
Manuscript accepted on :10-10-2023
Published online on: 14-11-2023
Plagiarism Check: Yes
Reviewed by: Dr R Rajalakshmi
Second Review by: Dr. Moumita Hazra and Dr. P. Shivakumar
Final Approval by: Dr. Patorn Piromchai
Tahani Hassan1* , Nadine Alhumaidan1, Basher Yousef1, Mariam Alsalhi1, Abdulrahman Albulayhi2 and Sultan Al Harbi3
, Nadine Alhumaidan1, Basher Yousef1, Mariam Alsalhi1, Abdulrahman Albulayhi2 and Sultan Al Harbi3
1Department of Pharmacology and Toxicology, College of Pharmacy, Qassim University, Buraidah, KSA.
2Diabetes and Endocrinology Center ,Buraydah, King Fahad Specialist Hospital (KSA).
3Diabetes and Endocrinology Center, Unaizah, King Saud Hospital (KSA).
Corresponding Author E-mail:tahani-ibrahim@hotmail.com
DOI : https://dx.doi.org/10.13005/bpj/2821
Abstract
Diabetes can affect many different organs in the body and may lead to serious complications. Many studies related vitamin D deficiency to the occurrence Type 2 diabetes complications. However, the link between diabetic complications and vitamin D deficiency is under debate. Therefore this study aimed to evaluate the clinical relevance of vitamin D levels on diabetic complications. This retrospective cross-sectional study was conducted on 252 patients followed at King Fahd Specialist Hospital in Buraydah and King Saud Hospital in Unaizah, Saudi Arabia. The participants were divided into five groups: Non-diabetic group, diabetic without complications, diabetic nephropathy, diabetic peripheral neuropathy, and diabetic retinopathy. 78.3% of diabetic neuropathy showed vitamin D deficiency compared to diabetic nephropathy (75%), retinopathy (56.9%), and diabetics without complications (31.4%). Vitamin D deficiency was higher in diabetic patients with complications (69.8%) compared to those without complications (31.4%). Moreover 39.2% of diabetics without complications showed normal vitamin D level compared with 13.4% of diabetics with complications. The results showed that vitamin D deficiency was significantly associated with diabetic complications.
Keywords
Diabetic complications; Type 2 diabetes; Vitamin D deficiency
Download this article as:| Copy the following to cite this article: Hassan T, Alhumaidan N, Yousef B, Alsalhi M, Albulayhi A, Harbi S. A. The Association between Vitamin D Status and Diabetic Complications in Type 2 Diabetic Patients. Biomed Pharmacol J 2023;16(4). |
| Copy the following to cite this URL: Hassan T, Alhumaidan N, Yousef B, Alsalhi M, Albulayhi A, Harbi S. A. The Association between Vitamin D Status and Diabetic Complications in Type 2 Diabetic Patients. Biomed Pharmacol J 2023;16(4). Available from: https://bit.ly/47aerIl |
Introduction
Vitamin D is a fat-soluble vitamin which comprises two forms, vitamin D2 (ergocalciferol ) and vitamin D3 (cholecalciferol ) 1, 2. Vitamin D play pivotal role in humans’ body, like modulation of cell growth, immune function, and glucose metabolism 1, 3. Vitamin D deficiency affects almost half of the population worldwide. In Saudi Arabia it represent a serious public health issue as it affect all ages including elderly, woman, men, and school children 4.
The committee of Food and Nutrition Board (FNB) specified vitamin D deficiency at concentrations less than 30 nmol/L (12 ng/mL); insufficiency at 30 to 50 nmol/L (12–20 ng/mL), and sufficient at 50 nmol/L (20 ng/mL) or more 3. Some studies linked inadequacy level of vitamin D other conditions such as CVD, hypertension, autoimmune diseases, cancer, and insulin resistance, which related to type 2 diabetes, and its complications 1. Type 2 diabetes mellitus (T2DM) is a heterogenous metabolic disorder which characterize by impairment of insulin secretion, insulin action, or both. It involve dysfunction of pancreatic beta cell , systemic inflammation, and elevated blood glucose levels 5. T2DM is considered as the most prevalent type of diabetes, affecting 90-95% of all diabetic patients 6. In Saudi Arabia, a review study reported that by 2030 the prevalence of T2DM is expected to reach 45.8% 7. In Saudi vision 2030, it was considered as one of the three major chronic diseases that threaten public health 8 .
Diabetic complications are classified to microvascular complications, which related to damage to small blood vessels e.g in nervous system (neuropathy), renal system (nephropathy) and eye (retinopathy) and macrovascular complications due to damage to the arteries which involve peripheral vascular disease , coronary artery disease, and cerebrovascular disease 9,10 .
Previous studies reported relationship between vitamin D and T2DM, and there is evidence that vitamin D contributes to the onset of diabetes 11, 12. Several studies connected vitamin D deficiency to the occurrence T2DM complications 1. A cross-sectional study done in Jazan documented a positive relation between diabetic retinopathy and vitamin D deficiency , however other findings suggested that diabetic neuropathy and diabetic nephropathy are not linked with vitamin D deficiency in patients with T2DM 13 . Nevertheless, the nature of the relationship between vitamin D deficiency and developing diabetic complications is under debate. Therefore, the aim of this study was to evaluate the clinical relevance of vitamin D levels on diabetic complications.
Methods
Study design
This retrospective cross-sectional study was conducted on patients followed at endocrinology clinics of King Fahd Specialist Hospital and King Saud Hospital / Saudi Arabia. The participants were divided into five groups (each group 50 patients) as follow: None diabetic (ND), Diabetic without complications (D w/o C), Diabetic with nephropathy (DN), Diabetic with peripheral neuropathy (DPN), and diabetic retinopathy (DR).
The study was approved by Qassim Regional Ethical Committee (Reg. No 607-43-1112). Anthropometric and laboratory measurements were retrieved from the patients’ records in a predesigned data collection form.
Inclusion and exclusion criteria
The study included type 2 diabetic patients of both genders. Patients were excluded if they have Type 1 DM, HbA1c or serum vitamin D level missing data, Osteomalacia, chronic kidney disease, vitamin D or calcium supplementation, nutrition supplements that affected vitamin D metabolism, pregnancy, and lactation.
Statistical analysis
The results were presented as numbers and frequencies for categorical variables, mean ± standard deviation (SD) for continuous variables. The comparisons between groups were performed using Chi-squared test for categorical variables, and one-way analysis of variance (ANOVA) for continuous variables. Statistical significance is considered at P value ≤ 0.05.
Results
This study included 252 participants with age ranged from 18 to 87 years. 54.8% of the participants were females and the rest were males. Females were predominant among DR and diabetic with no complications groups (66.7% for each). Regarding BMI, 41.7% of the participants were obese, 34.9% overweight, and 23.4% with normal weight. Obesity was highest among DPN followed by DR and diabetic with no complications (P=0.036) [Table 1].
Table 1: Demographic data of study group (N= 252)
|
Bio-demographic data |
Total |
Groups |
p-value |
||||
|
ND (n=52) |
Dw/oC (n=51) |
DN (n=52) |
DPN (n=46) |
DR (n=51) |
|||
|
No (%) |
|||||||
|
Age in years |
|
|
|
|
|
|
0.001*$ |
|
< 40 |
30 (11.9) |
18 (34.6) |
2 (3.9) |
1 (1.9) |
1 (2.2) |
8 (15.7) |
|
|
40-59 |
101 (40.1) |
23 (44.2) |
18 (35.3) |
12 (23.1) |
23 (50.0) |
25 (49.0) |
|
|
60+ |
121 (48.0) |
11 (21.2) |
31 (60.8) |
39 (75.0) |
22 (47.8) |
18 (35.3) |
|
|
Gender |
|
|
|
|
|
|
0.010* |
|
Male |
114 (45.2) |
26 (50.0) |
17 (33.3) |
33 (63.5) |
21 (45.7) |
17 (33.3) |
|
|
Female |
138 (54.8%) |
26 (50.0) |
34 (66.7) |
19 (36.5) |
25 (54.3) |
34 (66.7) |
|
|
Body mass index |
|
|
|
|
|
|
0.036* |
|
Normal weight |
59 (23.4) |
21 (40.4) |
12 (23.5) |
13 (25.0) |
7 (15.2) |
6 (11.8) |
|
|
Overweight |
88 (34.9) |
18 (34.6) |
15 (29.4) |
17 (32.7) |
17 (37.0) |
21 (41.2) |
|
|
Obese |
105 (41.7) |
13 (25.0) |
24 (47.1) |
22 (42.3) |
22 (47.8) |
24 (47.1) |
|
Data are shown as number (N) and percentage (%); $: Exact probability test, * P < 0.05 ,ND: None diabetic; D w/o C: Diabetic without complications ;Diabetic with diabetic nephropathy (DN); Diabetic with diabetic peripheral neuropathy (DPN); Diabetic with diabetic retinopathy (DR)
Table 2 shows that high density lipoprotein (HDL) was significantly different among DN and DPN groups compared with non-diabetic group, moreover significant differences was found between DN group and DR group (P=0.001). Low-density lipoprotein (LDL) was significantly lower among DN group compared with non-diabetic and DR group (P=0.001). Serum Triglycerides (TG) was significantly higher among diabetic patients with no complications than among non-diabetic group also DN showed significantly higher levels than control group (P=0.009).
Table 2: Lipid profile among study group (N= 252).
|
Parameter |
Groups |
p-value |
||||
|
ND |
D w/o C |
DN |
DPN |
DR |
||
|
(Mean ± SD) |
||||||
|
HDL (mmol/L) |
(1.24± 0.34) |
(1.12± 0.26) |
(0.97 ae± 0.25) |
(1.06 a± 0.28) |
(1.17± 0.28) |
0.001* |
|
LDL (mmol/L) |
(3.16± 0.74) |
(2.40 a± 1.03) |
(2.22 ae± 0.69) |
(2.45 a± 0.78) |
(2.86± 1.43) |
0.001* |
|
Total cholesterol(mmol/L) |
(4.62± 0.97) |
(4.08 ± 1.24) |
(6.03 ± 16.71) |
(4.20± 1.32) |
(4.39± 1.12) |
0.709 |
|
Triglycerides (mmol/L) |
(1.22± 0.71) |
(1.85 a± 0.98) |
(1.78 a± 1.17) |
(1.61± 0.73) |
(1.65± 0.81) |
0.009* |
Data are shown as mean ± Standard Deviation.;HDL: high-density lipoprotein; LDL: low-density lipoprotein; ND: None diabetic; D w/o C: Diabetic without complications ;DN: Diabetic with diabetic nephropathy; DPN: Diabetic with diabetic peripheral neuropathy; DR: Diabetic with diabetic retinopathy ; Significant difference with non diabetic group,Significant difference with diabetic with no complication group,Significant difference with diabetic with nephropathy group,Significant difference with diabetic with neuropathy group and Significant difference with diabatic with retinopathy group.; * P < 0.05.
Table 3 shows that vitamin D deficiency was widespread among DPN group followed by DN , DR and the least among diabetics without complications (78.3%,75%,56.9%, 31.4% ,respectively) with recorded statistical significance (P=0.001). According to Figure 1, vitamin D deficiency was higher among of diabetics with complications (69.8%) compared to diabetics with no complications (31.4%). On the other hand, 39.2% of diabetics with no complications showed normal vitamin D level compared to 13.4% of diabetic patients with complications (P=0.001).
Table 3: Vitamin D Status among study group (N= 252).
|
Vitamin D level |
Total |
Group |
p-value |
||||
|
Non diabetic a |
Diabetics with no complications b |
Diabetic with nephropathy b |
Diabetic with neuropathy d |
Diabetic with retinopathy e |
|||
|
No (%) |
|||||||
|
Deficiency |
154 (61.1) |
34 (65.4) |
16 (31.4) |
39 (75.0) |
36 (78.3) |
29 (56.9) |
0.001* |
|
Insufficiency |
50 (19.8) |
10 (19.2) |
15 (29.4) |
6 (11.5) |
6 (13.0) |
13 (25.5) |
|
|
Normal |
48 (19.0) |
8 (15.4) |
20 (39.2) |
7 (13.5) |
4 (8.7) |
9(17.6) |
|
|
(Mean ± SD) |
(49.4 ± 45.5) |
(46.9 ± 58.1) |
(74.4 ± 62.9 acd) |
(39.4 ± 24.9) |
(33.9 ± 25.3) |
(51.3 ± 28.1) |
0.001*£ |
Data are shown as number (N) and percentage (%) and mean ± Standard Deviation; ND: None diabetic; D w/o C: Diabetic without complications ;DN: Diabetic with diabetic nephropathy; DPN: Diabetic with diabetic peripheral neuropathy; DR: Diabetic with diabetic retinopathy ;Significant difference with non diabetic group,Significant difference with diabetic with no complication group,Significant difference with diabetic with nephropathy group,Significant difference with diabetic with neuropathy group, and Significant difference with diabatic with retinopathy group.;P: Pearson X2 test; £: One Way ANOVA test;* P < 0.05..
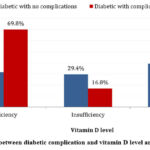 |
Figure 1: Association between diabetic complication and vitamin D level among diabetic patients. |
Table 4 demonstrates that among diabetic patients with no complications, 33.3% of patients with age 40 -59 years old exhibited vitamin D deficiency compared to 80% of those with diabetic complications. Moreover 29% of patients aged 60 and above in diabetic with no complications had vitamin D deficiency compared to 65.8% in diabetic with complications. For gender, vitamin D deficiency was reported among 80.3% of males compared to 60.3% of females in diabetic patients with complications (P=0.012), while in diabetic with no complications, it was reported in 35.3% of males compared to 29.4% females. Regarding BMI, 65.5% of overweight patients, and 72.1% of obese in the diabetic with complications had vitamin D deficiency compared to 40% and 33.3% in diabetic with no complications.
Table 4: Factors related with vitamin D level among diabetic patients and diabetic complications (N= 252)
|
Group |
Personal data |
Vitamin D level |
P value |
||
|
Deficiency |
Insufficiency |
Normal |
|||
|
No (%) |
No (%) |
No (%) |
|||
|
Diabetic with no complications |
Age in years |
|
0.836 |
||
|
< 40 |
1 (50) |
1 (50) |
0 (0) |
||
|
40-59 |
6 (33.3) |
5 (27.8) |
7 (38.9) |
||
|
60+ |
9 (29) |
9 (29.0) |
13 (41.9) |
||
|
Gender |
0.894 |
||||
|
Male |
6 (35.3) |
5 (29.4) |
6 (35.3) |
||
|
Female |
10 (29.4) |
10 (29.4) |
14 (41.2) |
||
|
BMI |
0.027* |
||||
|
Normal weight |
2 (16.7) |
8 (66.7) |
2 (16.7) |
||
|
Overweight |
6 (40) |
3 (20) |
6 (40) |
||
|
Obese |
8 (33.3) |
4 (16.7) |
12 (50) |
||
|
Diabetic with complications |
Age in years |
0.049* |
|||
|
< 40 |
4 (40) |
4 (40) |
2 (20.0) |
||
|
40-59 |
48 (80) |
8 (13.3) |
4 (6.7) |
||
|
60+ |
52 (65.8) |
13 (16.5) |
14 (17.7) |
||
|
Gender |
0.012* |
||||
|
Male |
57 (80.3) |
10 (14.1) |
4 (5.6) |
||
|
Female |
47 (60.3) |
15 (19.2) |
16 (20.5) |
||
|
BMI |
0.251 |
||||
|
Normal weight |
19 (73.1) |
3 (11.5) |
4 (15.4) |
||
|
Overweight |
36 (65.5) |
14 (25.5) |
5 (9.1) |
||
|
Obese |
49 (72.1) |
8 (11.8) |
11 (16.2) |
||
Data are shown as number (N) and percentage (%);BMI: body mass index;* P < 0.05 ; ND: None diabetic; D w/o C: Diabetic without complications ;Diabetic with diabetic nephropathy (DN); Diabetic with diabetic peripheral neuropathy (DPN); Diabetic with diabetic retinopathy (DR)
Discussions
The association between vitamin D deficiency and diabetic microvascular complications has been documented. The current study revealed that diabetic patients with complications had vitamin D deficiency compared to diabetic patients with no complications (69.8% versus 31.4%). A cross-sectional study documented a link between the prevalence and severity of microvascular complications in T2DM and vitamin D levels 14. Additionally, Japanese study on patients with T2DM showed an inverse, significant relationship between microvascular complications and vitamin D levels 15. 39.2% of diabetic patients with no complications showed normal vitamin D level compared to 13.4% of diabetic patients with complications (P=0.001). According to earlier studies, vitamin D deficiency and poor control of diabetes may exacerbate microvascular complications 14,15,13.
In the present study vitamin D deficiency was significantly associated with DPN, DN and DR, and there was a significant differences in the vitamin D levels compared to non-diabetic group with recorded statistical significance (P=0.001). Moreover, epidemiological studies reported significant relationship between diabetic microangiopathy and low vitamin D level 16. The association between low level of vitamin D and the prevalence of diabetes and impaired glucose tolerance have been documented by many studies 17,18. Based on these data, the highest level of vitamin D deficiency was found among patients with DPN compared to other groups with recorded statistical significance (P=0.001). The association of DPN with vitamin D deficiency in diabetic patients could be explained by different mechanisms . It is possible that it could be due to the role of vitamin D deficiency in the pathogenesis of T2DM through altering β-cell function, affecting plasma calcium, insulin resistance and stimulation of acute-phase proteins resulting in blood vessels inflammation19. A recent study stated that vitamin D deficiency is significantly associated with DPN, and that the association is independent of potential confounders (e.g duration of diabetes, hemoglobin, HbA1c and LDL levels) 20. Additionally vitamin D level of DN group were close to the level of vitamin D in DPN group. This result found to be similar with another study 21. The impact of vitamin D on DN has been attributed to that vitamin D deficiency stimulate myocardial hypertrophy and renin secretion 22. Another study showed that vitamin D reduce levels of transforming growth factor-β and proteins, thus protecting the kidneys 23.
Due to the different subjects’ characteristics many risk factors could contribute to vitamin D deficiency. This study showed that among diabetic group with no complications, 33.3% of obese patients had vitamin D deficiency compared to group with normal weight. It could be due to decrease bioavailability of vitamin D3 from skin and its deposition in body lipid 24. In addition, a cross-sectional study has reported the impact of an increase one unit in the BMI, cholesterol, LDL, HDL, and Fast Blood Glucose (FBS) increased liability of Vitamin D deficiency 25. A retrospective review stated the alarming association of vitamin D deficiency with weight 26. In the current study vitamin D deficiency was reported among 65.8% of patients aged 60 years or more compared to 40% of patients less than 40 years. Elderly people have less outdoor activities and therefore less sunlight exposure. In addition, the alteration in organ functions affect vitamin D 27. Previous studies reported that females were more susceptible to vitamin D deficiency compared to males 25. However, in this study males were more deficient in vitamin D compared to females. Consistent with our finding another study reported that mean vitamin D levels in males were significantly higher than fenales 27.
Conclusion
Vitamin D deficiency was more prevalent among diabetics with complications compared to diabetics without complications. Many factors influenced vitamin D levels e.g vitamin D deficiency was more prevalent in males than females. Regarding age, the prevalence of vitamin D deficiency was higher in patients aged 60 years or more than in those less than 40 years. Moreover the prevalence of vitamin D deficiency in obese patients was detected as highest among DPN versus diabetics with no complications. Therefore attention should be paid to link between vitamin D level and diabetic complications. Additional prospective studies are needed to evaluate the effect of vitamin D on diabetic complications.
Conflict of Interest
There is no conflict of interest.
Funding Sources
There are no funding sources.
References
- Contreras-Bolívar V, García-Fontana B, García-Fontana C, Muñoz-Torres M. Mechanisms involved in the relationship between vitamin D and insulin resistance: impact on clinical practice. Nutrients. 2021 Oct;13(10):3491.
CrossRef - Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Inmayo clinic proceedings 2010 Aug 1 (Vol. 85, No. 8, pp. 752-758). Elsevier.
CrossRef - National Institutes of Health. Office of Dietary Supplements. Vitamin D. Fact Sheet for Consumers [Internetas]. Nih. gov. 2016.
- Al-Daghri NM, Hussain SD, Ansari MG, Khattak MN, Aljohani N, Al-Saleh Y, Al-Harbi MY, Sabico S, Alokail MS. Decreasing prevalence of vitamin D deficiency in the central region of Saudi Arabia (2008-2017). The Journal of Steroid Biochemistry and Molecular Biology. 2021 Sep 1;212:105920.
CrossRef - Sultan S, Taimuri U, Basnan SA, Ai-Orabi WK, Awadallah A, Almowald F, Hazazi A. Low vitamin D and its association with cognitive impairment and dementia. Journal of aging research. 2020 Apr 30;2020.
CrossRef - American Diabetes Association. “2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2018.” Diabetes care 41. Supplement_1 (2018): S13-S27.
CrossRef - Meo, Sultan Ayoub. “Prevalence and future prediction of type 2 diabetes mellitus in the Kingdom of Saudi Arabia: A systematic review of published studies.” JPMA. The Journal of the Pakistan Medical Association 66.6 (2016): 722-725.
- AlRuthia, Yazed, et al. “The status of licensed pharmacy workforce in Saudi Arabia: a 2030 economic vision perspective.” Human resources for health 16.1 (2018): 1-8.
CrossRef - Fowler, Michael J. “Microvascular and macrovascular complications of diabetes.” Clinical diabetes 26.2 (2008): 77-82.
CrossRef - Susan van, Dieren, et al. “The global burden of diabetes and its complications: an emerging pandemic.” European Journal of Cardiovascular Prevention & Rehabilitation 17.1_suppl (2010): s3-s8.
CrossRef - Alcubierre, Nuria, et al. “Vitamin D deficiency is associated with poorer satisfaction with diabetes-related treatment and quality of life in patients with type 2 diabetes: a cross-sectional study.” Health and quality of life outcomes 16.1 (2018): 1-8.
CrossRef - Angellotti, Edith, and Anastassios G. Pittas. “The role of vitamin D in the prevention of type 2 diabetes: to D or not to D?” Endocrinology 158.7 (2017): 2013-2021.
CrossRef - Darraj, Hussain, et al. “Vitamin D deficiency and glycemic control among patients with type 2 diabetes mellitus in Jazan City, Saudi Arabia.” Diabetes, metabolic syndrome and obesity: targets and therapy 12 (2019): 853.
CrossRef - Zhao, W.-J., Xia, X.-Y., & Yin, J. (2021). Relationship of serum vitamin D levels with diabetic microvascular complications in patients with type 2 diabetes mellitus. Chinese Medical Journal, 134(7), 814–820.
CrossRef - Suzuki, A., Kotake, M., Ono, Y., Kato, T., Oda, N., Hayakawa, N., Hashimoto, S., & Itoh, M. (2006). Hypovitaminosis D in type 2 diabetes mellitus: Association with microvascular complications and type of treatment. Endocrine Journal, 53(4), 503–510.
CrossRef - Patrick PA, Visintainer PF, Shi Q, et al. Vitamin D and retinopathy in adults with diabetes mellitus. Arch Ophthalmol 2012;130:756–60.
CrossRef - Pietschmann, P., Schernthaner, G., & Woloszczuk, W. (1988). Serum osteocalcin levels in diabetes mellitus: analysis of the type of diabetes and microvascular complications. Diabetologia, 31(12), 892–895.
CrossRef - Isaia, G. C., Ardissone, P., Di Stefano, M., Ferrari, D., Martina, V., Porta, M., Tagliabue, M., & Molinatti, G. M. (1999). Bone metabolism in type 2 diabetes mellitus. Acta diabetologica, 36(1-2), 35–38.
CrossRef - Palomer, X., González-Clemente, J. M., Blanco-Vaca, F., & Mauricio, D. (2008). Role of vitamin D in the pathogenesis of type 2 diabetes mellitus. Diabetes, obesity & metabolism, 10(3), 185–197.
CrossRef - Shehab, D., Al-Jarallah, K., Mojiminiyi, O., Al Mohamedy, H., & Abdella, N. (2011). Does Vitamin D deficiency play a role in peripheral neuropathy in Type 2 diabetes?. Diabetic Medicine, 29(1), 43-49.
CrossRef - Xiao, X., Wang, Y., Hou, Y., Han, F., Ren, J., & Hu, Z. (2016). Vitamin D deficiency and related risk factors in patients with diabetic nephropathy. The Journal of international medical research, 44(3), 673–684.
CrossRef - Mozos, I., & Marginean, O. (2015). Links between Vitamin D Deficiency and Cardiovascular Diseases. BioMed research international, 2015, 109275.
CrossRef - Romero-Aroca, P., Baget-Bernaldiz, M., Reyes-Torres, J., Fernandez-Ballart, J., Plana-Gil, N., Mendez-Marin, I., & Pareja-Rios, A. (2012). Relationship between diabetic retinopathy, microalbuminuria and overt nephropathy, and twenty-year incidence follow-up of a sample of type 1 diabetic patients. Journal of diabetes and its complications, 26(6), 506–512.
CrossRef - Wortsman, J., Matsuoka, L. Y., Chen, T. C., Lu, Z., & Holick, M. F. (2000). Decreased bioavailability of vitamin D in obesity. The American journal of clinical nutrition, 72(3), 690–693.
CrossRef - Alloubani, A., Akhu-Zaheya, L., Samara, R., Abdulhafiz, I., Saleh, A., & Altowijri, A. (2019). Relationship between Vitamin D Deficiency, Diabetes, and Obesity. Diabetes & metabolic syndrome, 13(2), 1457–1461.
CrossRef - Alfawaz, H., Tamim, H., Alharbi, S., Aljaser, S., & Tamimi, W. (2014). Vitamin D status among patients visiting a tertiary care center in Riyadh, Saudi Arabia: a retrospective review of 3475 cases. BMC public health, 14, 159.
CrossRef - Hidayat, R., Setiati, S., & Soewondo, P. (2010). The association between vitamin D deficiency and type 2 diabetes mellitus in elderly patients. Acta medica Indonesiana, 42(3), 123–129.

