
Manuscript accepted on :06-05-2025
Published online on: 05-06-2025
Plagiarism Check: Yes
Reviewed by: Dr. Nicolas Padilla
Second Review by: Dr. Gowri Sankara Rao Burle
Final Approval by: Dr. Anton R Keslav
Ángel Tarra-Marrugo1 , Daniel Meléndez-Díaz1, Yicela Pérez-Loaiza1, Maryarena Castro-Leones1, Leonardo Soto-Anaya1, Dilia Aparicio-Marenco2 and Neyder Contreras-Puentes2
, Daniel Meléndez-Díaz1, Yicela Pérez-Loaiza1, Maryarena Castro-Leones1, Leonardo Soto-Anaya1, Dilia Aparicio-Marenco2 and Neyder Contreras-Puentes2
1Department of Medicine, Rafael Núñez University Corporation, Cartagena de Indias D.T. and C., Colombia.
2GINUMED, Department of Medicine, Rafael Núñez University Corporation, Cartagena de Indias D.T. and C., Colombia.
Corresponding Author E-mail: neyder.contreras@curnvirtual.edu.co
DOI : https://dx.doi.org/10.13005/bpj/3161
Abstract
Obesity is a chronic disease causing physical and mental health, leading to the rise of bariatric surgery as a treatment method. However, this increases the risk of nutritional deficiencies, including vitamin B1. Evaluate the pre- and post-surgical prevalence of vitamin B1 deficiency in bariatric surgery patients. A literature search was performed using EBSCO, PubMed, PubMed Central, ScienceDirect, Scopus, and Web of Sciences databases from 2014 to 2024. Three investigators independently selected publications and data were extracted into a matrix. A risk of bias assessment was performed using the CASP and Joanna Briggs Institute Checklist. Statistical analyses were conducted using R software. The review included 16 studies, of which 3,384 patients undergoing bariatric surgery were included and 2702 individuals with vitamin B1 deficiency. The prevalence of preoperative deficiency is 18%, and postoperative deficiency is 17% in 3 months, decreasing to 8% in 12 months. The Roux-en-Y gastric bypass and sleeve gastrectomy showed postoperative prevalences of 12 and 4%, respectively. The most frequent comorbidities reported were DM-II, hypertension and dyslipidemias. Vitamin B1 deficiency associated with bariatric surgeries showed considerable pre-operative prevalence values, which decreased in the postoperative period due to strategies such as supplementation, favoring reduced adverse events and complications.
Keywords
Bariatric surgery; Deficiency; Obesity; Prevalence; Vitamin B1
Download this article as:| Copy the following to cite this article: Marrugo A. T, Díaz D. M, Loaiza Y. P, Leones M. P, Anaya L. S, Marenco D. A. Puentes N. C. Prevalence of Vitamin B1 Deficiency Associated with Bariatric Surgery in Obese Patients: Systematic Review and Mmeta-analysis. Biomed Pharmacol J 2025;18(2). |
| Copy the following to cite this URL: Marrugo A. T, Díaz D. M, Loaiza Y. P, Leones M. P, Anaya L. S, Marenco D. A. Puentes N. C. Prevalence of Vitamin B1 Deficiency Associated with Bariatric Surgery in Obese Patients: Systematic Review and Mmeta-analysis. Biomed Pharmacol J 2025;18(2). Available from: https://bit.ly/45GdTM8 |
Introduction
Obesity is a chronic condition defined by an excessive accumulation of body fat that adversely impacts both physical and mental health.1 According to the WHO, in 2022, one in eight people in the world was obese, representing a high economic demand for developed and developing countries, which is why different treatment methods emerged. Bariatric surgery has been the predominant method for weight reduction.2 Worldwide, more than 720,000 bariatric procedures were performed in 2018.3 Likewise, over 6,700 cases were reported in Asian countries such as Korea between 2019 and 2021.4 Sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) are the most often executed bariatric surgical methods globally. While generally beneficial, bariatric surgery may elevate the risk of nutritional deficits.5
One of these trace elements is vitamin B1, also known as thiamine. It is one of the B complex vitamins, classified as water-soluble. At the circulatory level, the enzyme thiamine diphosphokinase catalyzes the conversion of vitamin B1 into its active form, thiamine pyrophosphate (TPP), which facilitates many roles in metabolism, glycolysis, the Krebs cycle, and the pentose phosphate pathway, and is absorbed in the small intestine.6 Thiamine, or vitamin B1, deficiency arises when the recommended daily intake (RDI) is not met. Deficiency may also arise from inadequate intestinal absorption or elevated excretion rates.7 Due to the limited storage lifetime of vitamin B1 before its rapid elimination, maintaining optimal blood serum levels requires a steady and regular food intake. Specific individuals exhibit heightened vulnerability to vitamin B1 deficiency under various circumstances, particularly those after bariatric surgery.8,9
Vitamin B1 deficiency may manifest with either early or advanced symptoms. Initial symptoms predominantly originate from the neurological, cardiovascular, and gastrointestinal systems, encompassing weight loss, anorexia, disorientation, transient amnesia, malaise, muscular weakness, and cardiac manifestations.10,11 One of the most significant is beriberi, which can manifest as either wet or dry beriberi. Wet beriberi manifests as high-output heart failure characterized by edema, cardiomegaly, warm extremities, tachycardia, and respiratory distress. Dry beriberi primarily manifests as a neurological problem impacting the peripheral nervous system, characterized by peripheral neuropathy, malaise, muscular weakness, convulsions, or overactive tendon reflexes.12,13 In cases of persistent or untreated vitamin B1 deficiency, individuals may exhibit progressive symptoms, ultimately leading to the onset of Wernicke-Korsakoff syndrome.14 This condition manifests in two stages: Wernicke encephalopathy and Korsakoff psychosis. Wernicke encephalopathy is characterized by early onset and presents with polyneuropathy, ataxia, ophthalmoplegia, and gait abnormalities. If untreated, it may advance to Korsakoff psychosis, characterized by significant short-term amnesia, disorientation, confabulation, and hallucinations.15,16
This review aims to provide an update on the use of bariatric procedures in obese individuals and their link to developing vitamin B1 deficiency pre- and postoperatively.
Materials and Methods
Search strategies
The search for original scientific publications was carried out using the following databases: EBSCO, PubMed (MedLine), PubMed Central (PMC), ScienceDirect, Scopus, and Web of Sciences. To this end, restrictions were imposed regarding publication dates. EBSCO: Bariatric surgery AND vitamin B1 deficiency NOT Wernicke’s encephalopathy, publication date: 20140101-20241231. PubMed: Bariatric surgery AND vitamin B1 deficiency, publication date: 2014/01/01-2024/12/31. PubMed Central (PMC): Bariatric surgery AND vitamin B1 deficiency, publication date from 2014/01/01 to 2024/12/31. ScienceDirect: Bariatric surgery AND vitamin B1 deficiency, article type: Research articles and years: 2014-2024. Scopus: TITLE-ABS-KEY (Bariatric surgery AND vitamin B1 deficiency) AND (PUBYEAR, 2024) OR (LIMIT TO (PUBYEAR, 2023) OR (LIMIT TO (PUBYEAR, 2022) OR (LIMIT TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020) OR LIMIT-TO (PUBYEAR, 2019) OR LIMIT-TO (PUBYEAR, 2018) OR LIMIT-TO (PUBYEAR, 2017) OR LIMIT-TO (PUBYEAR, 2016) OR (LIMIT TO (PUBYEAR, 2015) OR (LIMIT TO (PUBYEAR, 2014) AND (LIMIT-TO (DOCTYPE, "ar")) AND (LIMIT-TO (LANGUAGE, "English")) AND (LIMIT-TO (PUBSTAGE, “final”)). Web of Sciences: Bariatric surgery AND vitamin B1 deficiency (All fields), refined by: publication date: 2014-01-01 to 2024-12-31, document type: Article, Languages: English.
Eligibility criteria
The original articles included adult patients over 18 years old undergoing bariatric procedures and having vitamin B1 deficiency as a study population. Clinical articles from 2014 to 2024, published in English, complete and available publications, were included. Pediatric or minor population studies excluded syndromes or pathologies linked to vitamin B1 deficiencies, experimental reports using animal models, unavailable publications, clinical case reports, case series, and brief communications.
Selection of studies and data extraction
The studies were selected using the Rayyan platform, which implements the detection and elimination of duplicates. Subsequently, three authors reviewed the titles and abstracts in parallel to discard non-relevant reports. Subsequently, key aspects were identified, including type of study, study population, sex, type of bariatric procedure, vitamin B1 concentration, relevant results, and potential complications associated with vitamin B1 deficiency.
Evaluation of the included studies
The risk of bias was evaluated with the CASP Checklist for Cohort and Randomized Controlled Studies. The Joanna Briggs Institute (JBI) Checklist for Analytical Cross-Sectional Studies questionnaire was utilized instead. These were conducted using the specific study types and the criteria established for each test.
Statistical analysis
The analyses were conducted utilizing R software version 4.2.1 (R Core Team 2022, Austria, Vienna), employing the packages for the meta-analysis. The “metaprop” function was used to assess the prevalence of pre- and postoperative vitamin B1 deficiency, applying inverse variance with Fixed + Random methods. Data on vitamin B1 deficiency was collected at 3, 6, 12, 24, and ≥36 months post-surgery. Forest plots were generated to illustrate the meta-analysis findings and the study heterogeneity. Additionally, the prevalence of vitamin B1 deficiency was evaluated by comparing different surgical procedures and varying postoperative follow-up durations.
Results
A total of 1,338 scientific publications were identified. 166 were eliminated due to duplication, and 1,147 were excluded by filtering the correspondence between titles and abstracts. Thirty-two potentially eligible articles were then obtained and subjected to full-text reading. Finally, 16 publications were selected to validate the risk of bias, final inclusion, and meta-analysis.17–32 (Figure 1).
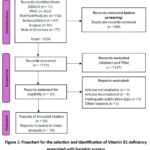 |
Figure 1: Flowchart for the selection and identification of Vitamin B1 deficiency associated with bariatric surgery.Click here to view Figure |
Risk of bias and certainty of evidence
The average quality of the included publications was 7.0 ± 0.71 for randomized controlled trials, 10.3 ± 0.78 for cohort studies, and 7.0 ± 0.0 for cross-sectional studies. Figure 2.
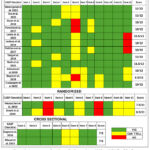 |
Figure 2: Assessment of study quality by applying CASP and JBI Checklist for studies included in the study.Click here to view Figure |
Characteristics of the studies
According to the reported publications, three types of studies are described: randomized controlled studies, cross-sectional studies (prospective and retrospective), and cross-sectional studies. The 16 articles included show a total population size of 3,384 patients undergoing bariatric procedures; in this population, vitamin B1 levels were studied in 2,702 individuals. The characteristics of the studies are summarized in Table 1.
Additionally, the patients were between 18 and 80 years old, evaluating both sexes (male and female), more prevalent among women. Likewise, it was reported that the preoperative BMI was between 35 and 51.7 Kg/m2, and at the postoperative level, values between 28.8 and 40.2 Kg/m2 were recorded. Patients were considered from the preoperative and postoperative intervention period (3 to 48 months) and the types of bariatric surgeries, determining the cumulative prevalence and proportions of patients with vitamin B1 deficiency (Table 1 – Supplementary Material). In bariatric procedures, 12 studies were identified where the Sleeve gastrectomy (SG) technique was implemented, followed by five studies of Roux-en-Y gastric bypass (RYGB), two studies reported Gastric bypass (GB). In contrast, only 1 study reports for Vertical sleeve gastrectomy (VSG), Laparoscopic sleeve gastrectomy (LSG), sleeve gastrectomy with jejunal bypass (SGJB) and sleeve gastrectomy with duodenal-jejunal bypass (SGDJB).
On the other hand, among the most frequent comorbidities, it is reported that 11 studies show the presence of DM type II, 9 studies report hypertension, 7 indicate dyslipidemias, and 5 show sleep apneas. Additionally, rare comorbidities such as gastroesophageal reflux disease (GERD) and fatty liver disease were reported in 3 studies; obstructive sleep apnea syndrome (OSAS) in two studies, and osteoarthritis, hypothyroidism, inflammatory bowel syndrome (IBS), depression, anxiety, and bipolar disorder in a single publication. Finally, it was established that most study patients were supplemented with multivitamin complexes or vitamin B1 products.
Table 1. Main characteristics of the included studies.
| Authors and Date | Type of Study | (n) | Type of bariatric surgery | Duration intervention (month) | Vitamin B1 deficiency (number) | Comorbidities | Treatment | Outcomes (Clinical resolution) |
| Heusschen et al. 2020 17 | A double-blind, randomized controlled trial | 139 | SG | 12 | Pre: 1/128Post: 4/106 | HT, T2DM, DLD, OSAS | MVS | Not resolved |
| Wawrzyniak et al. 2022 18 | Retrospective cohort study | 30 | SG | 9 | Pre: 28/30Post: 4/30 | HD, T2DM, SA, OA. | Supplementation vitamins (Vit. B1) | Reduction in deficiency of vit. B1 |
| Tan et al. 2021 19 | Retrospective cohort study | 215 | SG, SGJB, SGDJB | 12 | Pre: 4/131 | HT, T2DM, DLD | NR | ND |
| Dagan et al. 2016 20 | Cross-sectional analysis | 100 | LSG | 12 | Pre: 6/100 | NAFLD, T2DM, DLD, HT | Dietary supplementation | Not resolved |
| Guan et al. 2018 21 | Retrospective cohort study | 269 | RYGB, SG | 12 | Pre: 74/189Post: 5/31 (RYGB); 5/30 (SG) | HT, T2DM, FL, GERD. | Talcid®, Ilaprazole enteric-coated tablet®, Caltrate ® and Centrum®. | Reduction in deficiency of vit. B1 |
| Punchai et al. 2017 22 | Retrospective cohort study | 47 | RYGB, SG, BPD-DS | 12 | Pre: 30/47Post: 6/47 | HT, SA, DLD, T2DM, FL, depression, anxiety, and BD | Nutritional interventions (vitamin B1) and pharmacotherapy | Partially resolved |
| Lewis et al. 2023 23 | Prospective observational study | 210 | SG, GB | 12 | Pre: 8/90 (SG); 4/64 (GB). Post: 1/86 (SG); 2/48 (GB) | T2DM | Oral micronutrient supplementation (12 mg Vitamin B1) | Decrease in deficiency to 6% |
| Ledoux et al. 2014 24 | Long-term prospective cohort | 144 | GB | 12 | Pre: 22/144. Post: 16/144 | T2DM, HT, DLD, SA | Multivitamin supplements | ND |
| Pellitero et al. 2017 25 | Cohort prospective study | 176 | SG | 12 | Pre: 6/176 Post: 9/176 | Obesity | Standard multivitamin supplementation | Not resolved |
| Wiese et al. 2023 26 | Monocentric cross-sectional study | 35 patients | SG, RYGB | 12 | Post: 0/35 | HT | Micronutrient-based German S3 guideline recommendations | ND |
| Tang et al. 2018 27 | Retrospective cohort study. | 147 | VSG | 12 | Post:27/105 | T2DM, HT, DLD, SA Hypothyroidism, GERD, IBS | 2 Flintstones Complete (3 mg vit. B1 daily) | Postoperative vit. B1 deficiency associated with surgery |
| Smelt et al. 2020 28 | Single-center study | 970 | SG | 12 | Pre: 37/970 Post: 1/223 and 14/594 for UN and UNN. | T2DM, HT, DLD, GERD, OSAS. | 50 mg Vit. B1 daily for 3 months | De novo deficiencies reduced for all WLS Optimum users. |
| Nath et al. 2021 29 | Retrospective cohort study | 33 | RYBP SG | 12 | Post: 20/33 | T2DM | IM and oral Vit. B1 | Not resolved |
| Johnson et al. 2019 30 | Retrospective cohort study | 468 | SG, RYGB | 12 | Pre and Post (SG 10.5% and RYGB 13.7%) | NR | MVS (Including thiamine (Vit. B1) | The highest prevalence of vit. B1 deficiency to 12 months. |
| Boyce et al. 2016 31 | Retrospective cohort study | 309 | LRYGB | 12 | Pre: 8/307Post NCG: 4/123; CG: 1/176) | NR | Vitamin B1 | CG postsurgical was insignificant at 12 months (OR 17%). |
| Culpepper et al 2022 32 | Prospective cohort study | 92 | SG, RYGB | 12 | Pre: 1/56 Post: 1/31 | NR | PatchMD Multivitamin Plus patch (Vitamin B1 to 25 mg) | Mostly resolved |
BD: Bipolar disorder; DLD: Dyslipidemias; GERD: Gastroesophageal Reflux Disease; FL: Fatty liver; HD: Heart disease; HT: Hypertension; MVS: Multi-vitamin and mineral nutritional supplement; NAFLD: Non-alcoholic fatty liver disease; OA: Osteoarthritis; OSAS: Obstructive sleep apnea; Pre: Preoperative; Post: Postoperative; SA: Sleep apnea; T2DM: Type 2 diabetes mellitus; Vit. B1: Vitamin B1.
Pre‑operative prevalence of Vitamin B1 Deficiency
Thirteen scientific publications were included, containing 2,702 individuals, with 267 patients having vitamin B1 deficiency. Statistical analysis of the data established a pooled prevalence of 18% (95% CI: 4–31%, I2 = 98%, p <0.01) (See Figure 3).
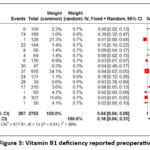 |
Figure 3: Vitamin B1 deficiency reported preoperatively.Click here to view Figure |
Postoperative prevalence of vitamin B1 deficiency
Three months after surgery, the vitamin B1 deficiency was 17% (95% CI: 11–24%, I2 = 25%, p = 0.27) in 25 individuals out of 158 patients. This prevalence decreased to 6% (95% CI: 3–9%, I2 = 66%, p < 0.01) at 6 months, from 63 out of 1282 patients with deficiency. According to data analyzed in 13 scientific publications, 8% (95% CI: 4–12%, I2 = 87%, p < 0.01) of individuals undergoing bariatric surgery showed vitamin B1 deficiency at 1 year after the procedure (Figure 4). After 2 years showed a cumulative prevalence of 2% (95% CI: 0–5%, I2 = 82%, p < 0.01); likewise, this behavior is observed at 48 months, where a cumulative prevalence of 1% is evident (95% CI: 0–2%, I2 = 0%, p = 0.58) (Figure 1S – Supplementary Material).
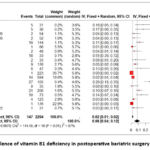 |
Figure 4: Prevalence of vitamin B1 deficiency in postoperative bariatric surgery at 12 months.Click here to view Figure |
Prevalence of postoperative vitamin B1 deficiency and types of bariatric procedures
Analysis of 8 studies in 1473 patients identified 57 cases of vitamin B1 deficiency at 12 months after bariatric surgery (SG), with the random effects model showing a cumulative prevalence of 4% (95% CI: 1–6%, I2 = 76%, p < 0.01). Similarly, 6 studies established that 39 patients had a deficiency in 477 patients undergoing RYGB (pooled prevalence: 12%; 95% CI: 0–25%; I2 = 89%; p < 0.01). While the GB procedure was reported in 2 studies, showing 18 deficient patients out of 192 individuals (pooled prevalence: 8%; 95% CI: 1-15%; I2 = 69%; p = 0.07) (See Figure 5).
On the other hand, comparisons were developed in the intervention times for the SG type of bariatric procedure, showed prevalences was higher in patients after 6 months of the procedure, reaching values of 4% (95% CI: 2–7%, I2 = 65%, p = 0.01), and that when compared with 12 months, the prevalence rates were decreasing; and even at 24 and 48 months, where pooled prevalences of 2% (95% CI: 0–5%, I2 = 82%, p < 0.01) and 1% (95% CI: 0–1%, I2 = 0%, p = 0.58) were established, respectively (See Figure 2S – Supplementary Material). Despite the imprecision in estimating due to the limited data available for assessment, we employed the Egger test to evaluate publication bias regarding the probability of vitamin B1 deficiency in patients receiving RYGB compared to SG after one year.
 |
Figure 5: Prevalence of vitamin B1 deficiency associated with bariatric surgery type. Click here to view Figure |
Discussion
Bariatric surgery demonstrates superior weight loss outcomes relative to non-surgical interventions. Consequently, it ameliorates obesity-related comorbidities, including hypertension, type 2 diabetes mellitus, non-alcoholic steatohepatitis, and obstructive sleep apnea. This intervention correlates with a 42% decrease in cardiovascular risk and a 30% reduction in mortality from alternative causes.33 Some authors have supported these arguments, showing reductions in body weight, BMI, and waist circumference in 5 years, as well as decreased triglyceride levels and insulin requirements.34 Also, in the studies by Pfefferkorn et al.35 the percentage of loss of body mass index was higher in the younger population than in older patients (75.6% vs 69.0%), and there was a lower presence of comorbidities. Similarly, Hasan et al. 36 identified that the mean BMI was 48.2 ± 9.25 in the preoperative period and 30.2 ± 5.97 in the postoperative period, as reported in the generally selected studies.
Despite several procedural kinds, including RYGB and SG, all show significant changes in weight loss as measured by BMI. However, Fatima et al.37 reported that RYGB has a higher percentage of remission of type 2 diabetes mellitus, improved quality of life, and reduced metabolic parameters in the postoperative period compared to patients undergoing VSG. Likewise, randomized studies with limited populations have ensured that despite the comparable results between SG and RYGB regarding weight reduction, resolution of type 2 diabetes, hyperlipidemia, and hypertension, the presence of complications is shown to be lower in SG compared to RYGB.38,39
Despite the benefits of this surgery being reported in multiple studies, micro- or macronutrient deficiencies and malnutrition are common after most of these procedures due to poor nutrient intake or absorption. One of the most important consequences is vitamin B1 deficiency. Vitamin B1 is an essential water-soluble vitamin that the human body does not produce, so it must be supplied through dietary pathways. Vitamin B1 is vital for energy metabolism and neuromuscular function. Its absorption varies by source, occurring through active transport at nutritional doses and passive diffusion at pharmacological doses. The hydrolysis of vitamin B1 by phosphatase is critical for its absorption in the small intestine, particularly in the duodenum and proximal jejunum. Phosphorylated thiamine is subsequently stored in the heart, kidneys, liver, and brain, with a limited half-life of 9 to 18 days.40 The deficiency may remain undetected, failing to identify or treat it promptly, potentially leading to beriberi, characterized by symptoms such as polyneuritis, cardiovascular issues, and Wernicke-Korsakoff neuropsychiatric syndrome.9
Numerous studies have reported elevated incidences of vitamin B1 deficiency in individuals who have undergone bariatric surgery, which is attributed to the structural modifications of the gastrointestinal tract that occur during these procedures. During sleeve gastrectomy, 70-85% of the stomach is removed, resulting in a decreased gastric reservoir size and a faster nutritional transit time, which can reduce nutrient absorption.41 In RYGB, a 30-milliliter pouch is formed from the proximal stomach, and the jejunum is bifurcated, with one segment connected to the newly formed pouch and the other linked to the duodenum to facilitate the entry of pancreatic and biliary secretions into the intestine.42 Therefore, a RYGB procedure would significantly impact the absorption of these vitamins since it excludes the duodenum and part of the proximal jejunum.43 It is also necessary to consider that postoperative gastrointestinal symptoms, such as vomiting and diarrhea, which can be directly associated with the type of bariatric surgery performed, can increase nutrient losses and similarly reduce vitamin B1 absorption. These symptoms are common in the immediate postoperative period and can be prolonged, contributing substantially to the depletion of vitamin B1 reserves.44
Bahardoust et al.9 indicated that 22% of bariatric procedures resulted in vitamin B1 deficiency across the entire sample; furthermore, Roux-en-Y gastric bypass and sleeve gastrectomy exhibited prevalence rates of 25% and 14%, respectively. Unlike Chen (2024), where the prevalence of vitamin B1 deficiency was 2% and Nunes et al.43 who agree that there are no significant differences between the techniques. Furthermore, this study reported that after 3 months, 19% of participants developed a vitamin B1 deficiency. This prevalence decreased to 9% after 6 months, 6% after the first year, and 3% two years after surgery.45
The European Federation of Neurological Societies recommends that, due to postoperative deficiencies, patients’ vitamin B1 levels be monitored for a minimum of 6 months and, if necessary, parenteral supplementation be administered, with standard treatment administered orally at 100 mg twice daily. Patients exhibiting symptoms of Wernicke’s encephalopathy or acute psychosis must be maintained under medical supervision in a hospital setting; they should be administered a minimum of 250 mg/day of vitamin B1 via intramuscular or intravenous route for 3-5 days. A deficit of vitamin B1 following bariatric surgery, when unresponsive to oral supplementation, is linked to increased bacterial proliferation in the small intestine. Antibiotic therapy is required to address this shortage in bariatric beriberi.46 The British Society for Metabolic and Obesity Surgery indicates a lack of adequate data to endorse the evaluation of an individual’s vitamin B1 levels before to surgery; nonetheless, a subset of individuals may exhibit low levels, with 7% demonstrating preoperative vitamin B1 deficiency. Moreover, if post-procedure the patient exhibits fast weight loss, inadequate nutrition, vomiting, alcohol misuse, edema, or neuropathic symptoms, it is advised to initiate therapy for vitamin B1 insufficiency without delay, regardless of pending blood results.47
Conclusion
Bariatric surgery has been shown to positively affect the reduction of body mass index in a few months after the interventions, accompanied by a decrease in cardiovascular risk and morbidity and mortality, also in pathologies such as arterial hypertension, type 2 diabetes mellitus, and dyslipidemias. The studies included in the review have established that preoperative vitamin B1 deficiency may occur in 18% of cases. However, the prevalence of vitamin B1 deficiency at 3 months postoperatively is 17%, even showing a deficiency of 8% after approximately 1 year. This decrease in postoperative prevalence values may be associated with comprehensive dietary control and vitamin supplementation plans. This event is directly related to short and medium-term complications with neurological symptoms, which worsen after bariatric surgery regardless of the type of bariatric procedure because the modalities of sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) also showed a higher prevalence of postoperative neurological symptoms after bariatric surgery (RYGB) showed a vitamin B1 deficiency of 4-12%, respectively.
Acknowledgment
Thanks to the members of GINUMED of the Rafael Nuñez University Corporation.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest-
The author(s) do not have any conflict of interest.
Data Availability Statement
Table 1 with complete information on the studies and supplementary material was uploaded on 10.6084/m9.figshare.28559744.
Ethics Statement –
This research did not involve human participants, animal subjects, or any materials that require ethical approval.
Informed Consent Statement
This study did not involve human participants; therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials
Permission to reproduce material from other sources
Not Applicable
Author Contributions
- Conceptualization and methodology: Neyder Contreras-Puentes, Daniel Meléndez-Díaz and Leonardo Soto-Anaya.
- Analysis and Writing – Original Draft: Angel Tarrá-Marrugo, Yicela Pérez-Loaiza and Maryarena Castro-Leones.
- Visualization and supervision: Dilia Aparicio-Marenco and Neyder Contreras. All authors have contributed significantly and equally to this work.
References
- Sánchez-Carracedo D. Obesity stigma and its impact on health: A narrative review. Endocrinol Diabetes Nutr. 2022;69(10):868-877. doi:10.1016/j.endinu.2021.12.002
CrossRef - Frigolet ME, Dong-Hoon K, Canizales-Quinteros S, Gutiérrez-Aguilar R. Obesidad, tejido adiposo y cirugía bariátrica. Bol Med Hosp Infant Mex. 2020;77(1). doi:10.24875/bmhim.19000115
CrossRef - Lazzati A. Epidemiology of the surgical management of obesity. J Visc Surg. 2023;160(2):S3-S6. doi:10.1016/j.jviscsurg.2022.12.004
CrossRef - Huh YJ, Lee HJ. Metabolic Surgery in Korea. Journal of Metabolic and Bariatric Surgery. 2023;12(2). doi:10.17476/jmbs.2023.12.2.17
CrossRef - Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and Risks of Bariatric Surgery in Adults: A Review. JAMA – Journal of the American Medical Association. 2020;324(9). doi:10.1001/jama.2020.12567
CrossRef - Nath A, Shope TR, Koch TR. Thiamine (Vitamin B1) After Weight Loss Bariatric Surgery. In: Academic Press, ed. Metabolism and Pathophysiology of Bariatric Surgery: Nutrition, Procedures, Outcomes and Adverse Effects. ; 2017:479. doi:10.1016/B978-0-12-804011-9.00037-6
CrossRef - Gomes F, Bergeron G, Bourassa MW, Fischer PR. Thiamine deficiency unrelated to alcohol consumption in high-income countries: a literature review. Ann N Y Acad Sci. 2021;1498(1):46-56. doi:10.1111/nyas.14569
CrossRef - Giblin J, Santos M, Finck C. Thiamine deficiency in an adolescent following bariatric surgery. J Pediatr Surg Case Rep. 2022;79:102233. doi:10.1016/j.epsc.2022.102233
CrossRef - Bahardoust M, Eghbali F, Shahmiri SS, et al. B1 Vitamin Deficiency After Bariatric Surgery, Prevalence, and Symptoms: a Systematic Review and Meta-analysis. Obes Surg. 2022;32(9):3104-3112. doi:10.1007/s11695-022-06178-7
CrossRef - Smith TJ, Johnson CR, Koshy R, et al. Thiamine deficiency disorders: a clinical perspective. Ann N Y Acad Sci. 2021;1498(1):9-28. doi:10.1111/nyas.14536
CrossRef - Polegato BF, Pereira AG, Azevedo PS, et al. Role of Thiamin in Health and Disease. Nutrition in Clinical Practice. 2019;34(4):558-564. doi:10.1002/ncp.10234
CrossRef - Wilson RB. Pathophysiology, prevention, and treatment of beriberi after gastric surgery. Nutr Rev. 2020;78(12):1015-1029. doi:10.1093/nutrit/nuaa004
CrossRef - Rohun J, Dorniak K, Młodziński K, et al. Vitamin B1 Deficiency and Perimyocarditis Fulminans: A Case Study of Shoshin Syndrome in a Woman Following an Unbalanced Dietary Pattern Followed by a Literature Review. Life. 2023;13(1):205. doi:10.3390/life13010205
CrossRef - Ota Y, Capizzano AA, Moritani T, Naganawa S, Kurokawa R, Srinivasan A. Comprehensive review of Wernicke encephalopathy: pathophysiology, clinical symptoms and imaging findings. Jpn J Radiol. 2020;38(9):809-820. doi:10.1007/s11604-020-00989-3
CrossRef - Donnelly A. Wernicke-Korsakoff syndrome: recognition and treatment. Nurs Stand. 2017;31(31):46-53. doi:10.7748/ns.2017.e10440
CrossRef - Eva L, Brehar FM, Florian IA, et al. Neuropsychiatric and Neuropsychological Aspects of Alcohol-Related Cognitive Disorders: An In-Depth Review of Wernicke’s Encephalopathy and Korsakoff’s Syndrome. J Clin Med. 2023;12(18):6101. doi:10.3390/jcm12186101
CrossRef - Heusschen L, Schijns W, Ploeger N, et al. The True Story on Deficiencies After Sleeve Gastrectomy: Results of a Double-Blind RCT. Obes Surg. 2020;30(4):1280-1290. doi:10.1007/s11695-019-04252-1
CrossRef - Wawrzyniak A, Krotki M. The need and safety of vitamin supplementation in adults with obesity within 9 months post sleeve gastrectomy (SG): assessment based on intake. Sci Rep. 2022;12(1):14295. doi:10.1038/s41598-022-18487-z
CrossRef - Tan BC, Park YS, Won Y, et al. Preoperative Nutritional Deficiencies in Bariatric Surgery Candidates in Korea. Obes Surg. 2021;31(6):2660-2668. doi:10.1007/s11695-021-05318-9
CrossRef - Dagan SS, Zelber-Sagi S, Webb M, et al. Nutritional Status Prior to Laparoscopic Sleeve Gastrectomy Surgery. Obes Surg. 2016;26(9):2119-2126. doi:10.1007/s11695-016-2064-9
CrossRef - Guan B, Yang J, Chen Y, Yang W, Wang C. Nutritional Deficiencies in Chinese Patients Undergoing Gastric Bypass and Sleeve Gastrectomy: Prevalence and Predictors. Obes Surg. 2018;28(9):2727-2736. doi:10.1007/s11695-018-3225-9
CrossRef - Punchai S, Hanipah ZN, Meister KM, Schauer PR, Brethauer SA, Aminian A. Neurologic Manifestations of Vitamin B Deficiency after Bariatric Surgery. Obes Surg. 2017;27(8):2079-2082. doi:10.1007/s11695-017-2607-8
CrossRef - Lewis CA, Osland EJ, de Jersey S, et al. Monitoring for micronutrient deficiency after bariatric surgery—what is the risk? Eur J Clin Nutr. 2023;77(11):1071-1083. doi:10.1038/s41430-023-01318-3
CrossRef - Ledoux S, Calabrese D, Bogard C, et al. Long-term evolution of nutritional deficiencies after gastric bypass: An assessment according to compliance to medical care. Ann Surg. 2014;259(6):1104-1110. doi:10.1097/SLA.0000000000000249
CrossRef - Pellitero S, Martínez E, Puig R, et al. Evaluation of Vitamin and Trace Element Requirements after Sleeve Gastrectomy at Long Term. Obes Surg. 2017;27(7):1674-1682. doi:10.1007/s11695-017-2557-1
CrossRef - Wiese ML, Wilke F, Gärtner S, et al. Associations of age, sex, and socioeconomic status with adherence to guideline recommendations on protein intake and micronutrient supplementation in patients with sleeve gastrectomy or Roux-en-Y gastric bypass. PLoS One. 2023;18(3 March):e0282683. doi:10.1371/journal.pone.0282683
CrossRef - Tang L, Alsulaim HA, Canner JK, Prokopowicz GP, Steele KE. Prevalence and predictors of postoperative thiamine deficiency after vertical sleeve gastrectomy. Surgery for Obesity and Related Diseases. 2018;14(7):943-950. doi:10.1016/j.soard.2018.03.024
CrossRef - Smelt HJM, van Loon S, Pouwels S, Boer AK, Smulders JF, Aarts EO. Do Specialized Bariatric Multivitamins Lower Deficiencies After Sleeve Gastrectomy? Obes Surg. 2020;30(2):427-438. doi:10.1007/s11695-019-04191-x
CrossRef - Nath A, Shope TR, Koch TR. Prevalence of Micronutrient Deficiencies in Geriatric Bariatric Patients. Advances in Gerontology. 2021;11:70-76. doi:10.1134/S207905702101046X
CrossRef - Johnson LM, Ikramuddin S, Leslie DB, Slusarek B, Killeen AA. Analysis of vitamin levels and deficiencies in bariatric surgery patients: a single-institutional analysis. Surgery for Obesity and Related Diseases. 2019;15(7):1146-1152. doi:10.1016/j.soard.2019.04.028
CrossRef - Boyce SG, Goriparthi R, Clark J, Cameron K, Roslin MS. Can Composite Nutritional Supplement Based on the Current Guidelines Prevent Vitamin and Mineral Deficiency After Weight Loss Surgery? Obes Surg. 2016;26(5):966-971. doi:10.1007/s11695-015-1853-x
CrossRef - Culpepper T, Lux T, Trivedi S, et al. Prevalence of Postoperative Micronutrient Deficiencies in Bariatric Surgery Patients Who Use Transdermal Patches for Supplementation: A Pilot Study. Cureus. Published online 2022:e25989. doi:10.7759/cureus.25989
CrossRef - Pozo D, Soledad M, Galdeano F. Complicaciones nutricionales de la cirugía bariátrica. Prensa Med Argent. 2022;108(4):209-213.
- Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes — 5-Year Outcomes. New England Journal of Medicine. 2017;376(7):641-651. doi:10.1056/nejmoa1600869
CrossRef - Pfefferkorn U, Hort S, Beluli M, La Vista M, Züger T. Weight Loss After Bariatric Surgery in Different Age Groups. Obes Surg. 2023;33(4):1154–1159. doi:10.1007/s11695-023-06488-4
CrossRef - Hasan NA, Freije A, Abualsel A, Al-Saati H, Perna S. Effect of bariatric surgery on weight loss, nutritional deficiencies, postoperative complications and adherence to dietary and lifestyle recommendations a retrospective cohort study from Bahrain. Sultan Qaboos Univ Med J. 2020;20(3):e344. doi:10.18295/squmj.2020.20.03.015
CrossRef - Fatima K, Farooqui SK, Ajaz I, et al. Sleeve gastrectomy versus Roux-en-Y Gastric Bypass for remission of type 2 diabetes mellitus at 1, 3 and 5 years: a systematic review and meta-analysis. Minerva Gastroenterology. 2022;68(4):450-458. doi:10.23736/S2724-5985.22.03117-5
CrossRef - Meneses E, Zagales I, Fanfan D, Zagales R, McKenney M, Elkbuli A. Surgical, metabolic, and prognostic outcomes for Roux-en-Y gastric bypass versus sleeve gastrectomy: a systematic review. Surgery for Obesity and Related Diseases. 2021;17(12). doi:10.1016/j.soard.2021.06.020
CrossRef - Young MT, Gebhart A, Phelan MJ, Nguyen NT. Use and outcomes of laparoscopic sleeve gastrectomy vs laparoscopic gastric bypass: Analysis of the American college of Surgeons nsqip. J Am Coll Surg. 2015;220(5):880-885. doi:10.1016/j.jamcollsurg.2015.01.059
CrossRef - Dhir S, Tarasenko M, Napoli E, Giulivi C. Neurological, psychiatric, and biochemical aspects of thiamine deficiency in children and adults. Front Psychiatry. 2019;10. doi:10.3389/fpsyt.2019.00207
CrossRef - Miedziaszczyk M, Ciabach P, Szałek E. The effects of bariatric surgery and gastrectomy on the absorption of drugs, vitamins, and mineral elements. Pharmaceutics. 2021;13(12):2111. doi:10.3390/pharmaceutics13122111
CrossRef - Mansoori A Al, Shakoor H, Ali HI, et al. The effects of bariatric surgery on vitamin b status and mental health. Nutrients. 2021;13(4):1383. doi:10.3390/nu13041383
CrossRef - Nunes R, Santos-Sousa H, Vieira S, et al. Vitamin B Complex Deficiency After Roux-en-Y Gastric Bypass and Sleeve Gastrectomy—a Systematic Review and Meta-Analysis. Obes Surg. 2022;32(3):873-891. doi:10.1007/s11695-021-05783-2
CrossRef - Wilson RB. Pathophysiology, prevention, and treatment of beriberi after gastric surgery. Nutr Rev. 2020;78(12):1015-1029. doi:10.1093/nutrit/nuaa004
CrossRef - Karimi Behnagh A, Eghbali M, Abdolmaleki F, Abbasi M, Mottaghi A. Pre- and Post-surgical Prevalence of Thiamine Deficiency in Patients Undergoing Bariatric Surgery: a Systematic Review and Meta-analysis. Obes Surg. 2024;34(2):653-665. doi:10.1007/s11695-023-06896-6
CrossRef - Çalapkorur S, Küçükkatirci H. Vitamin deficiencies and prevention methods after bariatric surgery. Mini-invasive Surgery. 2020;4:15. doi:10.20517/2574-1225.2019.51
CrossRef - O’Kane M, Parretti HM, Pinkney J, et al. British Obesity and Metabolic Surgery Society Guidelines on perioperative and postoperative biochemical monitoring and micronutrient replacement for patients undergoing bariatric surgery—2020 update. Obesity Reviews. 2020;21(11). doi:10.1111/obr.13087
CrossRef
Abbreviations
BMI: Body Mass Index
CI: Confidence intervals
IBS: Inflammatory bowel syndrome
GB: Gastric bypass
GERD: Gastroesophageal reflux disease
JBI: Joanna Briggs Institute
LSG: Laparoscopic sleeve gastrectomy
OSAS: Obstructive sleep apnea syndrome
RDI: Recommended daily intake
RYGB: Roux-en-Y gastric bypass
SG: Sleeve gastrectomy
SGDJB: Sleeve gastrectomy with duodenal-jejunal bypass
SGJB: Sleeve gastrectomy with jejunal bypass
TPP: Thiamine pyrophosphate

