
Manuscript accepted on :October 11, 2016
Published online on: --
Plagiarism Check: Yes
Behroz Barati and Mahboobe Asadi
Faculty of medicine, Department of otolaryngology and head and neck surgery, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
DOI : https://dx.doi.org/10.13005/bpj/1063
Abstract
Mastoid osteomas are rare asymptomaticlesion. When symptomsare present, surgical resection is the treatment of choice.Case report: The authors report a case of mastoid osteoma in a 56-year old woman. Computed tomography performed because of a retroauricular mass identified a large osteoma of the mastoid. Surgery carried out because of conductive hearing loss.Results: conductive hearing loss is an indication for surgical management of mastoid osteoma.Conclusion: mastoid osteoma is rare and surgery indicated in symptomatic cases.
Keywords
osteoma; mastoid
Download this article as:| Copy the following to cite this article: Barati B, Asadi M. Mastoid Osteoma: Report of an Unusual Case. Biomed Pharmacol J 2016;9(3). |
| Copy the following to cite this URL: Barati B, Asadi M. Mastoid Osteoma: Report of an Unusual Case. Biomed Pharmacol J 2016;9(3). Available from: http://biomedpharmajournal.org/?p=10740 |
Introduction
Osteomas are benign bone tumors of the head and neck that are frequently found in the frontal-ethmoid region.1,2Mastoidosteomas are rareThey are usually asymptomatic , present as a hard, painless, retroauricular mass.3
Even though most mastoid osteomas do not cause significant symptoms, they should be given attention by the Otorhinolaryngologists because they can lead to esthetical alterations and occasionally to functional ones.4
Case reports
A 56 year old female presented with the complaint of right posteriorauricular mass for 15 years. The retro auricular mass was painlesswith a gradual increase in size. There was no history of trauma,symptoms of inflammation but it resulted in right external auditory canal occlusion.Treatment was sought on functional grounds. Examinationrevealed a 2 · 1.5 cm mass over the right mastoid region. Itwas hard, non-tender with no overlying skin changes.
Tympanometry could not be done in right side because of the mass effect. Pure Tone Audiometry showedconductive hearingloss. Temporalcomputed tomography done reported a bony protuberance arisingfrom the right mastoid bone cortexwith slightly extension to external auditory canal(Figure 1). There was no evidence of bonydestruction or infiltration into the mastoid air cells. Middle ear cavity was normal. The visualizedsinuses and mastoid air cells were clear. A diagnosis of benign rightmastoid osteoma was made based on history, examination andradiological findings. This was confirmed by a histopathologicalreport. We proceeded with excision of the mastoidosteomabecause of right side hearing loss due to mass effect (Figure 2).
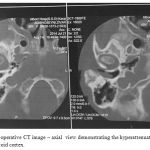 |
Figure 1: Pre-operative CT image – axial view demonstrating the hyperattenuating lesion on the right mastoid cortex. |
 |
Figure 2: The tumour resected |
Discussion
Fibro-osseous tumours such asosteomas are not uncommonbenign, slow-growing neoplasmsarising mainly in thefrontal and ethmoidparanasalsinuses.Osteomas are benign osteoblastictumours of mesenchymal origin.6
In the temporal region, osteomas are essentially reported in the external auditory canal, or more rarely in the middle ear,along the auditory canal or the styloid process, in the temporomandibular joint, in the apex of the petrous temporal bone or in the internal auditory canal.7Osteomaof the mastoid is a rare benign bone-forming tumor composed by bone tissue. It is a slow growing tumor that is kept stable for years. Normally it is asymptomatic, although it may cause cosmetic deformities most of the time.8 itmay produce pain by invasion ofneighbouring structures orwidening of periosteum. The complications are recurrence, facial nerve affection, sigmoid sinus damage and sensorineural hearing loss by nervous compression of inner ear. 2
There arecases in which conducting hearing loss develops due to pushingforward of the posterior canal wall by the mastoid osteoma.9As occurred in our patient. Occlusions of the external ear canal may cause recurrent ear infection.10
The clinical and radiological findings along with histopathologicevidence demonstrate the diagnosis of mastoid osteoma.11Asymptomatic patients can be followed up with observation and monitored with regular imaging.When symptomsare present, surgical resection is the treatment of choice.6thesurgery should include careful removal of periosteal coverand safe margin of the mastoid cortical around it.12Malignant transformation is yet to bereported.13
References
- Probst LE, Shankar L, Fox R. Osteoma of the mastoid bone. J Otolaryngol.1991; 20(3): 228-30.
- Burton DM, Gonzalez C. Mastoid osteomas. Ear Nose Throat J. 1991; 70(3): 161-2.
- Mastoid osteoma: Report of two cases. M. El Fakiri, W. El Bakkouri, C. Halimi, A. Aït Mansour, D. Ayach. European Annals of Otorhinolaryngology, Head and Neck diseases (2011) 128, 266—268.
- Denia A, Perez F, Canalis RR, Graham MD. Extracanalicularosteomas of the temporal bone.Arch Otolaryngol.1979; 105(12): 706-9.
- P. Stre˛k, O. Zagólski, A. Wywiał, E. Osteoma of the sphenoid sinus.Sachaand,M. Pasowicz .B-ENT. 2005, 1, 39-41.
- Parashari UC, Khanduri S, Singh N, Bhadury S. Mastoid osteoma. Indian J Otol. 2014;20:132–133.
- KimCW, Oh SJ, Kang JM, Ahn HY. Multiple osteomas in the middleear.Eur Arch Otorhinolaryngol.2006;263:1151—4.
- Patrícia M. S. TakenakaI; Filomena R. P. PerezII; Sandra J. PatrocínioIII; Juparethan T. RibeiroIV.Mastoidosteoma: report of a case and literature review.Rev. Bras.Otorrinolaringol. vol.70 no.6 São Paulo Nov./Dec. 2004
- Gulia J, Yadav S. Mastoid osteoma: a case report. Internet J HeadNeck Surg. 2008;3(1).
- Cheng Jeffrey, Garcia Roberto, Smouha Eric. Mastoid osteoma: acase report and review of the literature. Ear Nose Throat J. 2013March;92(3):E7.
- Swapan K. Ghosh, SaumyajitDatta, Alok Banka .Osteoma Of The Mastoid – A Case Report, Indian J Otolaryngol Head Neck Surg. 2006 Jul; 58(3): 315–316.
- Gupta OP, Samant IIC. Osteoma of the mastoid.Laryngoscope.1972; 82(2): 172-6.
- Ahmadi Mohammad Saeed, Ahmadi Mohammad, DehghanArash.Osteoid osteoma presenting as a painful solitary skull lesion: a casereport. Iran J Otorhinolaryngol. Apr 2014;26 (75):115–118.

