
Manuscript accepted on :23-03-2021
Published online on: 31-03-2021
Plagiarism Check: Yes
Reviewed by: Dr. B.Surendiran
Second Review by: Dr. Ankur Singh Bist
Final Approval by: Dr. Beatrice O. Ondondo
Mahmoud H. Alkhasawneh1* , Asma’a Al-Mnayyis2 and Yazeed Bagain3
, Asma’a Al-Mnayyis2 and Yazeed Bagain3
1Division of Radiology, Faculty of Medicine, Mutah University, Alkarak, Jordan.
2Department of Clinical Sciences, Faculty of Medicine, Yarmouk University, Jordan.
3Department of Radiology, Al-Karak Governmental Hospital -Jordanian ministry of health Jordan.
Corresponding Author E-mail: mahmoudalkasawneh@yahoo.com
DOI : https://dx.doi.org/10.13005/bpj/2149
Abstract
Magnetic resonance imaging (MRI) is the golden standard technique for spine disc disease diagnosis. Vertebral body endplate signal intensity on MRI is confirming lumber spine degenerative disc disease.The study aimed to record the lumbar spine degenerative relation between disc and diseaseusing magnetic resonance imaging. Our prospective and double blind investigation included 142 participants,having lumbar spine degenerativedisease confirmed by MRI. Pfirrmann score was used to record the relation between lumbar spine disc degeneration and lumbar spine degenerative disease. Modic modifications with the Pfirrmann and modified Pfirrmann scores of disc degeneration were assessed.Lumbar spine MRI was done for all participants using sagittal T1 and T2 WI. Modic was scored (0-III) The Pfirrmann scored I-V for disc degeneration. Lumbar disc degeneration was evaluated by modified Pfirrmann scoring from 1-8 according to signal intensity of the nucleus pulposus and inner annulus.Modic was recorded in 41.5%, 24.6%, 32.4% and 1.4% of participants with scores 0, I, II and III, respectively. Pfirrmann score was 13.4%, 73.9% and 12.7% of disc degeneration with scores III, IV and V, respectively, while,the modified Pfirrmann score was 2.1%, 15.5%, 38.7%, 26.8% and 16.9% of disc degeneration with scores of 4, 5, 6, 7 and 8, respectively. The modified Pfirrmann score showed notableinconsistencyin participants with Modic 0, I and II, but no difference between Modic I and II.There was significant relation between Modicand lumbar spine disc degeneration. In conclusion, there is a relation between Modic, Pfirrmann and modified Pfirrmann scores of lumbar spine disc degeneration in participants with lumbar spine degenerative disease.
Keywords
Degeneration; Disc; Disease; Lumbar; Modic; Modified Pfirrmann; Pfirrmann
Download this article as:| Copy the following to cite this article: Alkhasawneh M. H, Al-Mnayyis A, Bagain Y. Spinal Degeneration and Degenerative Disc Disease correlation identified with Magnetic Resonance Imaging. Biomed Pharmacol J 2021;14(1). |
| Copy the following to cite this URL: Alkhasawneh M. H, Al-Mnayyis A, Bagain Y. Spinal Degeneration and Degenerative Disc Disease correlation identified with Magnetic Resonance Imaging. Biomed Pharmacol J 2021;14(1). Available from: https://bit.ly/3rFAYah |
Introduction
MRI is considered the golden standard in the diagnosis of spine disc problems. Degenerative disc induces deprivation of water, proteoglycans, and collagen type II locally which can be seen on MRI. The inability to bind water for preventing dehydration is due to loss of proteoglycans, hence, the signal intensity of disc can be seen on MRI. The noticed vertebral body endplate signal intensity on MRI (Modic) is confirming degenerative disc disease1.Modic 0 is the normal picture, I is bone marrow edema and inflammation, II is fat instead of normal hemopoietic bone marrow and III issubchondral bone sclerosis (2).
There is a strong correlation between Modic and disc degeneration intensity1, 3.Endplate degeneration is associated with lumbar disc degeneration1. The aim of the present was to find therelation between lumbar spine degenerative disc and disease with MRI.
Methods
142 participants [55 men (38.7%) and 87 women (61.3%)] were enrolled in this prospective and double blind study, aged 41-65 years having lumbar spine degenerative disease confirmed using MRI.The study was performed at Alkarak teaching hospital, Ministry of health in Jordan during the period between 2016-2019, afterobtainingapproval from the Ethical and ResearchBoardReviewcommittees.
Lumbar spine disc degeneration was assessed using the Pfirrmann score. The relation between lumbar spine disc degeneration and lumbar spine degenerative disease was recorded by MRI according to the Pfirrmann score. Modic modifications with the Pfirrmann and modified Pfirrmann scores of disc degeneration were assessed. The association between Modicand disc degeneration of lumbar disc degenerative disease was recorded according to Pfirrmann and the modified Pfirrmann scores. The correlation between the Pfirrmann and the modified Pfirrmann scores of Modic 0, I, and II was assessed. Modic relation with disc degeneration was recorded.
All participants were examined by MRI for lumbar spine using sagittal T1 and T2 WI. Modic was scored as; 0: normal; I:newvascular endplate was hyperintense on T2WI and hypointense on T1WI; II:fat endplate was hyperintense on T1WI and isointense or hypointense on T2WI; III: endplate bone sclerosis was hypointense on T1 and T2 WI.Lumbar disc scoring was done in the sagittal T2WI1, 2.The Pfirrmann score determines degenerated spinal discs by MRI for inequality in disc building, differentiation between the nucleus and the annulus, signal intensity of spinal discs and scoring I-V for disc degeneration. Lumbar disc degeneration was evaluated by the modified Pfirrmannscore4 ,scoring 1-8 for disc degeneration according to signal intensity of the nucleus pulposus and inner annulus and signal intensity discrepancybetween the inner and outer of the posterior annulus.
Statistics
Data were analyzed by theKruskal-Wallis test.Association within Modic and disc degeneration was evaluated using binary logistic regression.P values less than 0.05 were considered statistically significant.
Results
Lumber endplate Modicwas positive in 58.5% (83/142) of the patients, 35/142 (24.6%), 46/142 (32.4%) and two patients/142 (1.5%) in Modic I, II and III, respectively (Figures 1, 2 and 3), while, Modic 0 disc degeneration was recorded in 59 patients (41.5%). (Table I). Disc degeneration was recorded at L2/3 (5; 6.1%), L3/4 (6; 7.2%), L4/5 (46; 55.4%) and L5/S1 (26; 31.3%).
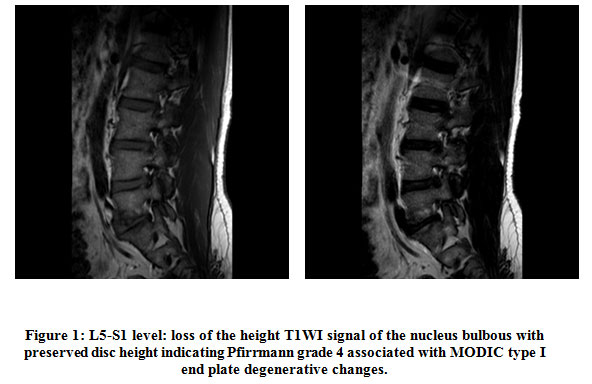 |
Figure 1: L5-S1 level: loss of the height T1WI signal of the nucleus bulbous with preserved disc height indicating Pfirrmann grade 4 associated with MODIC type I end plate degenerative changes. |
Table 1: Modic score.
| Degenerative lumbar disc disease | |
| Modic | Overall |
| I | 35(24.6%) |
| II | 46(32.4%) |
| III | 2(1.5%) |
| Overall | 83(58.5%) |
Regarding Pfirrmann score of vertebral degenerative disease,the patients were 19/142 (13.4%), 105/142 (73.9%)and 18/142 (12.7%) with scoresIII, IV and V of disc degeneration but there were no patients with score I or II disc degeneration. Table II. Regarding modified Pfirrmann score;the patients were 3/142 (2.1%), 22/142 (15.5%), 55/142 (38.7%), 38/142 (26.8%), 24/142 (16,9%) with scores4, 5, 6, 7 and 8 disc degeneration, but there were no patients with score of 1,2 or 3 disc degeneration.Table II.
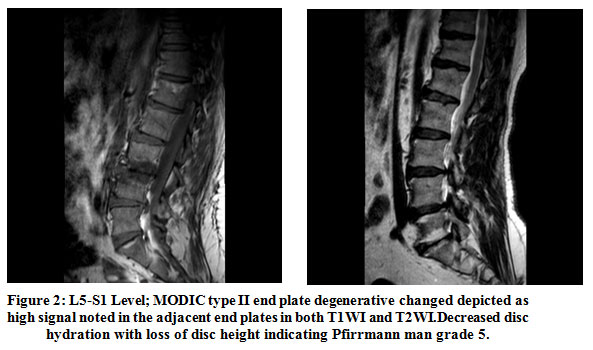 |
Figure 2: L5-S1 Level; MODIC type II end plate degenerative changed depicted as high signal noted in the adjacent end plates in both T1WI and T2WI. Decreased disc hydration with loss of disc height indicating Pfirrmann man grade 5. |
Table 2: Pfirrmannand modified Pfirrmannscores.
| Degenerative lumbar disc disease | |||
| Pfirrmann score | Overall | Modified Pfirrmann | Overall |
| I | 0 | 1 | 0 |
| II | 0 | 2 | 0 |
| III | 19(13.4%) | 3 | 0 |
| IV | 105(73.9%) | 4 | 3(2.1%) |
| V | 18(12.7%) | 5 | 22(15.5%) |
| Overall | 142(100%) | 6 | 55(38.7%) |
| 7 | 38(26.8%) | ||
| 8 | 24(16.9%) | ||
| Overall | 142(100%) | ||
Table 3: Modic and Pfirrmann scores.
| Modic | |||||
| Pfirrmann score | 0 | I | II | III | Overall |
| I | ——- | ———- | ———- | ———– | ———— |
| II | ———— | ———— | ———– | ————- | ————– |
| III | 15(10.6%) | 3(2.1%) | 1(0.7%) | ————- | 19(13.4%) |
| IV | 40(28.2%) | 25(17.6%) | 39(27.5%) | 1(0.7%) | 105(73.9%) |
| V | 4(2.8%) | 7(4.9%) | 6(4.2%) | 1(0.7%) | 18(12.7%) |
| Overall | 59(41.5%) | 35(24.6%) | 46(32.4%) | 2(1.5%) | 142(100%) |
Modic IIIwas recorded in 2 patients (1.5%) with modified Pfirrmann score of IV. P <0.05. Modic 0, I and II demonstrated remarkable discrepancy in Pfirrmann score (P<0.05). Table III-IV. Modichad the most association with disc degeneration.There was remarkable discrepancy regarding modified Pfirrmann score in participants with Modic 0, I and II (P<0.05), hence there was no remarkable discrepancy between Modic I and II (P>0.05).There was remarkable relation between Modic and lumbar spine disc degeneration.
Table 4: Modic and Modified Pfirrmann score.
|
Modic |
|||||
| Modified Pfirrmann score | 0 | I | II | III | Overall |
| 1 | ———- | ————– | —————- | ————– | ———– |
| 2 | ————- | ————– | —————- | ————— | ————- |
| 3 | ————— | ————— | ————– | ————— | ————– |
| 4 | 3(2.1%) | ———— | ———– | ————- | 3(2.1%) |
| 5 | 15(10.6%) | ———— | 7(4.9%) | ————– | 22(15.5%) |
| 6 | 29(20.4%) | 14(9.9%) | 11(7.7%) | 1(0.7%) | 55(38.7%) |
| 7 | 7(4.9%) | 11(7.7%) | 20(14.1%) | ———— | 38(26.8%) |
| 8 | 5(3.5%) | 10(7.04%) | 8(5.6%) | 1(0.7%) | 24(16.9%) |
| Overall | 59(41.5%) | 35(24.6%) | 46(32.4%) | 2(1.5%) | 142(100%) |
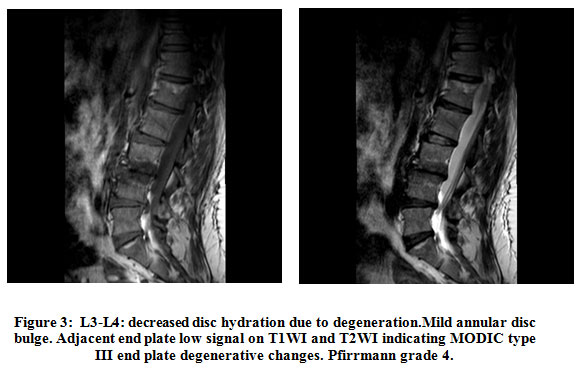 |
Figure 3: L3-L4: decreased disc hydration due to degeneration.Mild annular disc bulge. Adjacent end plate low signal on T1WI and T2WI indicating MODIC type III end plate degenerative changes. Pfirrmann grade 4. |
Discussion
MRI is the most important approach in assessing the pathology of intervertebral disc clinically. In the degenerated intervertebral disc, the loss of collagens, water and proteoglycans can be visualized using MRI with hypointense signal (T2 weighting).On MRI, changes in signal intensity at body endplate have been successfully applied in the diagnosis of lumber spine spondylosis and degenerative disc disease1.The association between the intensity, the degree of lumbar disc degeneration and Modic changes (signal intensity changes at vertebral endplate) had been reported3, also, a strong correlation between degeneration & tear of lumber disc degeneration with the degeneration of endplate was found4. Addionlly, the changes in signal intensity were detected in degenerative lumber disc disease patients in the adjacent endplates5.Now, the identified Modic changes are three types, on MRI, the changes in type I appear hypointense (T2W1)characterizing the local inflammation and edema of bone marrow, type II changes (T1W1) is hyperintense and (T2W1) isointense or slightly hyperintense representing the replacement of normal hemopoietic bone marrow, type III Modic changes is hypointense on T1W1 and T2W1 which characterizes the sclerosis of subchondral bone, while, Modic change type 0 is an indicator for the presence of normal anatomy6.
In our study, endplate signal intensity in degenerative lumbar disc disease was assessed and the link between Modic and disc degeneration was determined. The obtained results revealed that 58.5% of patients experienced Modic changes in endplate in MRI; 24.6% of and 32.4% of patients experienced types I and II endplate Modic changes, respectively, type III Modic change is less frequent than the Modic change types I and II. In Pfirrmannscores study,there were 13.4%, 73.9%, and 12.7% of the patients with scores III,V and V, respectively. Regarding the modified Pfirrmann score,the patients were 2.1%, 15.5%, 38.%, 26.8%and 16.9%of the patients with scores 4, 5, 6, 7 and 8 disc degeneration, respectively, both scores showed notable difference in Modic 0, 1 and II, the observed difference between Pfirrmann and the modified Pfirrmann scoring may be due to the insensitivity of Pfirrmann one to the degree of the degeneration of disc, so, the modified Pfirrmann scoring system is preferable in the differentiation of disc degeneration severity7.
Our obtained results are nearly in agreement with the results reported in the study of Li-Peng et al. in their study, the abnormalities in endplate were detected in 60% of the patients, one quarter and one third of themhad types I and II Modic changes1. Also, the analysis of results for Pfirrmann scorefor lumber disc degeneration of their patients, it was revealed that 12.96%, 75% and 12.03% with scores III, IV and V of the patients, respectively, but none was in scores and I and II, for the modified Pfirrmann scoresthe results showed 1.85%, 14.82%, 39.81%, 29.63% and 8 13.89% with scores 4, 5, 6, 7and 8 but none was I the scores 1 to 31, which is also inaccordance with our results
The findings in the present study propose the severity of lumber disc degeneration among our patients when compared to the results in other studies 3, 4, 6. The incidence of endplate Modic changes was 19% up to 59% of the degenerative lumber disc disease patients with more frequency of types I and II and less frequently type III change8. Other studies showed that Modic change type II about 90% (8), while, it was 19.5% and 84% for type I Modic change3.
Regarding the incidence of Modic changes types I and II, the difference between our results and those reported by Jensen et al.3 could be attributed to the study population in their study which was consisted of lumber disc degeneration patients in mild condition and clinically normal subjects.
It was believed that the changes in Modic type I were due endplate disruption, angiogenesis and formation of connective tissues which corresponded to the process of degeneration, the change accompanying type II Modic was the prolonged degeneration of red bone marrow, then, its replacement with yellow marrow, while, Modic type III was a characterof the process oflumber disc degenerative sclerosis9. Pro-inflammatory mediators such as interleukins 6 and 8 were detected as a result of insistentinjuries in lumber disc which could be considered as the main cause of back pain in the lumber region10, also it could be contributed to the high levels of TNFα and PGP 9.5 in endplates with Modic I changes due to nerve and inflammatory cells growth induction by TNFα11or due to edema under endplatecartilage12. The genetic factors, the nutritional factors and the physical pressure applied to the intervertebral space cannot be ignored as predisposing factors for Modic changes13, also, it was evidenced that there is an association between low back pain in the lumber region and other factors including intrinsic shape phenotypes and quality of life14.
The preset prospective study has few limitations including the findings of MRI should give further convincing results, the relatively small sample size and little findings of some MRI, so, supplementary study is inevitable for generalizing the results of the study.
Conclusion
Modic modifications are found in 60% of participants with degenerative disc disease and are related to disc degeneration. Evaluation of Modic modifications, Pfirrmannand modified Pfirrmannscores might detect disc degeneration early. This modified Pfirrmann scoring system more reliable, and preferable to be used in distinguishing the severity of disc degeneration.
Acknowledgement
Mahmoud H. Alkhasawneh- Concepts of ideas, literature search, experimental studies, data acquisition, manuscript preparation and editing Asma’a Al-Mnayyis- Manuscript preparation, editing and revision, Experimental studies, data acquisition YazeedBagain – Design, data analysis, statistical analysis, manuscript revision.
conflict of Interest
The authors declare that there are no conflicts of interest
Funding Sourse
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
References
- Li-PengY,Wen-Wu Q,Guo-Yong Y,etal.MRI assessment of lumbar intervertebral disc degeneration with lumbar degenerative disease using the Pfirrmann grading systems.PLOS One., 2012;7(12):e48074.
CrossRef - Long X,ChunlinN.I,JiandongS.H.I,et al .Analysis of Correlation Between Vertebral Endplate Change and Lumbar Disc Degeneration.international medical journal of experimental and clinical research., 2017,23:4932-8).
CrossRef - Jensen T.S, Kjaer P, Korsholm L, et al.. Predictors of new vertebral endplate signal (Modic) changes in the general population. Eur Spine., J 2010;19: 129–35.
CrossRef - Kokkonen S.M, Kurunlahti M, TervonenO, Ilkko E, Vanharanta H. Endplate degeneration observed on magnetic resonance imaging of the lumbarspine: correlation with pain provocation and disc changes observed on computed tomography diskography. Spine., 2002;27: 2274–2278.
CrossRef - de Roos A, Kressel H, Spritzer C, Dalinka M. MR Imaging of marrowchanges adjacent to end plates in degenerative lumbar disk disease. AJR.,1987;149:531–534.
CrossRef - Marshman L. A, Trewhella M, Friesem T, Bhatia C. K, Krishna M. Reverse transformation of Modic type 2 changes to Modic type 1 changes during sustained chronic low-back pain severity: report of two cases and review of the literature. J Neurosurg Spine., 2007;6:152–155.
CrossRef - Griffith J. F, Wang Y. X, Antonio G.,E, et al. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration.Spine., 2007;32: 708–12.
CrossRef - Toyone T, Takahashi K, Kitahara H, Yamagata M, Murakami M, et al.Vertebral bone marrow changes in degenerative lumbar disc disease: an MRIstudy of 74 patients with low back pain. J Bone Joint Surg Br., 1994;76: 757–764.
CrossRef - Modic M. T, Steinberg P. M, Ross J. S, Masaryk, Carter J. R. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology., 1988;166: 193–199.
CrossRef - Burke J. G, Watson R. W, McCormack D, Dowling F. E, Walsh M. G, et al. Intervertebral discs which cause low back pain secrete high levels ofproinflammatory mediators. J Bone Joint Surg Br., 2002;84: 196–201.
CrossRef - Ohtori S, Inoue G, Ito T, Koshi T, Ozawa T, et al. Tumor necrosisfactor-immunoreactive cells and PGP 9.5-immunoreactive nerve fibers invertebral endplates of patients with discogenic low back pain and Modic type1 or type 2 changes on MRI. Spine.,2006;31: 1026–1031.
CrossRef - Vital J. M, Gille O, Pointillart V, Pedram M, Bacon P, et al. Course ofModic 1 six months after lumbar posterior osteosynthesis. Spine.,2003;28: 715–721.
CrossRef - Jensen R. K, Leboeuf-Yde C. Is the presence of modic changes associatedwith the outcomes of different treatments? A systematic critical review. BMC MusculoskeletDisord., 2011;12: 183.
CrossRef - Janet AD, AnastasiaVP, LimAKP, et al .Is intrinsic lumbar spine shape associated with lumbar disc degeneration? An exploratory study.BMC Musculoskeletal Disorders., 2020;21:433.
CrossRef

