
Manuscript accepted on :19-12-2022
Published online on: 01-12-2023
Plagiarism Check: Yes
Reviewed by: Dr. Liudmila Spirina
Second Review by: Dr. M Mohan Varma
Final Approval by: Dr. Ayush Dogra
Divya Ravikumar1 , Poongodi Chellapandian2, Padmavathy Padmanaban1 and Surapaneni Krishna Mohan3*
, Poongodi Chellapandian2, Padmavathy Padmanaban1 and Surapaneni Krishna Mohan3*
1Department of Obstetrics and Gynaecology, Panimalar Medical College Hospital and Research Institute, Varadharajapuram, Poonamallee, Chennai, Tamil Nadu, India.
2Department of Obstetrics and Gynaecological Nursing, Panimalar College of Nursing, Varadharajapuram, Poonamallee, Chennai, Tamil Nadu, India.
3Departments of Biochemistry, Medical Education, Molecular Virology, Clinical Skills and Simulation, Research, Panimalar Medical College Hospital and Research Institute, Varadharajapuram, Poonamallee, Chennai, Tamil Nadu, India.
Corresponding Author E-mail:krishnamohan.surapaneni@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/2801
Abstract
Background: Coronavirus disease (COVID-19) has become a global pandemic. During any health emergency, the pregnant women and postnatal mothers are more vulnerable for hazards. Hence, it is important to provide them adequate knowledge and good practice guidelines as issued by the World Health Organization. This study was conducted to assess knowledge, attitude and practice against COVID-19 infection among Pregnant and post natal mothers in South Indian population. Materials and Methods: A cross-sectional observational study was conducted in the pregnant women who were in their third trimester and in postnatal mothers delivered within past 3 months. Semi structured questionnaire was used to assess 134 subjects. Results: Out of 134 participants 40(29.9%) had adequate, 43(32.1%) had moderate and 51(38.1%) had inadequate knowledge. The level of practice and attitude towards COVID-19 and its prevention was good (94.8% and 93.3% respectively). There was a significant correlation between knowledge &practices(P=0.023) and practices& attitudes(P=0.000) among the study population. The antenatal mothers had significantly more knowledge than their postnatal counterparts (P=0.044). Age had significant association with knowledge, attitude and level of practice while parity was associated with practice levels alone. It is also evident that some practices of hand hygiene and proper breastfeeding hygiene are lacking among antenatal women and postnatal mothers. Conclusion: By virtue of the findings, it is evident that pregnant women and postnatal mothers lack adequate knowledge about COVID-19 pandemic and its preventive measures as issued by the World Health Organization. Since the knowledge & practices and the practices & attitudes towards COVID-19 are correlated, it is essential that meticulous steps are initiated to provide proper knowledge to the antenatal women and postnatal mothers in order to protect them from COVID-19 infection. We also found that some practices of hand hygiene and proper breastfeeding hygiene are lacking among our women. Steps must be taken to educate and encourage antenatal women and post natal mothers with respect to practices of hand hygiene and proper breastfeeding hygiene during this this ongoingCOVID-19pandemic.
Keywords
Antenatal; COVID-19; Knowledge; Pregnancy; Postnatal; Practice; Pandemic
Download this article as:| Copy the following to cite this article: Ravikumar D, Chellapandian P, Padmanaban P, Mohan S. K. Pregnant Women and Postnatal Mothers Lack Knowledge of COVID-19 and its Preventive Measures. Biomed Pharmacol J 2023;16(4). |
| Copy the following to cite this URL: Ravikumar D, Chellapandian P, Padmanaban P, Mohan S. K. Pregnant Women and Postnatal Mothers Lack Knowledge of COVID-19 and its Preventive Measures. Biomed Pharmacol J 2023;16(4). Available from: https://bit.ly/3N93LBP |
Introduction:
Coronavirus disease (COVID 19) is a communicable disease caused by a newly discovered strain of coronavirus 1. The World Health Organization (WHO) declared it as Public Health emergency of International concern on 30th January 2020 2. India currently has about153178 active cases with COVID-19 infection (till June 16th 2020, 08:00 IST) and these numbers are in increasing trend 3.
During pregnancy and puerperium, women are more susceptible for infections due to changes in body physiology and immunity.The previous epidemics and pandemics of influenza have been detrimental to pregnant and postnatal mothers 4,5. WHO and other organizations like the Centres for Disease Control and Prevention(CDC,USA), National Health Services(NHS,UK), Ministry of Health and Family Welfare (MoHFW, India) have all emphasized that pregnancy and puerperium extra caution while treating this population 6-9. Guidelines and protocols keep changing constantly with new testing, treatment strategies, quarantine policies and even discharge polices 10. Hand hygiene, respiratory etiquette, social distancing, social distancing and self-isolation are preventive stratergies that have proven effective against contracting this virus 6.
Maternal and Child health services are the top priority programmes run by the Government of India and WHO. During this pandemic lot of personnel and infrastructure exclusive for these services had to be utilized for infection control. Many aspects of pregnancy and postnatal care like sterilization, contraception, nutrition, health education, mental healthetc have taken a backseat. Indian mothers are more prone to many illnesses like gestational diabetes mellitus, preeclampsia, preterm labour, anaemia, malnutrition than many of their counter parts in the world 11-13. Though COVID- 19 infection may not directly cause increased harm in pregnancy and puerperium, its impact on day to day activities has been unfavorable. This study was conducted among pregnant and postnatal mothers belonging to southern India to assess their knowledge, attitude and practice towards preventing the transmission of this novel COVID-19 infection.
Methodology
A cross-sectional observational study was conducted at Panimalar Medical College & Research Institute, Varadharajapuram, Poonamallee, Chennai – 600 123 during the period of March 25th, 2020 till May 12th, 2020. Prior approval from the Institution Review Board (IRB) of Panimalar Medical College & Research Institute(PMCH&RI) was taken before commencing the study.Pregnant women who were in their third trimester(from 28 – 42 weeks of gestation) and postnatal mothers who were delivered within past 6 months(delayed postpartum period) attending the Outpatient Department (OPD) of Obstetrics and Gynaecology at Panimalar Medical College Hospital & Research Institute who were willing to provide their informed consent were included in this study. All participants were above the age of 18 years. Participants who didnot provide consent and those pregnant women in their first and second trimester were excluded. Women who had delivered before 6 months from the start of the study were also excluded.
A semi-structured questionnaire was developed and validated by the investigators to assess the knowledge, attitudes and practices against COVID-19 infection among pregnant women and post natal mothers.All the questions/items/statements were taken from standard guidelines as issued by the World Health Organization (WHO) , Indian Council of Medical Research (ICMR) and Ministry of Health and Family Welfare (MoHFW), Government of India.All the salient aspects that needs to be known by the public regarding COVID-19 were incorporated in the questionnaire. After providing the informed consent form, participants were asked to fill up demographic details and advanced to 3 sections consisting of a total number of 27 questions in succession, which were based on knowledge, attitudes and practices regarding COVID-19 pertaining to antenatal and postnatal period. Section-I consists of nine (9) questions pertaining to knowledge on COVID-19 and its impact on pregnancy/puerperium on a two point Likert Scale (True/False). Section-II consists of nine (9) items aimed at assessing the practices of preventive measures during pregnancy/puerperium on a two point Likert Scale (Yes/No). Section-III consists of nine (9) statements that dealt with attitudes towards COVID-19 crisis and its preventive measures in pregnancy/puerperium on a five point Likert Scale. The respondents had to record their responses on the 5-point Likert scale ranging from Strongly Agree(SA)/Agree(A)/Neutral(N)/Disagree(DA)/Strongly Disagree(SD). Each item was given a numerical code to obtain scores for knowledge, attitude and practice of COVID-19 and it preventive measures. The study protocol was approved by the Institutional Review Board (IRB) of the Panimalar Medical College Hospital & Research Institute, Chennai (Panimalar Medical College Hospital & Research Institute IRB #1/2020/016) and conformed to the requirements of the Declaration of Helsinki (as revised in Seoul 2008).
After completing the questionnaire, a brief counselling session was given to all the participants of the study by the medical officer of the Department of Obstertics&Gynaecolgy with regard to the COVID-19 pandemic and its preventive measures. Helpline numbers of the institution were also provided to these women so that any doubts regarding antenatal care, delivery, postpartum, vaccination, mental health and other emergencies can be addressed 24 x7. Information regarding the spectrum of symptoms of COVID-19 and need for early testing and isolation were also given.
Statistical Analyses
All categorical variables were presented as numbers and percentages. Descriptive analysis was performed and data were reported as Mean and Standard Deviation for continuous variables and frequency distributions for categorical variables. Correlation, non-parametric tests for Kruskal-Wallis and Analysis of Variance (ANOVA) tests were performed to compare the differences in the variables. Spearman’s rho test was used to measure the strength and direct relationship between two variables. Chi-square test was done to assess the association between categorical variables. Statistical significance was set at p<0.05. All statistical analyses were performed using Statistical Package for Social Science (SPSS version 17) for Microsoft Windows, SPSS Inc. USA.
Results
134 pregnant women in their third trimester and postnatal mothers participated in this study. The mean age of the participants who participated was of 29.12 (±4.862) years. Participants below or equal to the age of 25 years were 23, 26-30 were 78 and > 30 years were 33. In our study, 51(38.1%) of women were primigravida, 59(44%) had 1 child and 24(17.9 %) had more than one children. Among the participants in our study, 85(63.4%) of them were professionals, 10(7.5%) were self-employed and 39 (29.1%) were housewives. With regard to the educational qualification, 68(50.7%) were postgraduates, 35(26.1%) were undergraduates, 10(7.5%) were doctorates,8(6.0%) were diploma holders, 8 (6%)were educated up to 12th standard, 4 (3.3%) were educated up to 10th standard, 1 (0.7%) had no formal education. Among the participants recruited 106(79.1%) were antenatal mothers in their third trimester and 28(20.9%) were postnatal mothers who delivered upto 12 weeks prior to the start of the study (Table 1.)
Table 1: Demographic characteristics of the women included in the study.
|
Demographic variable |
Frequency |
Percentage |
|
Age ≤25 years 26-30 years ≥30 years |
23 78 33 |
17.2 58.2 24.6
|
|
Parity 1 2 3 None |
59 21 3 51 |
44.0 15.7 2.2 38.1 |
|
Whether Antenatal(AN) or Post natal(PN) AN PN |
106 28 |
79.1 20.9 |
|
Occupation Professional Self employed Housewife |
85 10 39 |
63.4 7.5 29.1 |
|
Education No formal Education Upto 10th Upto 12th Diploma Undergraduate Postgraduate Doctorate |
1 4 8 8 35 68 10 |
0.7 3.0 6.0 6.0 26.1 50.7 7.5 |
Level of knowledge about COVID-19
In our study, out of 134 participants 40(29.9%) had adequate, 43(32.1%) had moderate and 51(38.1%) had inadequate knowledge (Figure 1). The statement” Pregnant women are at a higher risk of COVID-19” infection had the maximum wrong response and “Pregnant women must be prioritized for COVID-19 testing” had the maximum right response at 75.4 and 87.3% respectively. “Pregnant woman should attend regular frequent visits if they are residing in a cluster area”,” COVID-19 infection can be passed on from mother to child during pregnancy”, “COVID-19 infection can be passed on from mother to child through breast milk ,” breastfeeding should be avoided if a mother is mild/ asymptomatic COVID-19 positive” had equivocal 44%,48.5%, 53%,47% right responses. “Regular medications and vaccinations should be avoided during COVID-19 pandemic among pregnant women “was answered correctly by 70.1% of mothers and “there is no specific dietary recommendations to prevent COVID-19 infections among pregnant women” was answered correctly by 66.4%. 79.1% of the mothers felt that normal delivery was possible in pregnant women with COVID-19 infection (Table 2).
Table 2: Statements to assess the knowledge of COVID-19 among pregnant and postnatal mothers.
|
Statement |
Response |
Frequency |
Percentage |
|
Pregnant women are at a higher risk of COVID-19 infection. |
True False |
101 33 |
75.4 24.6 |
|
Pregnant women must be prioritised for COVID -19 testing. |
True False |
117 17 |
87.3 12.7 |
|
Pregnant should attend regular and frequent antenatal visits if they are residing in a clusterarea. |
True False |
75 59 |
56.0 44.0 |
|
Regular medications and vaccinations should be avoided during COVID-19 pandemic amongpregnant women. |
True False |
40 94 |
29.9 70.1 |
|
There is no specific dietary recommendation to prevent COVID-19 infection amongpregnantwomen. |
True False |
89 45 |
66.4 33.6 |
|
If a pregnant women has COVID-19 infection, normal delivery is not possible. |
True False |
28 106 |
20.9 79.1 |
|
COVID-19 infection can be passed on from mother to child during pregnancy. |
True False |
69 65 |
51.5 48.5 |
|
COVID-19 infection can be passed on from mother to child through breast milk. |
True False |
63 71 |
47.0 53.0 |
|
Breastfeeding should be avoided if a mother is mild/ asymptomatic COVID-19 positive. |
True False |
71 63 |
53.0 47.0 |
Practice of preventive measures against COVID-19
In our study, 118(88.1%) had good level of practice of preventive measures against COVID-19. 9(6.7%) had average and 7(5.2%) had poor levels of practice of preventive measures against COVID-19(Figure 1). 130(97%) responded that they wear a mask while they travel outside and 128(95.5%) avoided non-essential travel. 113(84.3%) of women practiced social distancing, 114(85.1%) avoided touching of face unnecessarily, 123(91.8%) preferred to work from home, 124(92.5%) restricted visitors to their homes. 127(94.8%) of pregnant women were aware of symptoms of COVID-19 infection, 119(88.8%) had the intention to handle their babies with care following hand and respiratory hygiene. The minimum response of given to the practice of hand washing 4-5 times/day for 20seconds with 107(79.9%) of pregnant and postnatal mothers (Table 3).
Table 3: Questions to assess the level of practice of measure against COVID-19 among Pregnant and postnatal mothers
|
Questions |
Response |
Frequency |
Percentage |
|
Do you wash your hands 4-5 times a day for 20secs with soap and water? |
Yes No |
107 27 |
79.9 20.1 |
|
Do practice social distancing of 1metre when you meet others? |
Yes No |
113 21 |
84.3 15.7 |
|
Do you avoid touching your face unnecessarily? |
Yes No |
114 20 |
85.1 14.9 |
|
Do you wear a mask while traveling outside? |
Yes No |
130 4 |
97.0 3.0 |
|
Do you avoid non-essential travel?
|
Yes No |
128 6 |
95.5 4.5 |
|
Do you prefer to work from home than travel to your place of work?
|
Yes No |
123 11 |
91.8 8.2 |
|
Have you restricted the visitors coming to your home? |
Yes No |
124 10 |
92.5 7.5 |
|
Are you aware of the symptoms of COVID-19 infection? |
Yes No |
127 7 |
94.8 5.2 |
|
Do you (intend to) handle your baby by following hand and respiratory hygiene measure? |
Yes No |
119 15 |
88.8 11.2 |
Attitude towards COVID-19 and its prevention
Our present study with 134 participants, 110(82.1%) had adequate, 15(11.2%) had moderate and 9 (6.7%) had inadequate attitude towards COVID-19 prevention (Figure 1). The mean attitude among the study population was 37.04±6.077. The statement “I have to be more careful than others during COVID-19 pandemic to protect myself and my family” was strongly agreed upon maximally and statements” COVID-19 testing must be done if you are due for delivery in a high risk area”, “active testing of people can help in control of COVID-19 infection”, “I am comfortable to get tested for COVID-19 infection “ had the maximum strongly disagreed response of 10.4% by the subjects. The statements to assess the attitude towards COVID-19 infection are postulated in the (Table 4).In our study we also found that there was significant correlation between knowledge &practice at P=0.038 and practice &attitude at P<0.01(Table 5) among the study population.
 |
Figure 1: Knowledge, attitude and practices of COVID-19 and its preventive measures among pregnant and postnatal mothers. |
Table 4: Statements to assess the attitude towards COVID-19 infection
|
Statements |
Response |
Frequency |
Percentage |
|
COVID-19 testing must be done if you are due for delivery in a high risk area. |
SA A N D SD |
78 32 8 2 14 |
58.2 23.9 6.0 1.5 10.4 |
|
I have to be more careful than others during this COVID-19 pandemic to protect myself and my child. |
SA A N D SD |
99 19 3 0 13 |
73.9 14.2 2.2 0 9.7 |
|
Following government norms on hand and respiratory hygiene reduces the risk of COVID-19 infection. |
SA A N D SD |
76 40 5 0 13 |
56.7 29.9 3.7 0 9.7 |
|
Active testing of people can help in control of COVID-19 infection. |
SA A N D SD |
66 37 13 4 14 |
49.3 27.6 9.7 3.0 10.4 |
|
I am comfortable to get tested for COVID-19 infection. |
SA A N D SD |
55 48 15 2 14 |
41 35.8 11.2 1.5 10.4 |
|
My family has shown full support during this COVID-19 lockdown and taken good care of me. |
SA A N D SD |
91 29 3 6 5 |
67.9 21.6 2.2 4.5 3.7 |
|
COVID-19 lock down and other preventive measures have affected my family. |
SA A N D SD |
47 27 33 23 4 |
35.1 20.1 24.6 17.2 3.0 |
|
During this COVID-19 crisis, my household work has increased. |
SA A N D SD |
61 35 23 11 4 |
45.5 26.1 17.2 8.2 3.0 |
|
Even if COVID-19 infection is controlled, I have fear to go back to my previous lifestyle. |
SA A N D SD |
60 40 21 9 4 |
44.8 29.9 15.7 6.7 3.0 |
(SA-strongly agree, A-Agree,N-neutral,D-disagree,SD-Strongly Disagree)
Table 5: Correlation between knowledge, practice and attitude among the pregnant and postnatal mothers.
|
Variables |
Pearson correlation |
Spearman’s rho |
|
Knowledge & Practice |
r=0.197 P=0.023 |
rs=0.179 P=0.038 |
|
Practice & Attitude |
r=0.640 P<0.01 |
rs=0.371 P<0.01 |
|
Attitude & Knowledge |
r=0.065 P=0.458 |
rs=-0.043 P=0.619 |
In our present study, we found that participants between 26-30 years had significantly higher knowledge. But, women above 30 years had higher levels of practice and better attitude against COVID-19 and its prevention. Hence, age had a significant association with level of knowledge, practice and attitude among the subjects(P=0.042,0.013and 0.031 respectively)(Table 6). We found that women with more children had higher the levels of practice of preventive measures (P=0.012). Level of knowledge and attitude showed no statistically significant association with parity in our study (Table 6).
Table 6: Associations between various demographic variables with level of knowledge, Attitude and practice among Pregnant and postnatal mothers in our study.
|
Variables |
N |
Mean |
Test of Significance |
||||||||
|
K |
P |
A |
ANOVA |
Kruskal-Wallis |
|||||||
|
V |
F |
P |
v |
Chi-square |
P |
||||||
|
Age ≤25 years 26-30 years ≥30 years |
23 78 33 |
4.35 5.51 5.06 |
7.26 8.18 8.48 |
33.3937.50 38.52 |
|
||||||
|
K P A |
3.552 4.280 5.720 |
0.031 0.016 0.004 |
K P A |
6.354 8.670 6.960 |
0.042 0.013 0.031 |
||||||
|
Parity 1 2 3 None |
59 21 3 51 |
5.29 4.62 4.33 5.39 |
8.25 8.48 9.00 7.71 |
37.92 37.43 42.67 37.04 |
K P A |
1.068 1.893 2.390 |
0.365 0.134 0.072 |
K P A |
3.430 10.958 6.587 |
0.330 0.012 0.086 |
|
|
Occupation Professional Self-employed Housewife |
85 10 39 |
5.38 5.10 4.85 |
8.36 7.50 7.67 |
38.00 35.20 35.44 |
K P A |
1.046 3.301 2.963 |
0.354 0.040 0.055 |
K P A |
2.602 2.724 4.001 |
0.272 0.256 0.135 |
|
|
Education No formal education Upto 10th 12th Diploma Undergraduate Postgraduate Doctorate
|
1 4 8 8 35 68 10
|
7.00 4.75 3.38 3.88 5.14 5.53 5.70 |
9.00 8.50 8.75 6.50 8.06 8.15 8.40 |
45.00 39.00 39.50 32.00 35.54 37.62 38.90 |
K P A |
2.689 1.719 2.219 |
0.017 0.122 0.045 |
K P A |
15.488 7.556 10.068 |
0.17 0.273 0.122 |
|
Among the antenatal women, we observed no significant difference in attitude and practice.34.9% had inadequate knowledge, 30.2% had moderate and34.9% had adequate knowledge among Antenatal women and 50% had inadequate, 32.1% and 10.7% had adequate knowledge among postnatal mothers (Figure-2&3). This showed a statistically significant association of P=0.044(Table 7).
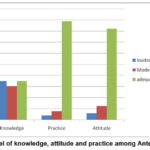 |
Figure 2: Level of knowledge, attitude and practice among Antenatal women. |
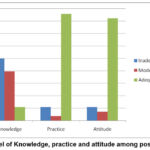 |
Figure 3: Level of Knowledge, practice and attitude among postnatal women. |
Table 7: Association between Antenatal and postnatal mothers with knowledge, practice and attitude.
|
Variable |
N |
Mean |
Test of significance |
|||
|
Mann Whitney |
Chi-Square |
|||||
|
Antenatal Women |
106
|
K P A |
5.34 8.07 37.01
|
MR |
P |
P 0.044 0.274 0.506 |
|
70.34 64.84 66.48 |
0.096 0.071 0.553
|
|||||
|
Postnatal mothers |
28 |
K P A |
4.68 8.21 37.18 |
56.75 77.57 71.36 |
||
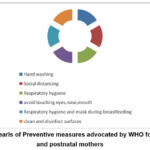 |
Figure 4: Pearls of Preventive measures advocated by WHO for pregnant and postnatal mothers |
Discussion
COVID-19 infection is highly contagious and has emerged as a global pandemic. Prevention and treatment of pregnant women and post natal mothers with COVID-19 infection is a major concern for the medical fraternity14. Information regarding prevention and treatment of COVID-19 disease in pregnant and postnatal mothers have been devised by global organizations like World Health Organization (WHO), the International Federation of Gynaecology and Obstetrics(FIGO)etc6,15. These guidelines have been taken up by all countries and their own modified versions with respect to the logistics and extent of disease spread have been devised. In India, the Ministry of Health and Family Welfare (MoHFW) has periodically reviewed the situation and provides information for the public to adopt to fight this global pandemic and protect our women3. It is important that the public are aware of these guidelines properly and do not get misleading information.
In our study, we found that 38.1% women with inadequate knowledge regarding information pertaining to COVID-19 and pregnancy/puerperium. The guidelines released by WHO have stated that frequent hand washing with soap and water or alcohol based hand rub, practicing social distancing of at least 1 meter, avoiding unnecessary handling of face, covering of the nose and mouth while coughing or sneezing with elbow or tissue can help pregnant women from protecting themselves from COVID-19 infection6. In addition to the above information, The Ministry of Health and Family Welfare (MoHFW), Government of India have emphasized on the use of facial masks for individuals with risk and avoiding non-essential travel(3). Many local governing bodies within the country have advised individuals in ‘hotspots’ formandatory universal wearing of masks while coming out of their homes(16). Vertical transmission of COVID-19 virus from the mother to the fetus and spread of the virus through breast milk has not been documented till date14,17. Proper hand hygiene and usage of masks appropriately prevents transmission of the virus during breastfeeding if the mother is COVID-19 positive. WHO has emphasized that early rooming in and exclusive breastfeeding helps the baby to thrive and should be encouraged17. WHO and FIGO have stated that currently pregnancy and puerperiumdoes not increase risk for serious infection5,15. This can be thought as a ray of hope in this gloomy situation because previous epidemics and pandemics of Influenza have been very adverse to the pregnant population. WHOhas also clearly stated that maternity and reproductive health services should run uninterrupted during this pandemic18. But, practically due to lockdown situation and fear of infection, the number of hospital visits as well as home based services have taken a toll. Tele-consultation is now advocated in areas where the case load is high 19. The MoHFW has emphasised in its bulletin on essential services during COVID-19 that Iron and folic acid tablets, Calcium tablets and other medications for high risk pregnancies and postnatal mothers must be supplied uninterrupted9. Vaccination and contraception services should also be provided under essential care with precautions to be followed in the containementareas20,21. WHO has reiterated the need for a well-balanced nutritious diet among the antenatal women and postnatal mothers. Ministry of AYUSH,India has postulated lifestyle modifications like yoga, breathing exercises and herbal tea supplements for immunity boost against COVID-19. But these cannot be advised for pregnant and postnatal mothers without robust evidence22. Previously, ICMR had advised testing for all pregnant women due to deliver in 5 days to get tested, but changed its position to test only for symptomatic women23. Cesarean section for women with mild/moderate COVID-19 infection should be done only for obstetric indications9. Donning of personal protection equipment (PPE) and the availability of personnel in case of dire emergencies must be kept in mind while making decisions regarding mode of delivery.
In our study, we found that 118(88.1%) had good level of practice of preventive measures against COVID-19. This can be attributed to the usage of social media and mass communication for constantly campaigning for hygienic practices. In a country like India with 1.3 billion people, were the average population density is has high as 382/kilometer2 24, steps like early lockdown and sensitization of public regarding the sanitary practices has helped individuals to adopt them. 94.8% of pregnant women were aware of symptoms of COVID-19 infection and 88.2% had the intention to handle their babies with care following hand and respiratory hygiene. This aids in curtailing the infection among this vulnerable group of population. But in our study, we found that only 79.9% practiced proper hand hygiene which is the single most important step to prevent transmission of COVID-19 infection. COVID-19 spreads through droplet infection and fomites18. Hand washing with soap and water or alcohol based hand rub has been proven to effectively curb the virus. Hence, pregnant women and postnatal should adopt proper hand hygiene to protect themselves. It is important to note that all these practices should be collectively performed by all the people in the community in order to effectively control the infection(Figure 4). Non adherence to anyone of these preventive measures can lead to contracting the infection voluntarily.
In this present study ,majority of pregnant and postnatal mothers had adequate positive attitude towards COVID-19 prevention. There were significant correlation between knowledge and attitude (P=0.043) in our study. Significant correlation between practice & attitude was observed P<0.01.This proves to show that as we provide our pregnant women with adequate knowledge, they are able to cope up with this unprecedented situation better. Better attitude bringing about better practices and vice versa. Majority of them showed positive attitude towards testing and control of infection. 55.2% agreed that COVID-19 crisis had an impact on their family. It is important that the journey of pregnancy and childbirth makes our women feel empowered. The WHO has persistently stressed upon respectful maternity care were the health care community and her family provides constant support with dignity25,26.Interestingly we found that 71.6% of our participants felt that their household chores has increased during this crisis. It is understandable that since lockdown and measures to reduced movement of people have been advocated as a step to curtail infection, domestic work at homes increases. During these tough times support from the family and sharing of work may provide relief to women.
In our present study, we found that participants between 26-30 years had significantly higher knowledge. This may be attributed to the increased exposure to internet and social media among this group. Women above 30 years had higher levels of practice at P=0.016 and attitude at P=0.004. This may be due to slightly higher level of experience and maturity. Hence, age had a significant association with level of knowledge, practice and attitude among the subjects towards COVID-19 and its prevention. Higher the parity, higher the levels of practices of preventive measures was observed in our study (P=0.012). This can be due to adopting some of these hygienic methods with their previous child rearing experience. We observed that working professional had significantly higher levels of practice of the preventive stratergies. Government has given clear and mandatory guidelines that needs to be adopted very strictly at places of employment and hence it might have been obligatory to follow these preventive measures.
34.9% had inadequate knowledge, 65.1% had adequate knowledge among antenatal women and 50% had inadequate and 50% had adequate knowledge among postnatal mothers which had statistically significant association. Apprehension towards delivery and risk to the unborn which might have made pregnant women to seek for information regarding COVID-19 and changing scenarios may have been the reasons for the slightly higher level of knowledge among antenatal mothers.
Recommendations
While guidelines are constantly being updated, it is important that the people are also sensitised with the same information. Hence, periodically studies should to be done regarding knowledge and adherence to government policies to prevent further worsening of the pandemic. Elaborate demographic descriptions may help in implementing targeted approach in areas where knowledge and practices needs to be improved.
Limitations
This study was done on women attending the outpatient clinic at Department of Obstetrics and Gynaecology at Panimalar Medical College Hospital & Research Institute, Chennai, Tamil Nadu, India. A larger recruitment may provide more meaningful resultsso as to be generalized to the whole population.Pregnant women in their third trimester and puerperium were involved in the study.
Conclusion
In our study, we found that pregnant and postnatal mothers lack adequate knowledge about COVID-19 pandemic and its preventive measure. We also established that knowledge &practices; practices and attitudes towards COVID-19 are correlated with eachother. Hence, it is essential that meticulous steps are taken to provide proper knowledge to our pregnant and postnatal population in order to protect them from COVID-19 infection. We also found that some practices of hand hygiene and proper breastfeeding hygiene are lacking among our women. Steps must be initiated to encourage these preventive measures to fight with this on-going pandemic and COVID-19 crisis.
Acknowledgments
We are thankful to Dr. S. Porchelvan, MSc, MBA, PGDCA, PhD, Professor in Biostatistics for assisting with the statistical analyses.
Conflict of Interest
The authors declare that there is no conflict of interest.
Funding Sources
There is no funding sources.
References
- WHO, 2020a. Health topics/coronovirus URL https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed 16thJune 2020).
- WHO,2020b.Newsroom/detail URL https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed 16thJune 2020)
- MoHFW, 2020a. URL https://www.mohfw.gov.in/ (accessed on 16th June 2020 08:00IST)
- Mak TK, Mangtani P, Leese J, Watson JM, Pfeifer D. Influenza vaccination in pregnancy: current evidence and selected national policies. The Lancet infectious diseases. 2008 Jan 1;8(1):44-52.
CrossRef - Van Kerkhove MD, Vandemaele KA, Shinde V, Jaramillo-Gutierrez G, Koukounari A, Donnelly CA, Carlino LO, Owen R, Paterson B, Pelletier L, Vachon J. Risk factors for severe outcomes following 2009 influenza A (H1N1) infection: a global pooled analysis. PLoS medicine. 2011 Jul;8(7).
CrossRef - WHO, 2020b. Q&A pregnancy, Childbirth and Covid-19 URL https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-on-covid-19-pregnancy-and-childbirth (accessed on 16thJune 2020)
- CDC, 2020 URL https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/pregnancy-breastfeeding.html (accessed 16thJune 2020)
- RCOG, 2020 URL https://www.rcog.org.uk/en/guidelines-research-services/guidelines/coronavirus-pregnancy/covid-19-virus-infection-and-pregnancy/ (accessed 16th June2020)
- MoHFW, 2020b. EssentialservicesduringCOVID19updated041120.pdf (Accessed 16th June 2020)
- MoHFW, 2020c. Clinical management protocol.pdf ReviseddischargePolicyforCOVID19.pdf (accessed 16thJune 2020)
- Seshiah V, Balaji V, Balaji MS, Paneerselvam A, Arthi T, Thamizharasi M, Datta M. Prevalence of gestational diabetes mellitus in South India (Tamil Nadu): a community based study. JAPI. 2008 May 15;56:329-3.
- Bentley ME, Griffiths PL. The burden of anemia among women in India. European journal of clinical nutrition. 2003 Jan;57(1):52-60.
CrossRef - Malik A, Jee B, Gupta SK. Preeclampsia: Disease biology and burden, its management strategies with reference to India. Pregnancy hypertension. 2019 Jan 1;15:23-31.
CrossRef - Qiao J. What are the risks of COVID-19 infection in pregnant women?. The Lancet. 2020 Mar 7;395(10226):760-2.
CrossRef - FIGO, 2020 URL https://www.figo.org/news (accessed 16thJune 2020)
- Covid19.chennaicorporation, 2020. URL http://covid19.chennaicorporation.gov.in/c19/index.jsp (accessed 16thJune 2020)
- WHO ,2020c. URL https://www.who.int/reproductivehealth/publications/emergencies/COVID-19-pregnancy-ipc-breastfeeding-infographics/en/ (accessed 16thJune 2020)
- World Health Organization. Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations: scientific brief, 27 March 2020. World Health Organization; 2020. (accessed 16th June 2020)
CrossRef - ICMR, 2020 b. URL: Guidance_for_Management_of_Pregnant_Women_in_COVID19_Pandemic_12042020,pdf. (accessed 16th June 2020)
- MoHFW, 2020d. URL https://www.mohfw.gov.in/GuidanceNoteonProvisionofessentialRMNCAHNServices24052020.pdf (accessed 16th June 2020)
- MoHFW 2020e. URL https://www.mohfw.gov.in3ImmunizationServicesduringCOVIDOutbreakSummary150520202.pdf (accessed 16th June 2020)
- Ayush ,2020.URL https://www.ayush.gov.in/ (accessed 16thJune 2020)
- ICMR, 2020a. Covid-19 testing stratergies. URLhttps://main.icmr.nic.in/content/covid-19 (accessed 16thJune 2020)
- Censusindia, 2020 URLhttps://censusindia.gov.in/Census_And_You/area_and_population.aspx(accessed 16th June 2020)
- Alliance WR. Respectful maternity care. Essential obstetric and newborn care toolkit. USAID maternal and child health integrated program. 2011.
- Reis V, Deller B, Catherine Carr CN, Smith J. Respectful maternity care. Country experience.Database – Alliance francophone pour l’accouchementrespecté (AFAR)

