
Manuscript accepted on :
Published online on: 07-01-2016
Plagiarism Check: Yes
R. Mensudar,* and Muthulingam Vivek
Department of Conservative Dentistry, Sree Balaji Dental College and Hospital, Bharath University, Pallikaranai, Chennai-600100
DOI : https://dx.doi.org/10.13005/bpj/723
Abstract
This case report describes of patient with maxillary anterior spacing, which was treated using a planned sequence of multidisciplinary approach for esthetic treatment. If the spacing is caused by tooth size discrepancy involving one or more teeth then an interdisciplinary treatment plan involving orthodontic, restorative, and periodontal treatment approach is recommended to achieve a harmonious esthetic result. Hence, the aesthetic appearance with a pleasant smile requires an interdisciplinary approach to achieve the treatment goal.
Keywords
smile; spacing; multidisciplinary approach; aesthetic
Download this article as:| Copy the following to cite this article: Mensudar R, Vivek M. Smile Redesigned – A Case Report. Biomed Pharmacol J 2015;8(October Spl Edition) |
| Copy the following to cite this URL: Mensudar R, Vivek M. Smile Redesigned – A Case Report. Biomed Pharmacol J 2015;8(October Spl Edition). Available from: http://biomedpharmajournal.org/?p=3669> |
Introduction
Tooth size discrepancy or uneven spacing between the anterior teeth is a major aesthetic problem for patients. Closure of these interdental spaces using resin composite offer to be a more conservative and practical approach. Direct composite restoration has several distinct advantages, such as conservation of tooth structure, reversibility of procedure, lower cost to patient and relative ease of addition or removal of materials when necessary. The other treatment modalities for treating the anterior spacing includes orthodontic approach or a combination of restorative and prosthodontic treatment method.
Therefore, an interdisciplinary approach that will combine two or more treatment options may be required in order to achieve aesthetically pleasing outcome. This case report describes the treatment of a patient with maxillary anterior spacing due to relapse of orthodontic treatment, which has lead to uneven spacing in the maxillary anterior region.
Case Report:
A 35-year-old female patient came complaining about spacing in the maxillary anterior teeth. On clinical examination, presence of uneven spacing in the maxillary anterior region from right canine to left canine was observed, with slight midline deviation to the right side. The patient’s past dental history reveals maxillary surgery, which was followed by orthodontic treatment for correction of her proclined upper anterior teeth 5 years back. The widest interdental space was between two central incisors, approximately 4 mm and between 11 and 12 spacing is approximately 3 mm. Mild proclination of the upper 11 was also present [FIG Ia, Ib, Ic]. On her first visit, an irreversible hydrocolloid impression of both arches were taken to fabricate the diagnostic cast.
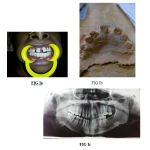 |
Figure 1a, Ib and Ic: Preoperative view, model and OPG. |
The main requirement for the patient was an immediate treatment result due to her personal reason and was neither willing for any orthodontic treatment nor any surgical procedure. Based on the analysis of the patient’s face, tooth size discrepancy and the diagnostic cast, a diagnostic wax-up was made. [FIG II]
 |
Figure 2: Wax mock up |
On the following visit, after thorough consultation and review of the treatment options with the patient, it was decided to perform intentional root canal therapy in 12, 11, 21, and 22 followed by fixed prosthetic replacement. Routine endodontic therapy was carried out. After establishing the working length, the root canals was cleaned and shaped using Universal Protaper rotary system up to F3 for 11 and 21 and F2 for both the laterals (12 & 22). Irrigation was performed with 1 ml of 2.5 % of NaOCl solution. The final irrigation was done with 2% chlorhexidine followed by normal saline. The canal were then obturated using the corresponding size gutta percha points by lateral condensation method with AH Plus sealer. The access cavity was sealed with glass ionomer cement. On her next visit, tooth preparation was done based on the mock wax up preparation made. An utmost care was taken to evenly distribute the interdental space among the anterior region [FIG III]. The final impression was taken for to process the Porcelain fused-metal bridge. Based on the mock preparation, the acrylic bridge was ready and temporization was done on the same day [FIG IV]. The final porcelain fused metal bridge was processed and was luted on her following visit using Type I Glass ionomer cement [FIG V]. It is six months since the treatment is complete and the patient is happy with her present esthetic smile.
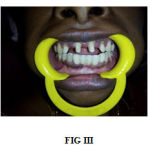 |
Figure 3: Tooth preparation |
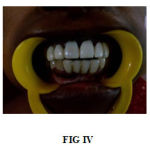 |
Figure 4:Temporization |
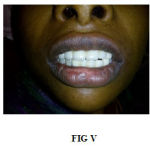 |
Figure 5: Final porcelain fused metal bridge |
Discussion
Treatment modalities in aesthetic cases often involve multidisciplinary approach, such as orthodontic treatment, periodontal evaluation, oral surgery, and restorative or prosthodontics treatment. To achieve the desired aesthetically pleasing treatment, smile analysis is essential. It is six months since the treatment is complete and the patient is happy with the outcome of the treatment through this comprehensive approach. A mock up preparation was done using the dental plaster models, which provided a three-dimensional source data, allowing dentists to examine the occlusion and the relation of the maxillary and mandibular dental arches. A diagnostic wax-up also act as a guideline in restoring the anterior maxillary teeth and aids in achieving a more harmonized space distribution. It also helped in turn to educate the patient and visually see the outcome of the treatment. The cosmetic improvement of the smile is possible with both direct and indirect techniques; the latter procedures might require more than one appointment, but are preferred when multiple teeth are involved in the treatment plan and accurate tooth reshaping or color matching is needed. With indirect technique, a pre-visualization of the final esthetic result is extremely useful both for the clinician and for the patient. In this way, desires and preferences related to the new smile are tested before carrying out irreversible teeth preparations.
The patient exhibited greater confidence with a new smile. Although, the patient is happy and satisfied with the appearance, a better result could have been achieved, if the gingival level of the central incisors also were corrected through periodontal approach. When considering treatment of the maxillary anterior teeth for esthetic purposes, the dentist must consider each case on its own merits. A step-by-step protocol was proposed from diagnostic evaluation, mock-up fabrication and trial, teeth preparation and impression, and adhesive cementation. The resolution of initial esthetic issues, patient’s satisfaction, nice integration of indirect restoration confirmed the success of this anterior dentition rehabilitation. This case report is an example of well-planned sequences of treatment from the beginning till the end of the procedure. By practical treatment approaches used in this case, the dentist was able to manage and obtain the highest result of esthetic and the patient’s demand was also met.
References
- Ittipuriphat I, Leevailoj C. Anterior space management: interdisciplinary concepts. J Esthet Restor Dent. 2013; 25(1):16-30.
- Claman l, Alfaro MA, Mercado A. An interdisciplinary approach for improved esthetic results in the anterior maxilla. J Prosthet Dent. 2003; 89(1):1-5.
- Waldman AB. Smile design for the adolescent patient–interdisciplinary management of anterior tooth size discrepancies. J Calif Dent Assoc 2008; 36(5):365-72.
- Chu CH, Zhang CF, Jin LJ. Treating a maxillary midline diastema in adult patients: a general dentist’s perspective. J Am Dent Assoc 2011; 142(11):1258-64.
- Rosa M, Zachrisson BU. Integrating esthetic dentistry and space closure in patients with missing maxillary lateral incisors. J Clin Orthod. 2001; 35(4):221-34.
- Pena CE, Viotti RG, Dias WR, Santucci E, Rodrigues JA, Reis AF. Esthetic rehabilitation of anterior conoid teeth: comprehensive approach for improved and predictable results. Eur J Esthet Dent. 2009 autumn; 4(3):210-24.
- Gurrea J, Bruguera A. Wax-up and mock-up. A guide for anterior periodontal and restorative treatments. Int J Esthet Dent 2014; 9(2):146-62.
- Mummidi B, Rao CH, Prasanna AL, Vijay M, Reddy KV, Raju MA. Esthetic dentistry in patients with bilaterally missing maxillary lateral incisors: A Multidisciplinary Case Report. J Contemp Dent Pract. 2013; 14(2):348-54.
- Paris JC, Ortet S, Larmy A, Brouillet JL, Faucher AJ. Smile esthetics: A methodology for success in a complex case. Eur J Esthet Dent 2011; 6(1):50-74.

