
Manuscript accepted on :06-Mar-2019
Published online on: 15-03-2019
Plagiarism Check: Yes
Reviewed by: Nicolas Padilla
Second Review by: Satheesha Nayak B.
Final Approval by: Dr. Javad Sharifi-Rad
Kumaresan M*1 , Sangeetha A2, Vijayakumar J1, Yuvaraj Maria Francis1, Siva T3 and Balaji K1
, Sangeetha A2, Vijayakumar J1, Yuvaraj Maria Francis1, Siva T3 and Balaji K1
1Department of Anatomy, Saveetha Medical College Hospital, Thandalam, Chennai India.
2Department of Physiology, Saveetha Medical College Hospital, Thandalam, Chennai India.
3Department of Anatomy, Sri Ramachandra Medical College and research institute, Chennai, India.
Corresponding Author E-mail: kumaresan1204@gmail.com
DOI : https://dx.doi.org/10.13005/bpj/1657
Abstract
The renal artery when it reaches close to the hilum of kidney where it cleaves into anterior and posterior divisions were receives around 75% and 25% of blood respectively. Further these branches divide into many segmental branches. These segmental arteries does not have collateral system, so when there is any occlusion of these arteries which results in the ischemia of the particular segment of kidney. Anatomists believe that knowledge of presence of lower polar artery is essential for polar nephrectomy. Prior knowledge of variations in the renal vessels is required for urological surgery for preoperative investigations as there are reports of surgical complications which include enormus haemorrhage. In this study we analyzed the different variations in the intra renal branch of inferior segmental artery.
Keywords
CT Angiogram; Inferior Segmental Artery; Kidney Donors; Nephrectomy; Renal Artery
Download this article as:| Copy the following to cite this article: Kumaresan M, Sangeetha A, Vijayakumar J, Francis Y. M, Siva T, Balaji K. Analysis of Intra Renal Arterial Pattern in Kidney Donors using 64-Slice Computed Tomography Angiography. Biomed Pharmacol J 2019;12(1). |
| Copy the following to cite this URL: Kumaresan M, Sangeetha A, Vijayakumar J, Francis Y. M, Siva T, Balaji K. Analysis of Intra Renal Arterial Pattern in Kidney Donors using 64-Slice Computed Tomography Angiography. Biomed Pharmacol J 2019;12(1). Available from: https://bit.ly/2W2VLFs |
Introduction
The renal artery is one of the lateral branches of abdominal aorta, as it reaches closer to the kidney it splits into anterior and posterior division were it receives around 75% and 25% of blood respectively. Further these branches divide into many segmental branches. These segmental arteries does not have collateral system, so when there is any occlusion of these arteries which results in the ischemia of the particular segment of kidney.1If lower polar accessory renal artery is present in the infant, it should be noted to be in close relation to main renal artery and not to ureter.
In later part of life the poles of kidney are separated from the main artery in such a case it could obstruct the ureter.2 Interestingly, a recent study result tells the reality about the galactosemia patients should be monitored for anomalies of renal vessels.3 Anatomists believe that precise knowledge of presence of lower polar artery is essential for polar nephrectomy. Prior awareness of anomalous of renal artery is needed for the urologist in preoperative findings as there are reports surgical complications which enormous haemorrhage.4 There are very less reports of additional renal artery to poles of kidney. Arrival of renal artery into the kidney other than usual route is considered as infrequent findings.5 The entire accessibility rate for inferior segmental artery rate was 88.5% from an anterior and 66.7% from a posterior surgical approach.6,7,8 This present study is to analyze the intra renal arterial pattern of inferior segmental artery in kidney donors. This study results not only gives information to intra-renal surgeries but also for renal transplantation.
Materials and Methods
In this study 99 CT angiogram images were analyzed in work station of specialized scan centre in Chennai after getting approval from the Institutional Human Ethics Committee, Saveetha Medical College – IHEC No. 001/09/2015/IEC/SU.The CT machine used was light speed VCTXTe, ADW 4.5 Version, 64 slice Computed Tomography Angiography. The study group was drawn from kidney donors who approached the scan center had no diseases related to kidney. Out of 99 donors there were 54male, and 45 were female. Inferior segmental branch of renal artery is classified into four types depending upon the mode of its origin [kher et al]. They are
Type I
Inferior segmental branch arises from the anterior division of renal artery.
Type II
Inferior segmental branch arises from the posterior division of renal artery.
Type III
Inferior segmental branch emerges from the main renal artery.
Type IV
Inferior segmental branch arises either above or below the main renal artery from aorta.
Observation and Results
Percentage of occurrence of pattern of origin of inferior segmental artery is given below. Among the 99 donors (198 kidneys), type 1 is seen in 66 kidneys on both sides, type 2 is seen in 6 kidneys on right side and 3 on left side, type 3 is seen around in 11 kidneys on right and 12 on left, type 4 is seen in 12 kidneys on right side and 13 on left side. Other patterns are seen in 4 kidneys on right and 5 on left side. In few kidneys we found an inferior segmental artery emerges from common iliac and middle segmental branch of renal artery.
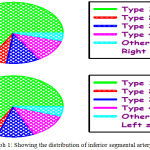 |
Graph 1: Showing the distribution of inferior segmental artery.
|
There is no association between the pattern of inferior segmental branch between right and left side, χ2 = 1.195; P = 0.879.
Discussion
This present work reported that the inferior segmental artery type 1 arises from anterior division of renal artery found to be more frequent which is similar to previous studies by servo et al9 reported in 47% of cases, Raghavendra et al10 reported in 51.66%, Chandra Girish et al11 reported in 59% of cases and Fine H et al12 study not observed the type 1 inferior segmental artery. Results obtained in our study shows different percentage in compare to other results (Table 2).
Table 1
| Pattern | Right | Left | ||
| Male (n=54) | Female(n=45) | Male(n=54) | Female(n=45) | |
| Type 1 | 37 (68.5%) | 29 (64.4%) | 37 (68.5%) | 29 (64.4%) |
| Type 2 | 4 (7.4%) | 2 (4.4%) | 3 (5.5%) | Nil |
| Type 3 | 5 (9.2%) | 6 (13.3%) | 6 (11.1%) | 6 (13.3%) |
| Type 4 | 6 (11.1%) | 6 (13.3%) | 5 (9.2%) | 8 (17.7%) |
| Others | 2 (3.7%) | 2 (4.4%) | 3 (5.5%) | 2 (4.4%) |
Values given in parenthesis are percentage. Statistical values are given in the below chart.
Table 2: Comparison of inferior segmental branch with previous workers.
| Type | Verma et al 1961 | Raghavendra et al 2007 | Chandra Girish et al 2014 | Present study 2018 |
| Kidneys studied | 98 | 60 | 100 | 198 |
| Type I | 88% | 51.66% | 59% | 66.6% |
| Type II | 1.02% | 8.33% | 6% | 4.5% |
| Type III | 3.06% | 10% | 28% | 11.6% |
| Type IV | – | 28.33% | 2% | 12.6% |
| Other pattern | – | – | – | 4.5% |
And this is the only angiographic study to find out the variations in inferior branch of renal artery in live donors, so compare to the previous study the results shows great significance. We also compared not only the variations in the sides but we found the gender differences. In this current study, type I and type II are more frequent in male on both sides whereas Type III and IV are more frequent in female on both sides. There is no association within the pattern of inferior segmental branch of renal artery between right and left side c2 = 1.195; P = 0.879. The presence of accessory lower polar artery prevail as the kidneys ascend upwards they are nourished by a succession of momentary aortic sprouts that emerge at gradually higher levels. Such arteries will not elongate to follow the ascending kidney but instead dissipated and are replaced by recent arteries. The final pair of arteries forms in the lumbar region and becomes the definitive renal arteries. Rarely, a inferior pair of arteries persistent as additional inferior polar arteries. Additional renal arteries can emerge from the abdominal aorta aloft the main branch or as low (inferiorly) as the internal iliac artery.13 Diverse origins may be from ventral branches of abdominal aorta such as, celiac, superior and inferior mesenteric and also from middle colic, lumbar, middle sacral and opposite side renal arteries have been reported.14
 |
Figure 1: Showing the classification of Inferior Segmental artery depending upon its origin.
|
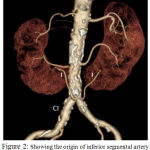 |
Figure 2: Showing the origin of inferior segmental artery from common iliac artery.
|
The presence of such anomalies may be important from the academic, anthropological and radiological point of view.15
Conclusion
The precise knowledge of intra renal arterial branches will provide a informative benefaction for surgeons in performing more conservative renal surgeries like partial and segmental resection of renal tissue instead of going for comprehensive nephrectomy.
Acknowledgements
I thank the Department of Anatomy, Saveetha Medical College and Hospital.
Conflict of Interest
There is no conflict of interest.
References
- Mc Dougal., Wein A., Kavoussi L., Novick A., Partin A., Peters C., Campbell-Walsh U. 10th ed, saunder elseiver. 2012;602-605.
- Stewart H. H. A new operation for the treatment of hydronephrosis in association with a lower pole (or aberrant artery). B.J.S. 1947;35:51-57.
- Mizoguchi N., Sakura N., Ono H., Naito K., Hamakawa M. Congenital porto-left renal venous shunt as a cause of galactosemia. J Inherit Metab Dis. 2001;24(1):72-78.
CrossRef - Toda R., Iguro Y., Moriyama Y., Hisashi Y., Masuda H., Sakata R. Double left renal vein associated with abdominal aortic aneurysm. Ann Thoracic cardio vasc surg. 2001;24(1):72-78.
- Gesase A. P. Rare origin of supernumerary renal vessels supplying the lower pole of the kidney. Ann Anat. 2007;189(1):53-58.
CrossRef - Weld K. J., Bhayani S. B., Belani J., Ames C. D., Hruby G., Landman J. Extrarenal vascular anatomy of kidney: Assessment of variations and their relevance to partial nephrectomy Urology. 2005;66(5):985-989.
CrossRef - Kher G. A., Bhargava I., Makhni F. S. Intrarenal branching of the renal artery. Ind J of Surg. 1960;22:563-79.
- Verma M., Chaturvedin R. P., Pathak R. K. Anatomy of the renal vascular segments. J Anat Soc. 1961;10:12-14.
- Servo V. V. Segmental arterial distribution in the human kidney. J of Urol. 1959;24-26.
- Raghavendra V. P., Manjappa T. Anjana Telkar Renal Apical Segmental Artery Variations and Their Surgical Importance. Journal of Clinical and Diagnostic Research. 2012;6(4):561-563.(Suppl2).
- Chandragirish S., Nanjaiah C. M., Shirur Y .S., Saheb H. S. Study on Variations of Posterior Division of Renal Artery. Int J Anat Res. 2014;2(4):709-11. ISSN 2321-4287.
- Fine H and Keen E. N. The arteries of the human kidney. J. Anat. 1966;100(4):881-894.
- Boijsen E Anomalies and malformations. In: Abrams HL Abrams angiography, 2nd edn. Little, Brown, Boston. 1983;1217-1221.
- Cuttino J. T., Clark R. L The normal vasculature of the genitourinary tract: embryology anatomy and hemodynamics. In: Hillman B. J. Clinical urography, Saunders, Philadelphia. 3:2076-2091.
- Pa Pa Hlaing K., Das S., Sulaiman M. I.,Latiff A. A., Ghafar A. N.,Suhaimi H. F. Accessory renal vessels at the upper and lower pole of the kidney a cadaveric study with clinical implications. Bratisl Lek Listy. 2010;111(5):308-10.

