
Manuscript accepted on :13-May-2019
Published online on: 17-06-2019
Plagiarism Check: Yes
Reviewed by: Abdalbasit Al-Ubaidi
Second Review by: Priestly Shan
Arshia Ummat1, Sreejeeta Dey1, Anupama Nayak P1, Nitin Joseph2, Ashwin Rao1 and Karuna Y. M1
1Department of Paedodontics and Preventive Dentistry, Manipal College of Dental Sciences, Mangalore, Manipal Academy of Higher education, Manipal, Light house hill road- 575001, India.
2Department of Community Medicine, Kasturba Medical College, Mangalore Manipal Academy of Higher Education, Manipal, Light house hill road- 575001, India.
Corresponding Author E-mail: anupama.np@manipal.edu
DOI : https://dx.doi.org/10.13005/bpj/1716
Abstract
Dental fear and anxiety (DFA) serves as significant problem in child patient management as it leads to greater prevalence and increased severity of the disease associated with delayed dental visits. Therefore, it is necessary to effectively predict children dental behaviour and identify children at risk of Behaviour Management problems. Study of factors influencing DFA and its association with behaviour in children during first dental visit. The study included 209 children (5-14 years). DFA levels were assessed using 3 standardised questionnaires i.e. Facial Image Scale (FIS), Dental Anxiety Scale (DAS), Children’s Fear Survey Schedule – Dental Subscale (CFSS-DS). The behaviour of the child was then assessed using Frankl’s Behaviour Rating Scale (FBRS). The data were analysed, and a correlation was established between DFA and behaviour using statistical analysis. Presence of DFA according to FIS is 13.4%, according to DAS is 15.2% and according to CFSS-DS is 17.7%. Maximum participants showed positive behaviour (81.8%) according to FBRS. Factors causing maximum Dental anxiety according to DAS was anticipation of treatment (26.30%) and factor which caused maximum dental fear according to CFSS-DS was injections (45.4%). There is association between DFA and behaviour in children during first dental visit. This study will help assess the factors which lead to dental fear and anxiety in children and also find a correlation between dental fear and anxiety and behaviour management problems which can help the Paedodontist to predict various behaviour management problems and to avoid the factors which lead to them before the initiation of the dental treatment. This can lead to a decrease in the fear and anxiety levels of children which will further lead to better treatment and in turn better case management.
Keywords
Behaviour Rating Scale; Child Behavior; Dental Anxiety; Dental Care; Problem Behavior; Surveys and Questionnaires
Download this article as:| Copy the following to cite this article: Ummat A, Dey S, Nayak A. P, Joseph N, Rao A, Karuna Y. M. Association Between Dental Fear and Anxiety and Behavior Amongst Children During Their Dental Visit. Biomed Pharmacol J 2019;12(2). |
| Copy the following to cite this URL: Ummat A, Dey S, Nayak A. P, Joseph N, Rao A, Karuna Y. M. Association Between Dental Fear and Anxiety and Behavior Amongst Children During Their Dental Visit. Biomed Pharmacol J 2019;12(2). https://bit.ly/2ZvkSm4 |
Introduction
Dental fear and anxiety serve as a consequential problem in pedodontic patient management1,2. Dental fear is a normal emotional response or reaction to one or more specific threatening stimuli during or prior to a dental treatment1. On the contrary, dental anxiety is indicative of apprehension that something bad will occur in relation to the dental treatment. Both dental fear and anxiety initiates mostly during childhood and persist through adolescence and can have a major influence towards the provision of dental services and tends to decrease as child grows older3. According to previous studies children with dental fear and anxiety present with various behavior management problems associated with dental treatment4. Thus, the provision of dental care may become time consuming, expensive and taxing for both the child and the dentist.
Evaluating a child’s level of dental fear and anxiety before commencing the actual dental treatment can help reduce the behavior management problems associated with it and can make the dental visit a more fruitful4. Also, identifying which factors lead to or trigger dental fear and anxiety is important to take necessary steps to attenuate the same and to implement an appropriate behavior management technique.
Therefore, it is necessary to predict negative dental behavior amongst children and identify the children at risk5.
The present study was aimed to identify factors influencing dental fear and anxiety and its association with behavior management problems in children aged 5- 14 years during the dental visit. The null hypothesis for the study was set as, there will not be any association between dental fear and anxiety and behavior management problems in children during first dental visit using facial image scale, CFSS- DS, Dental anxiety scale and Frankl’s behavior rating scale.
Materials and Method
The study was initiated after approval from Institutional Ethics Committee. This was a cross sectional study carried out in children aged between 5-14 years in the Department of Paedodontics and Preventive Dentistry. The sample size calculated was 209 to achieve 95% confidence interval, 20% relative precision and 80% power. The sample selection was done by simple random sampling method and were later divided into four groups based on their age:
Group 1: 6 years and less
Group 2: 7-8 years
Group 3: 8-11 years
Group 4: More than 11 years d
The inclusion criteria for the study were as follows: 1) Healthy children visiting the dental clinic with their parent 2) Accompanying parent/ guardian was one of the child’s primary caretakers 3) Children indicated for procedures like restorative fillings, dental extractions, preventive pit and fissure sealant application and topical fluoride application 4) Children aged 5 -14 years 5) Both male and female gender the dentist had no previous connection with child or guardian 6) The child was able to understand and reply to our questions.1,4,6
Children with mental disabilities and easily discernible mental disorders or children with dental emergencies such as trauma, acute pulpitis, periapical abscess, and acute periapical periodontitis etc. were excluded from the study.1,4
When the patient along with their guardian/parent arrived at the clinic, the aim of the study was briefed to them in their language at the waiting area and their consent was taken without affecting the dental care procedure given to the child. An operator elicited each child’s background variables using standardized questionnaires. The study consisted of three sets of questionnaires of fear and anxiety scales- Facial Image Scale (FIS), Dental Anxiety scale (DAS) and Children’s Fear Survey Schedule –Dental Subscale (CFSS-DS)
At first FIS score was recorded. FIS comprises of a row of five faces from very happy (1) to very unhappy (5). The child was asked to point at the facial image which best describes his mental state.7
The child was then asked to fill, or was interviewed by the investigator, on the DAS questionnaire which is a four-question format with answers ranging from low anxiety level (<9) to severe anxiety level (15-20).8,9
Thereafter, the DFA levels were assessed by applying the CFSS-DS which is a 15‑question form with a five‑point response scale from 1 ‑ “not afraid at all” to 5 ‑ “very afraid.” Total score thus ranged from 15 to 75. The cut off score is 38 for the presence of dental fear. Here also, the child was asked to complete the questionnaire or if the child was incapable to do so the investigator interviewed the child to assist him/her to do the same.10
All the above questionnaires were translated into the common language for better understanding. After collection of all the questionnaires, the child is escorted into the clinic for dental treatment.
The behavior of the child during dental treatment was directly rated using Frankel’s Behavior Rating Scale FBRS as-
Definitely Negative (Rating 1)
Refusal of treatment or crying forcefully or fearful, or any other overt evidence of extreme negativism.
Negative (Rating 2)
Reluctant to accept treatment or uncooperative or some evidence of negative attitude but not pronounced (sullen, withdrawn).
Positive (Rating 3)
Acceptance of treatment or at times cautious or willingness to comply with the dentist or at times with reservation but patient follows the dentist’s directions cooperatively.
Definitely Positive (Rating 4)
Good rapport with the dentist or interested in the dental procedures or laughing and enjoying.5
The questionnaires were then collected from the participants. Answers were reviewed and analyzed and a correlation was determined between dental fear and anxiety and behavior using suitable statistical analysis. 4
Statistical Analysis
The data analysis was completed using SPSS version 16. The statistical tests applied were Karl Pearson’s Coefficient of Correlation test, Chi Square test, Unpaired t test, Analysis Of Variance. p value <0.05 was taken as cut off to assess statistical significance.
Results
The study was conducted amongst 209 children among which 103 (49.3%) were males and 106 (50.7%) were females. Internal consistency and reliability of all the questionnaires (FIS, DAS AND CFSS-DS) were assessed using Chronbach’s alpha coefficient. Alpha values > 0.70 were considered satisfactory. Chronbach’s alpha coefficient was calculated to be 0.811 which indicated high reliability.
According to Facial image scale (FIS) maximum respondents (51.2%) showed a score 2 i.e. happy as seen in table 1. 12.4% children depicted the presence of dental fear by scoring 4 (unhappy) and 5 (very unhappy) in the FIS. There is a statistically significant association seen between the FIS scores and the different age groups taken into consideration (p value = 0.0324) using Pearsons chi square test as seen in table 2. There was no significant association seen between gender and FIS scores computed using both student’s t test and Pearsons chi square test (p value = 0.376).
According to Dental Anxiety Scale (DAS) maximum respondents (55%) showed mild anxiety (score < 9). 15.2% respondents showed high to severe anxiety by scoring between 13 and 20 in DAS. There is a statistically significant between the various age groups taken into consideration and dental anxiety (p value = 0.0091) according to Pearson’s chi square test as seen in table 3. However, there is no significant relation seen between gender and DAS scores (P value = 0.490) according to both student’s t test and Pearson’s chi square test. The factor which contributed the most to dental anxiety was ‘anticipation of treatment’ (waiting for treatment outside the dental office) i.e. 26.30 % followed by ‘waiting in the dental chair while the dentist gets the drill ready for treatment’ i.e. 14.30% as seen in figure 1.
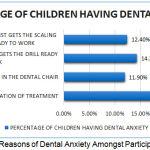 |
Figure 1: Distribution of Reasons of Dental Anxiety Amongst Participants.
|
This figure depicts that the factor which contributed the most to dental anxiety was ‘anticipation of treatment’ (waiting for treatment outside the dental office) i.e. 26.30 % followed by ‘waiting in the dental chair while the dentist gets the drill ready for treatment’ i.e. 14.30%.
According to Children’s Fear Survey Schedule – Dental Subscale (CFSS-DS) 17.7% respondents displayed the presence of dental fear i.e. score > 38 as shown in table 4. There was no statistically significant relationship seen between age groups taken into consideration and dental fear according to CFSS-DS scores according to Pearson’s chi square test (P value= 0.600) and one-way ANOVA (f value = 0.625). There was also no significant relationship seen between gender and dental fear according to CFSS-DS scores according to Pearson’s chi square test (p value = 0.118). The factor which caused maximum fear amongst children according to CFSS-DS was INJECTIONS (45.4%) followed by having to open their mouth (18.6%) and the dentist drilling (14.4%) as seen in figure 2.
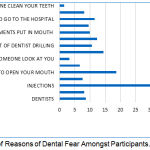 |
Figure 2: Distribution of Reasons of Dental Fear Amongst Participants.
|
This figure depicts that the factor which caused maximum fear amongst children according to CFSS-DS was injections (45.4%) followed by having to open their mouth (18.6%) and the dentist drilling (14.4%)
A correlation was determined between Frankel’s Behavior Rating Scale (FBRS) scores and Dental Anxiety Scale (DAS) scores using Karl Pearson’s Coefficient of Correlation test. A negative correlation was determined between the same (P value = 0.001) as seen in table 4. A correlation was also determined between Frankel’s Behavior Rating Scale (FBRS) scores and Children’s Fear Survey Schedule – Dental Subscale (CFSS-DS) scores using Karl Pearson’s Coefficient of Correlation test. A negative correlation was determined between the same (P value = 0.001) as seen in table 5.
Discussion
The study was aimed at identifying children with dental fear and anxiety (DFA) and the factors responsible for causing them. As it is an extremely common barrier in the completion of paediatric dental treatment and causes adverse consequences to the patient’s oral and psychological health.1,11 Access to dental care is often intervened by presence of dental fear and anxiety amongst children which in turn leads to delayed dental visits.12
Since one questionnaire is never a hundred percent accurate in assessing DFA levels, a set of three standard questionnaires were used to assess the DFA levels in children for better accuracy and results were correlated with the behavior of the child.13 The three scales used in this study were Facial Image Scale (FIS), Dental Anxiety Scale (DAS) and Children’s Fear Survey Schedule- Dental Subscale (CFSS-DS). FIS is a series of five facial images which serves as a quick and useful tool for assessment of DFA. 7 CFSS-DS is one of the most used survey instrumental in assessing DFA levels.10 According to the study conducted by Bajrice et al, it has an excellent internal consistency and presence of two-dimensional concept of DFA in children.14 DAS serves as a reliable, valid and useful tool for the measurement of dental anxiety amongst children in the dental clinic.15
Many behavior rating scales are present in the field of paediatric dentistry. Frankl et al classified child’s dental behavior into four classes according to the attitude and cooperation of the child. It is one of the most reliable tools developed for behavior rating in the paediatric dental setting.5
The presence of dental fear according to FIS was 13.4% i.e. 28 respondents showed presence of dental fear. Maximum respondents had a score of 2 i.e. HAPPY (51.2%). There was a statistically significant difference between FIS scores amongst different age groups taken into consideration. As the age of the child increases the level of dental fear decreases. This may be due to the development of better understanding in older children. 1 There was no statistically significant difference between distribution of dental fear between males and females. Almost the same level of fear was present in both genders. This was against the findings specified in the study done by Rajwar and Goswami where the levels were more in females than in males.1
According to DAS maximum respondents had mild anxiety (55%). There is a statistically significant relationship between the different age groups and anxiety levels shown. This portrays that as the age increases the levels of dental anxiety decreases significantly, due to better cognitive understanding of the surrounding dental environment and setting. The gender although does not have a significant relation with anxiety level of the child.
CFSS-DS was also recorded for all children. CFSS-DS level >38 was considered as a positive parameter for the presence of dental fear.16 82.3% children fell under the low fear group. No statistically significant relation was found between age or gender and CFSS-DS scores. The maximum mean score was present in children between 7-8 years of age (29.08±9.395) but it was a statistically insignificant increase. This was in accordance with the study conducted by Rajwar and Goswami.1 A higher mean scores were seen in males than females (29.21 ± 11.015). This however is not in accordance to the study done by them, where the presence of dental fear was more in females than males.1
On correlating FBRS scores and DAS scores a significant negative correlation was obtained i.e. as the child became more anxious (higher DAS score) the FBRS score turned more negative which revealed that the child showed uncooperative and negative behavior. Similarly, a negative correlation was seen between CFSS-DS scores and FBRS scores i.e. as a child became fore fearful, the FBRS scores turned more negative and the child displayed more negative behavior. On assessment of various factors which cause dental anxiety, ‘anticipation of treatment while the child waited in the dental office’ (26.3%) followed by ‘waiting in the dental chair while the dentist got the drill ready for treatment’ (14.30%) were the factors which caused maximum dental anxiety in children.
Factors which caused maximum fear where ‘injection’ (45.44%) followed by ‘having to open their mouth’ (18.6%) and ‘dentist drilling’ (14.4%) dominated. This was in accordance to the studies conducted by Rajwar and Goswami 1, Nakai et al 17 and Domoto et al.18
Thus, using the results of this study the child’s behavior can be understood better and appropriate behavior management strategies can be thought of and applied to minimize dental fear and anxiety amongst children. There is still need for further research for understanding the fears and behavior of children and adolescents alike.
Table 1: Frequency and Percentage of Facial Image Scale Scores.
| SCORE | Frequency | Valid Percent | Cumulative Percent | |
| 1 | Very happy | 35 | 16.7 | 16.7 |
| 2 | Happy | 107 | 51.2 | 67.9 |
| 3 | Neutral | 39 | 18.7 | 86.6 |
| 4 | Unhappy | 23 | 11.0 | 97.6 |
| 5 | Very unhappy | 5 | 2.4 | 100.0 |
| Total | 209 | 100.0 | ||
This table depicts the frequency and distribution of facial image scale scores. The maximum respondents had a score 2 or Happy whereas 13.4% respondents showed a score of 3 and 4 i.e. Unhappy And Very Unhappy which showed the presence of dental fear and anxiety.
Table 2: Association Between Age Groups and Fis.
| Very Happy | Happy | Neutral | Unhappy | Very Unhappy | ||
| 6 Years and Less | 8 9.71% |
31 29.69% |
11 10.82% |
7 6.38% |
1 1.39% |
58 |
| 7-8 Years | 5 8.71% |
27 26.62% |
7 9.70% |
9 5.72% |
4 1.24% |
52 |
| 9 Years and More | 22 16.58% |
49 50.68% |
21 18.47% |
7 10.89% |
0 2.37% |
99 |
| Total | 35 | 107 | 39 | 23 | 5 | 209 |
(χ2 = 16.785, df = 8, χ2/df = 2.10, P = 0.0324)
This table depicts the association between the age groups taken into consideration and the facial image scores. As the age of the child increased the level of dental fear and anxiety decreased significantly.
Table 3: Association Between Various Age Groups and Dental Anxiety.
|
Age Group |
DAS | ||||||
| Mild Anxiety | Moderate Anxiety | High Anxiety | Severe Anxiety | Total | |||
| 6 years and less | Count | 28 | 21 | 3 | 6 | 58 | |
| % within age group | 48.3% | 36.2% | 5.2% | 10.3% | 100.0% | ||
| 7-8 years | Count | 22 | 16 | 8 | 6 | 52 | |
| % within age group | 42.3% | 30.8% | 15.4% | 11.5% | 100.0% | ||
| 9-10 years | Count | 21 | 16 | 3 | 1 | 41 | |
| % within age group | 51.2% | 39.0% | 7.3% | 2.4% | 100.0% | ||
| 11 years and above | Count | 44 | 9 | 3 | 2 | 58 | |
| % within age group | 75.9% | 15.5% | 5.2% | 3.4% | 100.0% | ||
|
Total |
Count | 115 | 62 | 17 | 15 | 209 | |
| % within age group | 55.0% | 29.7% | 8.1% | 7.2% | 100.0% | ||
χ2 = 21.916, df = 9, χ2/df = 2.44, P (χ2 > 21.916) = 0.0091.
This table depicts the association between various age groups taken into consideration and dental anxiety. As the age of the child increased the level of dental anxiety according to the Dental Anxiety Scale reduced significantly.
Table 4: Correlation Between FBRS Score and Dental Anxiety Scores.
| Mean | Std. Deviation | N | |
| FBRS | 2.85 | .757 | 209 |
| Total Das | 8.44 | 3.786 | 209 |
This table depicts a significant correlation between the Frankl’s behavior rating scale scores and Dental anxiety scale scores. As the level of dental anxiety increased the behavior of the child became more negative.
Table 5: Correlation Between FBRS Score and CFSS-DS Scores.
| Mean | Std. Deviation | N | |
| CFSS-DS | 27.99 | 10.336 | 209 |
| FBRS | 2.85 | .757 | 209 |
This table depicts a significant correlation between the Frankl’s behavior rating scale scores and Children’s Fear Survey Schedule – Dental Subscale (CFSS-DS) scores. As the level of dental anxiety increased the behavior of the child became more negative.
Conclusion
From the results obtained above it was found out that as the dental fear and anxiety of the child increased, the behavior became more negative. This was influenced by many factors such as age, anticipation of treatment, fear of injections, fear of a drill. These factors can be used to effectively identify the child’s dental behavior which in turn can help in reducing the dental fear and anxiety amongst them.
Clinical Significance
This study will help assess the factors which lead to dental fear and anxiety in children during a dental visit and also find a correlation between dental fear and anxiety and behavior management problems which can help the Paedodontist to predict various behavior management problems and to avoid the factors which lead to dental fear and anxiety before the initiation of the dental treatment. This can lead to a decrease in the fear and anxiety levels of children which will further lead to a better treatment and in turn better case management.
Acknowledgements
The author(s) received no specific funding for this work.
Conflict of Interest
There is no conflict of interest.
Funding Sources
The authors received no specific funding for this work
References
- Rajwar AS, Goswami M. Prevalence of dental fear and its causes using three measurement scales among children in New Delhi. J Indian SocPedodPrev Dent 2017;35:128-33.
- Shinde SD, Hegde RJ. Evaluation of the influence of parental anxiety on children’s behavior and understanding children’s dental anxiety after sequential dental visits. Indian J Dent Res 2017;28:22-6
- Boka, K. Arapostathis, V. Karagiannis, N. Kotsanos, C. van Lovere, J. Veerkamp. Dental fear and caries in 6-12 year old children in Greece. Determination of dental fear cut-off points. European Journal of Paediatric Dentistry 2017;18: 45- 50.
- Sharma A, Kumar D, Anand A, Mittal V, Singh A, Aggarwal N. Factors predicting Behavior Management Problems during Initial Dental Examination in Children Aged 2 to 8 Years. Int J ClinPediatr Dent 2017;10(1):5-9.
- Sharma A, Tyagi R. Behavior Assessment of Children in Dental Settings: A Retrospective Study.Int J ClinPediatr Dent. 2011; 35-39.
- Pai R, Mandroli P, Benni D, Pujar P. Prospective analysis of factors associated with dental behavior management problems, in children aged 7-11 years. J Indian SocPedodPrev Dent 2015;33:312-8.
- Muthu M, Sivakumar N. Pediatric dentistry. 2nd ed. Noida: Elsevier; 2009.
- Corah NL. Development of a dental anxiety scale. J Dent Res1969; 48: 596.
- Norman Corah’s Dental Questionnaire [Internet]. www.dentalfearcentral.org. 2017 [cited16October2017].Available from: http://www.dentalfearcentral.org/media/dental_anxiety_scale.pdf.
- Curthbert, MS Barbara, G Melamed, and Ph Da screening device: children at risk for dental fear and management problems. Journal of dentistry for children 1982:432-4.
- Sunil Raj, Manisha Agarwal, Kiran Aradhya, Sapna Konde, V Nagakishore. Evaluation of Dental Fear in Children during Dental Visit using Children’s Fear Survey Schedule-Dental Subscale. Int J Clin Pediatr Dent. 2013; 6(1):12-15.
- Chellappah N, Vignehsa H, Milgrom P, Lam L. Prevalence of dental anxiety and fear in children in Singapore. Community Dentistry and Oral Epidemiology. 1990;18(5):269-271.
- Schuurs A, Hoogstraten J. Appraisal of dental anxiety and fear questionnaires: a review. Community Dentistry and Oral Epidemiology. 1993;21(6):329-339.
- Bajric E, Kobaslija S, Huseinbegovic A, SelimovicDragas M, Muratbegovic A, Markovic N. Reliability and Validity of the Modified Version of Children’s Fear Survey Schedule-Dental Subscale in 9-12 Years Old Schoolchildren in Bosnia and Herzegovina. Medical Archives. 2018;72(3):192.
- Corah N, Gale E, Illig S. Assessment of a dental anxiety scale. The Journal of the American Dental Association. 1978;97(5):816-81.
- Singh P, Pandey R, Nagar A, Dutt K. Reliability and factor analysis of children′s fear survey schedule-dental subscale in Indian subjects. Journal of Indian Society of Paedodontics and Preventive Dentistry. 2010;28(3):151.
- Nakai Y, Hirakawa T, Milgrom P, Coolidge T, Heima M, Mori Y et al. The Children’s Fear Survey Schedule-Dental Subscale in Japan. Community Dentistry and Oral Epidemiology. 2005;33(3):196-204.
- Domoto P, Weinstein P, Melnick S, Ohmura M, Uchida H, Ohmachi K et al. Results of a dental fear survey in Japan: implications for dental public health in Asia. Community Dentistry and Oral Epidemiology. 1988;16(4):199-201.

