existing hypertension. Progestin-only pills are linked to negligible alterations in blood pressure, rendering them a favorable choice for women with elevated cardiovascular risk.
While the observed increases in blood pressure are generally modest in absolute terms, their cumulative effect over time particularly in high-risk individuals may be clinically meaningful and warrants caution. It is also important to distinguish between statistical and clinical significance: although some changes reached statistical significance, their real-world impact on individual patient profiles and duration of use.
Clinical guidelines underscore the need of personalized contraceptive choices, especially for women with hypertension and cardiovascular issues. Consistent blood pressure monitoring is essential, particularly during the initial months of OCs therapy, to identify and address possible hazards promptly. Future research should prioritize longitudinal studies in diverse population to enhance our understanding of these effects and support the development of safer contraceptive strategies. These findings are vital for guiding clinical management and informing public health policies aimed at reducing cardiovascular risk associated with OCs use.
Acknowledgment
We, thank you to the MET’s, Institute of Pharmacy, BKC, affiliated under Savitribai Phule Pune University, Nashik, for their constant support and providing all facilities to complete this work.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest
Data Availability
This statement does not apply to this article
Ethics Statement:
This review work did not involve human participants, animal subjects, or any material that requires ethical approval
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical trial registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not applicable
Author’s Contribution
- Umesh Laddha: Supervision, Writing-original draft and editing.
- Gayatri Kotwal: Data collection, Writing- original draft
- Akshada Jadhav: Data collection, Writing- original draft
- Devyani Patil: Data collection, Writing- original draft
- Gangadhar Magar: Conceptualization, Data collection, Data analysis Writing- original draft
References
- Dhont M. History of oral contraception. Eur J Contracept Reprod Health Care. 2010;15 Suppl 2:S12-S18. doi:10.3109/13625187.2010.513071
CrossRef - Morotti M, Remorgida V, Venturini PL, Ferrero S. Progestin-only contraception compared with extended combined oral contraceptive in women with migraine without aura: a retrospective pilot study. Eur J Obstet Gynecol Reprod Biol. 2014;183:178-182. doi:10.1016/j.ejogrb.2014.10.029
CrossRef - Calçada MMS, Alves AMR. Hormonal Contraceptives and Post-fertilization Effects. Issues Law Med. 2022;37(1):29-80.
- Shoham Z, Jacobs HS, Insler V. Luteinizing hormone: its role, mechanism of action, and detrimental effects when hypersecreted during the follicular phase. Fertil Steril. 1993;59(6):1153-1161. doi:10.1016/s0015-0282(16)55968-8
CrossRef - Bastianelli C, Farris M, Bruni V, Rosato E, Brosens I, Benagiano G. Effects of progestin-only contraceptives on the endometrium. Expert Rev Clin Pharmacol. 2020;13(10):1103-1123. doi:10.1080/17512433.2020.1821649
CrossRef - Trussell J, Portman D. The creeping Pearl: Why has the rate of contraceptive failure increased in clinical trials of combined hormonal contraceptive pills?. Contraception. 2013;88(5):604-610. doi:10.1016/j.contraception. 2013.04.001
CrossRef - Ignatov A, Ortmann O. Endocrine Risk Factors of Endometrial Cancer: Polycystic Ovary Syndrome, Oral Contraceptives, Infertility, Tamoxifen. Cancers. 2020;12(7):1766. doi:https://doi.org/10.3390/cancers 12071766
CrossRef - De Leo V, Musacchio MC, Cappelli V, Piomboni P, Morgante G. Hormonal contraceptives: pharmacology tailored to women’s health. Human Reproduction Update. 2016;22(5):634-646. doi:https://doi.org/10.1093/ humupd/dmw016
CrossRef - Baillargeon JP, McClish DK, Essah PA, Nestler JE. Association between the Current Use of Low-Dose Oral Contraceptives and Cardiovascular Arterial Disease: A Meta-Analysis. The Journal of Clinical Endocrinology and Metabolism. 2005;90(7):3863-3870. doi:https://doi.org/10.1210/jc.2004-1958
CrossRef - Herrington DM, McClain BP. Sex hormones and normal cardiovascular physiology in women. Published online November 10, 2005:478-508. doi:https://doi.org/10.3109/9780203640340-34
- Wenger N, Sebastian T, Engelberger RP, Kucher N, Spirk D. Pulmonary embolism and deep vein thrombosis: Similar but different. Thrombosis Research. 2021;206:88-98. doi:https://doi.org/10.1016/j.thromres. 2021.08.015
CrossRef - Previtali E, Bucciarelli P, Passamonti SM, Martinelli I. Risk factors for venous and arterial thrombosis. Blood transfusion = Trasfusione del sangue. 2011;9(2):120-138. doi:https://doi.org/10.2450/2010.0066-10
- Gawronska J, Meads C, Smith L, Cao C, Wang N, Walker S. Association of oral contraceptive pill use and depression among US women. Journal of Affective Disorders. 2024;344:132-140. doi:https://doi.org/10.1016/ j.jad.2023.10.041
CrossRef - Wilson P, Culleton B. Epidemiology of cardiovascular disease in the United States. American Journal of Kidney Diseases. 1998;32(5):S56-S65. doi:https://doi.org/10.1053/ajkd.1998.v32.pm9820465
CrossRef - Gadducci A, Barsotti C, Cosio S, Domenici L, Riccardo Genazzani A. Smoking habit, immune suppression, oral contraceptive use, and hormone replacement therapy use and cervical carcinogenesis: a review of the literature. Gynecological Endocrinology. 2011;27(8):597-604. doi:https://doi.org/10.3109/ 09513590.2011. 558953
CrossRef - Cao L, Yan C, Yu X, Zou X, Xu J, Shen X. Prenatal Exposure to PCBs and OCPs and Neurodevelopment of Newborn: Shanghai Study. Epidemiology. 2011;22:S286-S287. doi:https://doi.org/10.1097/01.ede. 0000392580. 73317.c1
CrossRef - Dragoman MV. The combined oral contraceptive pill- recent developments, risks and benefits. Best Practice & Research Clinical Obstetrics & Gynaecology. 2014;28(6):825-834. doi:https://doi.org/10.1016/ j.bpobgyn. 2014.06.003
CrossRef - Fruzzetti F, Fidecicchi T, Gambacciani M. Oestrogens in oral contraception: considerations for tailoring prescription to women’s needs. The European Journal of Contraception & Reproductive Health Care. 2024;29(3):93-102. doi:https://doi.org/10.1080/13625187.2024.2334350
CrossRef - Windisch S, Frishman WH. Thrombotic and Vascular Complications of Oral Contraceptives. Cardiology in Review. Published online January 17, 2024. doi:https://doi.org/10.1097/crd.0000000000000643
CrossRef - Shrader SP, Dickerson LM. Extended- and Continuous-Cycle Oral Contraceptives. Pharmacotherapy. 2008;28(8):1033-1040. doi:https://doi.org/10.1592/phco.28.8.1033
CrossRef - Burkman R, Bell C, Serfaty D. The evolution of combined oral contraception: improving the risk-to-benefit ratio. Contraception. 2011;84(1):19-34. doi:https://doi.org/10.1016/j.contraception.2010.11.004
CrossRef - Cameron NA, Blyler CA, Bello NA. Oral Contraceptive Pills and Hypertension: A Review of Current Evidence and Recommendations. Hypertension. 2023;80(5):924-935. doi:https://doi.org/10.1161/ hypertensionaha. 122.20018
CrossRef - Davis HC, Hackney AC. The Hypothalamic–Pituitary–Ovarian Axis and Oral Contraceptives: Regulation and Function. Sex Hormones, Exercise and Women. Published online November 11, 2016:1-17. doi:https://doi.org/10.1007/978-3-319-44558-8_1
CrossRef - Park H, Kim K. Associations between oral contraceptive use and risks of hypertension and prehypertension in a cross-sectional study of Korean women. BMC Women’s Health. 2013;13(1). doi:https://doi.org/10.1186/ 1472-6874-13-39
CrossRef - Seravalle G, Guıdo Grassı. Renin–angiotensin–aldosterone system and blood pressure regulation. Elsevier eBooks. Published online January 1, 2023:63-75. doi:https://doi.org/10.1016/b978-0-323-96120-2.00002-9
CrossRef - Fuller PJ, Young MJ. Mechanisms of Mineralocorticoid Action. Hypertension. 2005;46(6):1227-1235. doi:https://doi.org/10.1161/01.hyp.0000193502.77417.17
CrossRef - Tan CH, Low KA, Kong T, et al. Mapping cerebral pulse pressure and arterial compliance over the adult lifespan with optical imaging. Rypma B, ed. PLOS ONE. 2017;12(2):e0171305. doi:https://doi.org/10.1371 /journal.pone. 0171305
CrossRef - Drury ER, Wu J, Gigliotti JC, Le TH. Sex Differences in Blood Pressure Regulation and Hypertension: Renal, Hemodynamic, and Hormonal Mechanisms. Physiological Reviews. 2024;104(1):199-251. doi:https://doi.org/10.1152/physrev.00041.2022
CrossRef - Kung AW, Fan T, Xu L, et al. Factors influencing diagnosis and treatment of osteoporosis after a fragility fracture among postmenopausal women in Asian countries: a retrospective study. BMC Women’s Health. 2013;13(1). doi:https://doi.org/10.1186/1472-6874-13-7
CrossRef - dos Santos PA, de Oliveira AM, Alves CQ, Souza Filho CF, Ladeia AMT, Petto J. Renin-Angiotensin-Aldosterone System in Women Using Combined Oral Contraceptive: A Systematic Review. Revista Brasileira de Ginecologia e Obstetrícia / RBGO Gynecology and Obstetrics. 2022;44(07):710-718. doi:https://doi.org/10.1055/s-0042-1745790
CrossRef - Stanczyk FZ, Archer DF, Bhavnani BR. Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment. Contraception. 2013;87(6):706-727. doi:10.1016/j.contraception.2012.12.011
CrossRef - Mathieu P, Poirier P, Pibarot P, Lemieux I, DesprésJP. Visceral Obesity. Hypertension. 2009;53(4):577-584. doi:https://doi.org/10.1161/hypertensionaha.108.110320
CrossRef - Casanova G, Bossardi Ramos R, Ziegelmann P, Spritzer PM. Effects of Low-Dose Versus Placebo or Conventional-Dose Postmenopausal Hormone Therapy on Variables Related to Cardiovascular Risk: A Systematic Review and Meta-Analyses of Randomized Clinical Trials. The Journal of Clinical Endocrinology & Metabolism. 2015;100(3):1028-1037. doi:https://doi.org/10.1210/jc.2014-3301
CrossRef - HEE L, KETTNER LO, VEJTORP M. Continuous use of oral contraceptives: an overview of effects and side-effects. Acta Obstetricia et Gynecologica Scandinavica. 2012;92(2):125-136. doi:https://doi.org/ 10.1111/ aogs.12036
CrossRef - Hussain SF. Progestogen-only pills and high blood pressure: is there an association? Contraception. 2004;69(2):89-97. doi:https://doi.org/10.1016/j.contraception.2003.09.002
CrossRef - Kharbanda EO, Parker ED, Sinaiko A, et al. Initiation of Oral Contraceptives and Changes in Blood Pressure and BMI in Healthy Adolescents. The Journal of pediatrics. 2014;165(5):1029-1033. doi:https://doi.org/10.1016/j.jpeds.2014.07.048
CrossRef - Ruan X, Mueck AO. Oral contraception for women of middle age. Maturitas. 2015;82(3):266-270. doi:https://doi.org/10.1016/j.maturitas.2015.06.030
CrossRef - Curtis KM, Tepper NK, Marchbanks PA. U.S. medical eligibility criteria for contraceptive use, 2010. J Womens Health (Larchmt). 2011;20(6):825-828. doi:10.1089/jwh.2011.2851
CrossRef - Brown HL, Warner JJ, Gianos E, et al. Promoting Risk Identification and Reduction of Cardiovascular Disease in Women Through Collaboration With Obstetricians and Gynecologists: A Presidential Advisory From the American Heart Association and the American College of Obstetricians and Gynecologists. Circulation. 2018;137(24). doi:https://doi.org/10.1161/cir.0000000000000582
CrossRef - American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 203. Obstetrics & Gynecology. 2019;133(1):e26-e50. doi:https://doi.org/10.1097/aog.0000000000003020
CrossRef - de Melo NR. Estrogen-Free Oral Hormonal Contraception: Benefits of the Progestin-Only Pill. Women’s Health. 2010;6(5):721-735. doi:https://doi.org/10.2217/whe.10.36
CrossRef - Florio K, Kao M, Johnson T, et al. Contraception for the Cardiac Patient: a Cardiologist’s Primer. Current Treatment Options in Cardiovascular Medicine. 2020;22(12). doi:https://doi.org/10.1007/s11936-020-00853-7
CrossRef - Harvey RE, Hart EC, Charkoudian N, et al. Oral Contraceptive Use, Muscle Sympathetic Nerve Activity, and Systemic Hemodynamics in Young Women. Hypertension. 2015;66(3):590-597. doi:https://doi.org/10.1161/hypertensionaha.115.05179
CrossRef - Flaherty GT, Hession P, Liew CH, et al. COVID-19 in adult patients with pre-existing chronic cardiac, respiratory and metabolic disease: a critical literature review with clinical recommendations. Tropical Diseases, Travel Medicine and Vaccines. 2020;6(1). doi:https://doi.org/10.1186/s40794-020-00118-y
CrossRef - Sammaritano LR. Which Hormones and Contraception for Women with APS? Exogenous Hormone Use in Women with APS. Current Rheumatology Reports. 2021;23(6). doi:https://doi.org/10.1007/s11926-021-01006-w
CrossRef - Stergiou GS, Palatini P, Parati G, et al. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. Journal of Hypertension. 2021;39(7):1293-1302. doi:https://doi.org/10.1097/hjh.0000000000002843
CrossRef - Vasan RS, Larson MG, Leip EP, et al. Impact of High-Normal Blood Pressure on the Risk of Cardiovascular Disease. New England Journal of Medicine. 2001;345(18):1291-1297. doi:https://doi.org/10.1056/nejmoa003417
CrossRef - Bitzer J, Marin V, Lira J. Contraceptive counselling and care: a personalized interactive approach. The European Journal of Contraception & Reproductive Health Care. 2017;22(6):418-423. doi:https://doi.org/10.1080/13625187.2017.1414793
CrossRef - Freeman S, Shulman LP. Considerations for the use of progestin-only contraceptives. Journal of the American Academy of Nurse Practitioners. 2010;22(2):81-91. doi:https://doi.org/10.1111/j.1745-7599.2009.00473.x
CrossRef - Freeman S, Shulman LP. Considerations for the use of progestin-only contraceptives. Journal of the American Academy of Nurse Practitioners. 2010;22(2):81-91. doi:https://doi.org/10.1111/j.1745-7599.2009.00473.x
CrossRef
Abbreviations List
OCs: Oral contraceptives;
RAAS: renin-angiotensin-aldosterone system;
RCTs: randomized controlled trials;
POPs: progestin-only pills;
CHCs: Combination hormonal contraceptives;
LH: luteinizing hormone;
FSH: follicle-stimulating hormone

